Article Text

Abstract
Objective: To estimate the incremental cost-effectiveness of the first-line pharmacotherapies (nicotine gum, patch, spray, inhaler, and bupropion) for smoking cessation across six Western countries—Canada, France, Spain, Switzerland, the United States, and the United Kingdom.
Design and study population: A Markov-chain cohort model to simulate two cohorts of smokers: (1) a reference cohort given brief cessation counselling by a general practitioner (GP); (2) a treatment cohort given counselling plus pharmacotherapy. Effectiveness expressed as odds ratios for quitting associated with pharmacotherapies. Costs based on the additional physician time required and retail prices of the medications.
Interventions: Addition of each first-line pharmacotherapy to GP cessation counselling.
Main outcome measures: Cost per life-year saved associated with pharmacotherapies.
Results: The cost per life-year saved for counselling only ranged from US$190 in Spain to $773 in the UK for men, and from $288 in Spain to $1168 in the UK for women. The incremental cost per life-year saved for gum ranged from $2230 for men in Spain to $7643 for women in the US; for patch from $1758 for men in Spain to $5131 for women in the UK; for spray from $1935 for men in Spain to $7969 for women in the US; for inhaler from $3480 for men in Switzerland to $8700 for women in France; and for bupropion from $792 for men in Canada to $2922 for women in the US. In sensitivity analysis, changes in discount rate, treatment effectiveness, and natural quit rate had the strongest influences on cost-effectiveness.
Conclusions: The cost-effectiveness of the pharmacotherapies varied significantly across the six study countries, however, in each case, the results would be considered favourable as compared to other common preventive pharmacotherapies.
- smoking cessation
- nicotine replacement therapy
- cost-effectiveness analysis
- Markov model
- countries
Statistics from Altmetric.com
Tobacco kills four million people worldwide each year and is presently one of the leading causes of avoidable premature death in the developed world.1 The main principle approaches to slowing the epidemic are prevention of initiation among young people and cessation among current tobacco users. Prevention is essential for achieving medium- and long-term reductions in tobacco-caused morbidity and mortality, while cessation will be the key to averting millions of deaths among current smokers that are forecasted for the next 50 years.1,2 Smokers who quit before the onset of illness will avoid most of the added mortality risk from smoking, which begins falling within a few years of cessation.3,4
Pharmacologic smoking cessation therapies—nicotine delivery through gum, patch, spray, or inhaler, and bupropion, an antidepressant that reduces symptoms of withdrawal and depression associated with quitting—have been shown to approximately double a smoker’s odds of quitting successfully when used in adjunction to brief physician counselling.5–7 It has been emphasised that studying the extent to which various tobacco dependence drug therapies are cost-effective requires additional research.7 Previous cost-effectiveness studies have been conducted for single countries only, limiting the possibility to generalise their results to other settings where the cost of physicians’ time and/or the pharmacotherapies may differ. Furthermore, previous economic studies of smoking cessation have used different methods and assumptions for estimating costs and effectiveness, making comparison between studies difficult.
To our knowledge, no study has compared cost-effectiveness of the five first-line pharmacotherapies across several different countries. In this analysis, we estimated the cost-effectiveness of the first-line pharmacotherapies for six Western industrialised countries.
METHODS
We calculated the cost per life-year saved of general practitioners (GPs) providing their patients each of the five first-line pharmacotherapies as an adjunct to cessation counselling for Canada, France, Spain, Switzerland, the United Kingdom (UK), and the United States (US). We selected these countries because they provided a broad perspective that represented Anglo-Saxon, Latin, and Germanic populations. Table 1 provides a summary of the most common, relevant characteristics of the health care system for each study country.8,9,10,11,12,13,14,15,16,17,18,19 Based on available evidence, we assumed that the effectiveness of treatment (that is, counselling and adjuvant pharmacotherapy) and the associated effects on mortality were the same across all countries.5 We calculated the costs of the pharmacotherapies separately for each country based on country-specific data. To shorten the length of this report, we presented here results for a 45-year-old man or woman and for the entire cohort divided into three age categories.
Summary characteristics of health care systems for each country
Calculation of effectiveness
We supposed that GPs provided their smoking patients opportunistic cessation counselling during routine office visits and offered pharmacotherapy to those for whom it was indicated. Clinical guidelines indicate pharmacologic cessation therapy only for smokers who consume at least 10–15 cigarettes per day.7 A large majority of daily smokers visiting a GP smoke on average a pack a day.20–22 Therefore, we included in our simulated cohorts only patients who smoked, on average, 20 cigarettes per day.
