Double blind, cluster randomised trial of low dose supplementation with vitamin A or βcarotene on mortality related to pregnancy in Nepal
BMJ 1999; 318 doi: https://doi.org/10.1136/bmj.318.7183.570 (Published 27 February 1999) Cite this as: BMJ 1999;318:570
- Keith P West Jr, professor (kwest{at}jhsph.edu)a,
- Joanne Katz, professora,
- Subarna K Khatry, project directorb,
- Steven C LeClerq, esearch associatea,
- Elizabeth K Pradhan, research associatea,
- Sharada R Shrestha, deputy project directorb,
- Paul B Connor, data systems coordinatora,
- Sanu M Dali, project obstetrician- gynaecologistb,
- Parul Christian, assistant scientist,a,
- Ram P Pokhrel, chairmanc,
- Alfred Sommer, dean on behalf of the NNIPS-2 Study Group.a
- aohns Hopkins School of Hygiene and Public Health, Division of Human Nutrition, Room 2041, 615 N Wolfe Street, Baltimore, MD 21205, USA
- bNepal Nutrition Intervention Project-Sarlahi (NNIPS), Nepal Netra Jyoti Sangh, Nepal Eye Hospital Complex, PO Box 335, Tripureswor,Kathmandu, Nepal
- c Nepal Netra Jyoti Sangh, Nepal Eye Hospital Complex, PO Box 335, Tripureswor, Kathmandu
- Correspondence to: Professor West
- Accepted 19 January 1999
Abstract
Abstract Objective: To assess the impact on mortality related to pregnancy of supplementing women of reproductive age each week with a recommended dietary allowance of vitamin A, either preformed or as βcarotene.
Design: Double blind, cluster randomised, placebo controlled field trial.
Setting: Rural southeast central plains of Nepal (Sarlahi district).
Subjects: 44646 married women, of whom 20119 became pregnant 22189 times.
Intervention: 270 wards randomised to 3groups of 90each for women to receive weekly a single oral supplement of placebo, vitamin A (7000¼g retinol equivalents) or βcarotene (42mg, or 7000¼g retinol equivalents) for over 31/2 years.
Main outcome measures: All cause mortality in women during pregnancy up to 12weekspost partum (pregnancy related mortality) and mortality during pregnancy to 6weeks postpartum, excluding deaths apparently related to injury (maternal mortality).
Results: Mortality related to pregnancy in the placebo, vitamin A, and βcarotene groups was 704,426,and 361deaths per 100000 pregnancies, yielding relative risks (95% confidence intervals) of 0.60(0.37to 0.97) and 0.51(0.30to 0.86). This represented reductions of 40% (P<0.04)and 49% (P<0.01) among those who received vitamin A and βcarotene. Combined, vitaminA or βcarotene lowered mortality by 44% (0.56(0.37to 0.84), P<0.005) and reduced the maternal mortality ratio from 645to 385deaths per 100000 live births, or by 40% (P<0.02). Differences in cause of death could not be reliably distinguished between supplemented and placebo groups.
Conclusion: Supplementation of women with either vitamin A or βcarotene at recommended dietary amounts during childbearing years can lower mortality related to pregnancy in rural, undernourished populations of south Asia.
Editorial by Olsen
Key messages
Maternal vitamin A deficiency, evident as night blindness or low serum retinol concentration during pregnancy, is widely prevalent in rural south Asia
In Nepal, women of reproductive age who were given 7000¼g retinol equivalents of vitamin A on a weekly basis showed a reduction in mortality related to pregnancy of 40%
Weekly dosing with 42mg βcarotene (also providing 7000¼g retinol equivalents) lowered their mortality by 49%
Preventing maternal vitamin A deficiency in rural South Asia can lower the risk of mortality of women during and after pregnancy
Introduction
Vitamin A deficiency is common among women in developing countries. Mean serum retinol concentrations of about 1.05¼mol/l (300¼g/l) have been reported during pregnancy among diverse groups of south Asian women1–6 in comparison with values of 1.57-1.75 ¼mol/l (450-500¼g/l) in better nourished populations.7
Concern about maternal vitamin A deficiency has focused on its effects on fetal and infant vitamin A status, 1 8–10 health, and survival, 8 11 with little attention being paid to its effects on the health consequences for the woman. An early trial in England reported that maternal vitamin A supplementation in late pregnancy through the first week post partum could reduce the incidence of puerperal sepsis,12 but this lead was ignored. In Nepal maternal night blindness, an indicator of vitamin A deficiency,13 has been associated with increased risks of urinary or reproductive tract infections and diarrhoea or dysentery14 and raised acute phase protein concentrations during infection.15 That vitamin A deficiency could predispose women to increased infectious morbidity and mortality is supported by evidence in children and animals.8 Mechanisms underlying such an effect could include impaired barrier defences of epithelial tissues and compromised innate and acquired immunity. 8 16
We conducted a study in rural Nepal to assess whether routine supplementation of women with normal, dietary amounts of vitamin A or provitamin A βcarotene could favourably affect fetal, infant, or maternal health and survival. In this paper we examine the effects of supplementation on maternal all cause mortality.
Participants and methods
Protocol
The study was a double blind, placebo controlled, cluster randomised trial carried out in Sarlahi district, in the southern plains of Nepal, to assess the effects of continuous, weekly, low dose supplementation of vitamin A or provitamin A βcarotene on mortality related to pregnancy in women of reproductive age. The trial required that the two supplementation groups (vitamin A or βcarotene) enrol a combined total of around 14000 pregnancies (roughly 7000in each group) and the placebo group around 7000 pregnancies, yielding an assignment ratio of 2to 1,to show a<=40% reduction in mortality related to pregnancy with <=80% power (1−β) and 95% confidence (1−α). These assumptions were based on an estimated mortality from pregnancy of >600 deaths per 100000 pregnancies in the study area. Smaller differences (<=20%) in fetal and infant mortality up to 6months of age would be discernible with the same sample size.
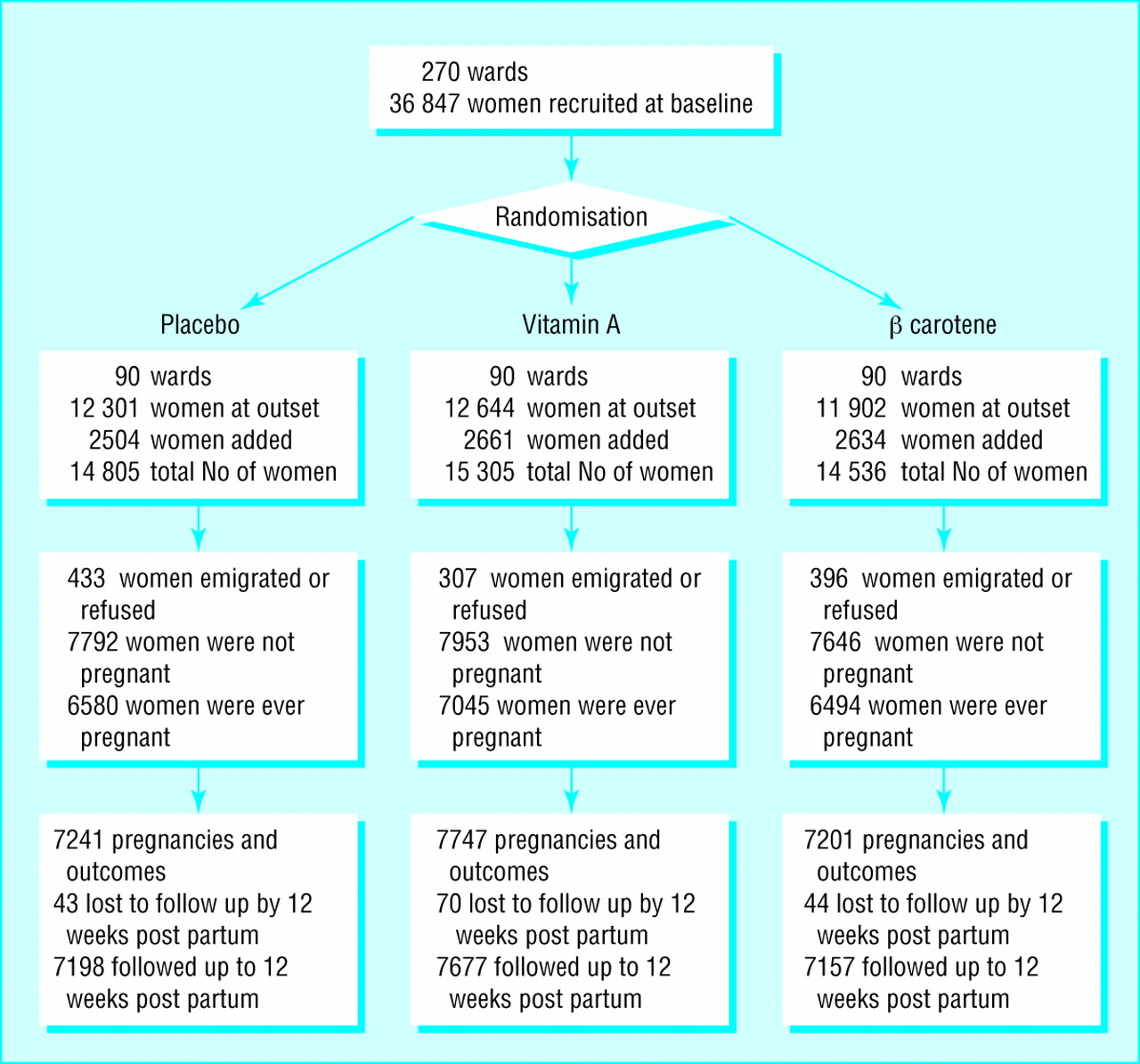
A total of 270wards in 30subdistricts (9wards each) covering an area of around 500sq km with a total population of around 176000 participated in the study. At a local crude birth rate of 41per 1000population per year, we anticipated that recruiting 21000 pregnancies would take around 3years. The purpose of the trial was explained at community meetings, and written consent to participate was obtained from subdistrict leaders during the year before the start of the trial. Women of childbearing age who were married and living with their husbands as of the first week of March 1994were recruited to the trial after giving their verbal consent. Newly married women were recruited throughout the trial. Women who were already married who had moved into study wards were not eligible to participate to minimise crossover. All wards were assigned in Kathmandu by a random draw of numbered chits, blocked on subdistrict, for eligible women to receive one of three identical coded supplements. These were opaque, gelatinous capsules containing peanut oil and 23300 IU of preformed vitamin A (7000g retinol equivalents) as retinyl palmitate, 42mg of all trans βcarotene (7000μg retinol equivalents, assuming a conversion ratio to retinol of 6to 1after uptake17), or no vitamin A or βcarotene (placebo) (fig 1). The dosage was intended to deliver an approximate recommended dietary allowance during pregnancy and lactation17 on a weekly basis. All capsules also contained about 5mg dl-α-tocopherol as an antioxidant.