We used a validated computer-simulated Markov model to generate two cohorts of identical smokers.23,24 Details can be found in the appendix entitled Markovmodel.pdf on the Tobacco Control website— http://www.tobaccocontrol.com. We characterised the two cohorts according to a set of base-case assumptions (table 2). The reference cohort received only cessation counselling from a GP. The second cohort received the same counselling plus each of the five pharmacotherapies. We expressed the effectiveness of adjuvant pharmacotherapy as the additional number of life-years saved attributable to the offer, use, and follow-up of each of the five pharmacotherapies. We derived the effectiveness of counselling and nicotine replacement therapy (NRT) from two published meta-analyses.5,6 We based the effectiveness of bupropion on a meta-analysis performed by the US Department of Health and Human Services.7 Each of these reference studies based its measurement of cessation status on the point prevalence at one year of abstinence. We used the reported odds ratios for efficacy from these studies as our measure of effectiveness for each form of treatment. We assumed that quit odds ratios were the same for men and women, the rationale for which has been presented elsewhere.6 Nicotine spray and nicotine inhaler were not approved for use in Canada and France, and Canada and Spain, respectively, so estimates in these cases could not be included in the analysis.
Variables used in the analysis
Cessation rates and risk of relapse
We assumed a natural quit rate (that is, cessation without intervention) of 2.5%. This rate reflects the estimated probability of quitting smoking over the course of one year in Switzerland as well as in other Western countries.20,25 Studies have shown that 50–70% of smokers would like to quit smoking.21,26 Yet, according to the Stages-of-Change model, a much smaller proportion of these smokers is in the preparation stage—truly ready to make a serious quit attempt—and therefore appropriate candidates for pharmacotherapy.27 We assumed that 25% of current smokers were in the preparation stage for quitting.28 The long-term risk of relapse for former smokers is not well documented. Existing long-term follow-up data suggest that approximately 30% of subjects who have been abstinent for one year will relapse sometime during the following five years.29,30 Relapse after five years does occur, but the rate is insignificantly low.29,30 From previous studies, we adopted the conservative assumption of a 35% lifetime probability of relapse after one year of validated abstinence.31,32
Mortality effects of smoking cessation
We based the mortality effects of smoking cessation for smokers of the six countries on the same data—that is, the results of the American Cancer Society Prevention Study II (CPSII)—which compared mortality rates for smokers and non-smokers up to age 75.29 According to this and other studies, the excess mortality risk declines significantly after cessation, and we assume that the mortality rate of former smokers rejoins that of never smokers approximately 20 years after quitting.3,4,29,33 Based on the findings of CPSII, we extrapolated the mortality curves to age 90 and supposed a phase-in period of 25 years for former smokers’ mortality risk to return to that of non-smokers.29
Cost of smoking cessation therapies
We assumed a third-party-payer perspective in calculating medical and non-medical costs of smoking cessation therapies, an approach used in previous cost-effectiveness analyses of NRT.34 This approach helps facilitate a comparison of our results with those of existing studies. We based the dosage and duration of pharmacotherapy on current clinical guidelines, which recommend that pharmacologic treatment last up to three months.7 Physicians commonly recommend that patients use pharmacotherapy for a minimum of one month, so we assumed that all smokers in the treatment cohort incur the costs of at least one month of NRT and bupropion, respectively. Previous studies suggest that 50% of smokers who initiate treatment continue for a second month, and only 30% of those who start continue for a third month.26,35 We estimated pharmacotherapy prices in the study countries based on pharmacy prices or published price data (view the appendix on the Tobacco Control website— http://www.tobaccocontrol.com). For Canada, we conducted an original survey of 50 randomly selected retail pharmacies across the country, weighted by province. For the US, we estimated average pharmacotherapy prices in January 2003 from two nationwide pharmacy chains (CVS, Chapel Hill, North Carolina; RiteAid, Los Angeles, California). Prices for France, Spain, Switzerland, and the UK were based on publicly or privately published price data.36–40 We compared these price data with those from other sources to verify reliability (for France, Vidal online 2003: www.vidal.fr; for Spain, Catalogo de Especialidades Farmaeutica 2002; for Switzerland, Pharmacia AG Suisse and Galexis 2003 Files; for UK, MIMS march 2003 par e-mediat AG). We based the costs associated with physicians’ time on the cost to a third-party-payer of a general consultation by a GP that does not include any technical procedures. We collected these data from the Ontario Medical Association (Ted Broadway, personal communication, December 2002) for Canada, estimates from the existing literature for France,41 official government data for Spain, the UK, and the US,42–44 and a private medical data consulting service for Switzerland.45
Sensitivity analysis
We conducted sensitivity analysis for several of the input variables (see table 2 for ranges used), which provides an important illustration of the degree to which cost-effectiveness changes in response to variations in input values. We based the sensitivity analysis for treatment efficacy on the 95% confidence interval. The parameters that change by country were price of inputs to smoking cessation therapy and physicians fees.