Field procedures
From April 1994to September 1997a staff of 432local female workers carried out weekly home visits and dosed participating women with their assigned supplement. At least 4days between doses were maintained to avoid any potential risk of toxicity from receiving supplements on two consecutive days. Workers recorded the survival of the women, receipt of capsules, menstrual activity in the previous week, and pregnancy status as reported by women. They revisited the homes of women who were absent until they were able to give them the dose or until the last day of a dosing week. Capsules were not left at homes.
Five months after supplementation and reporting were running smoothly, newly enrolled pregnant women entered into a protocol that included a mid-pregnancy, home based, 7day dietary, morbidity, and activity assessment and measurement of arm circumference by one of a trained team of about 30interviewers. Severely ill women were referred to one of seven local health centres for evaluation. A second visit during the third trimester included socioeconomic evaluation. Seven months after the start of the study newly enrolled pregnant women from a subsample of three contiguous subdistricts (27wards), selected for access, were enrolled for additional measures that required blood collection and measurement of concentrations of retinol and β carotene. A history of events and illnesses preceding death was obtained by interviewing family members of the dead woman (so called verbal autopsy), usually within one month after the death had been reported. These data were reviewed and a “proximate” cause of death assigned by two doctors (SKK and SMD), one of whom was an obstetrician-gynaecologist; both were blind to treatment allocation. Differences in assignment were discussed until the reviewers agreed on a cause of death.
Analysis
Comparability of randomised groups by socioeconomic and dietary characteristics of women during their first enrolled pregnancy was assessed by the χ2 test differences in distributions of serum retinol and βcarotene concentrations were tested by analysis of variance and comparing the two groups with the t test. We checked compliance in each supplement group by examining the percentage of all eligible doses during the trial (or until death) taken by women and the differences in serum retinol and βcarotene concentrations by code among pregnant women in the substudy sample.
Ascertained pregnancies served as the denominator for rate estimation, of which around 91% ended in one or more live births and 6-7% as a declared miscarriage or stillbirth in each group. The remaining 2% of pregnancies had been reported by women at six or more weekly visits but had no reported outcome. We considered these pregnancies to have ended in loss. Pregnancies declared for shorter periods for which no outcome was recorded were considered false positive reports and excluded from the analysis. Eligible pregnancies for this mortality analysis were those ending from mid-July 1994(by which time women had been routinely given supplements for <=5 months) and the end of June 1997,which permitted 12weeks of postpartum dosing and follow up. Mortality was evaluated on an intention to treat basis—that is, by supplement assignment irrespective of compliance. Mortality related to pregnancy and specific causes for each group was calculated from deaths that occurred during pregnancy up to 12weeks post partum and was expressed per 100000 pregnancies. We extended postpartum follow up from 6to 12weeks because maternal mortality related to malnutrition could extend beyond the conventional period of 6weeks. However, we also examined impact on the maternal mortality ratio (for which we excluded deaths due to reported injury and all deaths >6 weeks post partum) in relation to live births. Relative risks with 95% confidence intervals were calculated with the placebo group as the reference.18 Each confidence interval was adjusted to account for the fact that the ward rather than the person was the unit of randomisation. A quasi-likelihood Poisson regression model was used to estimate the degree of overdispersion in the ward specific death rates. 19 20 This overdispersion, due to the design effect, of about 21% of the variance resulted in a 10% inflation in the length of a confidence interval which was applied to the natural logarithm of all estimates of relative risk.
Ethical review
The trial protocol was reviewed and approved by the Nepal Health Research Council in Kathmandu,the Joint Committee on Clinical Investigation at the Johns Hopkins School of Medicine, and the Teratology Society in Bethesda. Two data and safety monitoring committees approved the trial, one in Baltimore and the other in Kathmandu.
Results
A total of 44646 women were recruited, 36847 at the outset and 7799newly married women during the trial (fig 1). In all, 1136(2.5%) women were excluded because they emigrated before becoming pregnant or dying or because they declined to be recruited. Overall, 20119 (45%) women were pregnant 22189 times. Maternal survival was known after all pregnancy outcomes, but 157women were lost to follow up during the postpartum period (their median follow up time post partum was around 2weeks in each group). As the women lost to follow up had completed pregnancies they were included in the denominators for estimating mortality.

At the time of their first study pregnancy, the three groups of women were comparable in age, arm circumference, and weekly dietary intakes. Small differences were evident with respect to cigarette smoking, alcohol consumption, and literacy. A smaller percentage of the placebo group were of low Hindu caste or were not Hindus. Only 3% of pregnancies were delivered at a health post, clinic, or hospital (table 1).
Characteristics of mothers during their first study pregnancy by supplement group. Values are numbers (percentages) unless stated otherwise

{kind=link}
{kind=link}
Women who were pregnant more than once during the trial received a greater percentage of their total eligible supplements than those who were never pregnant (fig 2). For example, half of the women who were ever pregnant and 44% of those who were never pregnant received <=80% of their intended supplements. Over 75% of the pregnant women received at least half of their eligible doses—that is, more than half of a dietary allowance for those receiving vitamin A or βcarotene—compared with around 62% of those who were never pregnant. Compliance was about 3% lower in the βcarotene group in the mid-range of supplement intake.
Among 1446women who had their first pregnancy in the 27substudy wards between September 1994andJuly 1996,1025(71%) were seen at the clinic, of whom 978(95%) were confirmed pregnant by urine test. From these women, serum samples were available for 935(96%) and 916(94%) mid-pregnancy determinations of retinol and βcarotene concentrations, respectively. The mean serum retinol concentration was lowest in the placebo group (1.02μmol/l), highest among vitamin A recipients (1.30μmol/l), and between these two values in the βcarotene group (1.14μmol/l) (table 2). The percentage of women by supplement group with serum retinol concentrations <0.70μmol/l followed the same pattern. The mean βcarotene concentration was significantly higher (0.20μmol/l) and the percentage of women with concentrations <0.09μmol/l lower (26.5%) in the βcarotene than in the vitamin A and placebo groups (around 0.14μmol/l and about 42% in both groups). Thus, compliance with taking supplements seems to have been adequate to change biochemical variables.
Serum retinol and beta carotene concentrations in women during mid-pregnancy
Mortality related to pregnancy up to 12weeks post partum was 704,426,and 361maternal deaths per100000 pregnancies in the placebo, vitamin A, and βcarotene groups, yielding relative risks of 0.60(0.37to 0.97) (P=0.04) and 0.51(0.30to 0.86) (P=0.01) in the vitamin A and βcarotene groups, respectively (table 3). Mortality among women receiving βcarotene was not significantly different from that in the vitamin A group (relative risk 0.85(0.48to 1.49), P=0.57). We therefore combined the effects to obtain a relative risk of 0.56(0.37to 0.84), reflecting a 44% reduction in mortality related to pregnancy associated with vitamin A or βcarotene supplementation (P=0.005). This survival effect was evident after 11/2 years of the trial, reflected by a relative risk of 0.54(0.32to 0.90) (P=0.02), which remained stable during the last part of the trial (relative risk 0.61(0.31 to 1.19), P=0.15, data not shown). The relative risk was protective for both nutritional supplements during pregnancy, from the end of pregnancy to 6weeks post partum, and from 6to 12weeks post partum (table 4).
Impact of supplementation on mortality related to pregnancy up to 12 weeks post partum
Impact of supplementation on mortality in women during and after pregnancy
Analysis of cause specific mortality, based on interviews with relatives, showed protective but non-significant effects of supplementation against risk of death from obstetric causes and infection (table 5). Point estimates of relative risk are stronger for βcarotene than for vitamin A.Supplementation was associated with protection from death attributed to injuries and other miscellaneous causes.
Impact of supplementation on cause related mortality in women during pregnancy up to 12 weeks post partum. Values are numbers of women unless stated otherwise
The maternal mortality ratio was 645(42deaths/6670 live births), 407(29/7074), and 361(23/6643) per 100000 live births in the placebo, vitamin A, and βcarotene groups, respectively (P=0.08 for vitamin A and 0.04for βcarotene vplacebo). The ratio for women receiving either vitamin A or βcarotene was 385, yielding a relative risk of 0.60(0.39to 0.93), representing a 40% reduction in mortality by this measure (P=0.02).
Discussion
In this poor, rural Asian setting the risk of death related to pregnancy was lowered, by about 40%, among women who were routinely given dietary supplements of vitamin A or βcarotene rather than placebo. Effect estimates were similar during pregnancy and post partum. The protective impact was established after 11/2 years of supplementation, reflecting consistency of the effect over time and a potential duration of dosing a population by which a clear mortality reduction could be expected. The impact on mortality was similar when expressed as a maternal mortality ratio that excluded deaths related to injury and those occurring more than 6weeks post partum. The comparability of groups of pregnant women with respect to compliance and demographic, socioeconomic, dietary, and obstetric variables shows that the observed survival effect was unlikely to have resulted from imbalances in other factors that could have influenced maternal mortality.
We intended the weekly dosage of vitamin A or βcarotene to deliver the equivalent of a liberal dietary allowance of vitamin A for pregnant or lactating women. 17 21 Although more than three quarters of all women who became pregnant during the trial received at least half of their recommended allowance of vitamin A through supplements, only half took 80% or more of their eligible supplements. This suggests that the risk of maternal death in populations who are deficient in vitamin A could be substantially lowered with modest increases in vitamin A or βcarotene intake, as has been shown in children.22
The interview with relatives was a feasible and insightful way to investigate causes of death in a population where medical diagnoses were unobtainable; however, this method may be subject to considerable imprecision and misclassification, 23 24 particularly given the complex nature of deaths related to pregnancy and the common lack of pathognomonic signs or symptoms that would be evident to lay relatives. Our interviews with relatives suggested there was a 22% reduction in infectious causes of death ((1−0.78)μ100), but the finding was inconclusive. Some deaths due to infection may have been misclassified as uncertain. Eight of the 12deaths with completed interviews (five women had been in the placebo group and three in the vitamin A and βcarotene group) had reported symptoms that were consistent with infectious disease before death.
A 27% decrease in maternal mortality was attributed to obstetric causes in women receiving supplements. The effect seemed to be more strongly associated with βcarotene (relative risk 0.56,P=0.18) than vitamin A (relative risk 0.88,P=0.73). Although the putative role of antioxidant defences in preventing disease25 and an in vivo antioxidant role for βcarotene26 remain controversial, βcarotene, acting as an antioxidant, 27 28 could have reduced some forms of obstetric risk in this malnourished population. Low serum βcarotene concentrations have been observed in pregnant Asian2 and African29 women with pre-eclampsia and eclampsia, whose pathogenesis entails vascular endothelial injury that may be associated with oxidative stress. 30 31 Placental abruption has also been associated with depressed serum antioxidant concentrations, including βcarotene.32
Currently, supplementation programmes of weekly low doses of vitamin A or βcarotene do not exist for women of reproductive age, although this approach may be a cost effective way of preventing iron deficiency anaemia in the developing world.33 Our findings suggest that raising the intake of preformed vitamin A or provitamin A carotenoids towards the values recommended for pregnancy or lactation, presumably by supplementation or by dietary means, can complement antenatal and essential obstetric services in lowering maternal mortality in rural south Asia.
Acknowledgments
The NNIPS-2 (Nepal Nutrition Intervention Project-Sarlahi) Study Group includes (in addition to the authors) Drs Ramesh Adhikari, Bhakta Raj Dahal, Michele Dreyfuss, Rebecca Stoltzfus, James Tielsch, and Sedigheh Yamini-Roodsari; Noor Nath Acharya, Dev N Mandal, Kerry Schulze, Tirtha R Shakya, Lee Shu-Fune Wu, Andre Hackman, and Gwendolyn Clemens.
We thank Drs Frances Davidson, Victor Barbiero, Tim Quick, Martin Frigg, James Tonascia, Frederick Trowbridge, Calvin Willhite, and David Calder; Molly Gingerich, Charles Llewellyn, David Peat, Lisa Gautschi, Ravi Ram, and more than 550staff of the NNIPS-2 study for their help.
Contributors: KPW was the principal investigator, formulated the major hypotheses, directed the study and analysis, wrote the paper, and is guarantor for the study. JK helped in study design, developed the data management and quality control systems, analysed the data, and contributed to writing the paper. SKK helped design forms and develop procedures and assigned causes of maternal death based on review and interpretation of verbal autopsies. SLC developed field procedures, helped in designing forms, supervised field supplementation and data collection, and helped to edit the paper. EKP helped design and pretest forms, managed data editing and entry and quality control systems and participated in data analysis and interpretation of findings. SRS supervised field data collection and supplementation and helped prepare manuals of field operations. PBC designed the data management and quality control systems. SMD helped develop protocols for assessing maternal morbidity and for verbal autopsies. PC helped in implementing the field study and contributed to the data analysis, interpretation of findings, and preparation of the manuscript. RPK oversaw the implementation and integration of the trial in the community. AS had the original idea of a maternal supplementation trial, helped in its conceptualisation, reviewed its design and procedures, and contributed to writing the paper.
Members of the study group are given at the end of the article
Funding: The NNIPS-2 trial was a collaboration (cooperative agreement No HRN-A-00-97-00015-00) between the Center for Human Nutrition and the Sight and Life Institute in the Department of International Health at the Johns Hopkins School of Public Health and the National Society for Comprehensive Eye Care (Nepal Netra Jyoti Sangh), Kathmandu, Nepal. It was supported by the Office of Health and Nutrition, US Agency for International Development (USAID), Washington, DC, and assisted bythe Sushil Kedia Foundation, Sarlahi, Nepal. The capsules were provided by Roche, Basle, as part of its Task Force Sight and Life project.
Conflict of interest: KPW and AS have received funds to support vitamin A research in the developing world from Task Force Sight and Life, Roche, Basle. The Center for Human Nutrition has received an endowment from Roche to establish a Sight and Life Institute for conducting micronutrient research related to child and maternal health and survival.