Discounting and currency conversion
To account for the time gap between the costs of the intervention and the benefits in life-years saved, it is common practice to calculate the present discounted value of the earlier-incurred costs and the later-realised benefits, thereby measuring their value on the same relative scale.23,46 We used a 3% discount rate in our base case analysis, which adheres to current guidelines for cost-effectiveness analysis.47 However, to present the results in their “raw” form and to acknowledge other discounting rationales, we included rates of 0% and 5% in the sensitivity analysis. To enable cross-country comparisons, we conducted the analysis using US dollars. We converted monetary data for each country according to the following 2002/2003 market rates of exchange for one US dollar: 1.42 Swiss francs, 0.64 British pounds, 1.01 Euros, and 1.54 Canadian dollars.
RESULTS
The cost per life-year saved for a 45-year-old for counselling was in ascending order $190 and $288 for men and women in Spain, $375 and $567 in Switzerland, $389 and $588 in Canada, $479 and $724 in France, $623 and $941 in the US, and $773 and $1168 in the UK. This high variation in the cost-effectiveness of counselling across the six study countries—the ratios for the UK are four times higher than for Spain—was due to substantial differences in GPs’ fees. For example, the hourly rate for a consultation with a GP in Spain was $33, while in France the rate was 2.5 times higher at $83 per hour, and in the UK it was four times higher at $134 per hour.
All cost-effectiveness ratios for pharmacotherapies must be interpreted in incremental terms, as they reflect the additional costs and benefits associated with adding pharmacotherapy to a base of physician counselling. The incremental cost per life-year saved varied across countries and pharmacotherapies, but in each case, pharmacotherapy as an adjunct to counselling yielded a greater number of life-years saved as compared to average gains from counselling only. Among the six countries, the incremental cost per life-year saved for a 45-year-old smoker (tables 3 and 4) ranged from $2230 for men in Spain to $7643 for women in the US for gum; $1758 for men in Spain to $5131 for women in the UK for patch; $1935 for men in Spain to $7969 for women in the US for spray; $3480 for men in Switzerland to $8700 for women in France for inhaler; and $792 for men in Canada to $2922 for women in the US for bupropion. Within pharmacotherapies, the highest cost-effectiveness ratio ranged from approximately 1.6 higher (inhaler) to almost three times higher (spray) than the lowest ratio. The most cost-effective pharmacotherapy for each country was bupropion, followed by the patch. The ranking of gum, spray, and inhaler varied across countries, though in many cases, the spray and inhaler outperformed the gum.
Incremental cost per life-year saved for a 45-year-old smoker: gum, patch, spray
Incremental cost per life-year saved for a 45-year-old smoker: inhaler, bupropion
There was a consistent difference, across all countries and pharmacotherapies, in cost-effectiveness between men and women, which proceeds directly from their respective smoking-caused mortality risk. The mortality curve related to smoking is steeper for men due to a greater burden of smoking-caused death and disease, and their burden is greater than women’s due to greater consumption (that is, more cigarettes smoked on average) than women.48 Men, therefore, stand to gain more units of benefit—life-years saved—from cessation than women, which results in the intervention being more cost-effective (lower cost-effectiveness ratios) for men than for women.
Cost-effectiveness ratios differ across all pharmacotherapies and countries according to age of patients at the time of the intervention (tables 5–10). The cost-effectiveness ratio was lowest among 35–49-year-olds for both sexes. However, the age class with the highest ratio was the class 20–34 for the women and the class 50–64 for the men. For example, among Canadian men, the cost-effectiveness ratio for gum was $3330 for 20–34-year-olds, $2791 for 35–49-year-olds, and $3699 for 50–64-year-olds. Among French women, the cost-effectiveness ratio for the inhaler was $12246 for 20–34-year-olds, $8924 for 35–49-year-olds, and $9458 for 50–64-year-olds. For Spanish men, the cost-effectiveness ratio for the spray was $2285 for 20–34-year-olds, $2208 for 35–49-year-olds, and $2926 for 50–64-year-olds. Among Swiss men, the cost-effectiveness ratio for the patch was $3430 for 20–34-year-olds, $2875 for 35–49-year-olds, and $3810 for 50–64-year-olds. For men in the UK, the cost-effectiveness ratio for bupropion was $1762 for 20–34-year-olds, $1477 for 35–49-year-olds, and $1957 for 50–64-year-olds. And among US women, the cost-effectiveness ratio for bupropion was $4112 for 20–34-year-olds, $2997 for 35–49-year-olds, and $3176 for 50–64-year-olds. Two dynamics account for this effect of all pharmacotherapies becoming progressively less cost-effective as patient age both increased and decreased from the middle-aged group: for the youngest smokers, discounting diminishes the value of the benefits and therefore the cost-effectiveness of pharmacotherapy; for the older smokers, the greater probability that they will die before realising all the benefits of quitting likewise diminishes the cost-effectiveness.
Incremental cost per life-year saved by age categories: Canada
Incremental cost per life-year saved by age categories: France
Incremental cost per life-year saved by age categories: Spain
Incremental cost per life-year saved by age categories: Switzerland
Incremental cost per life-year saved by age categories: United Kingdom
Incremental cost per life-year saved by age categories: United States
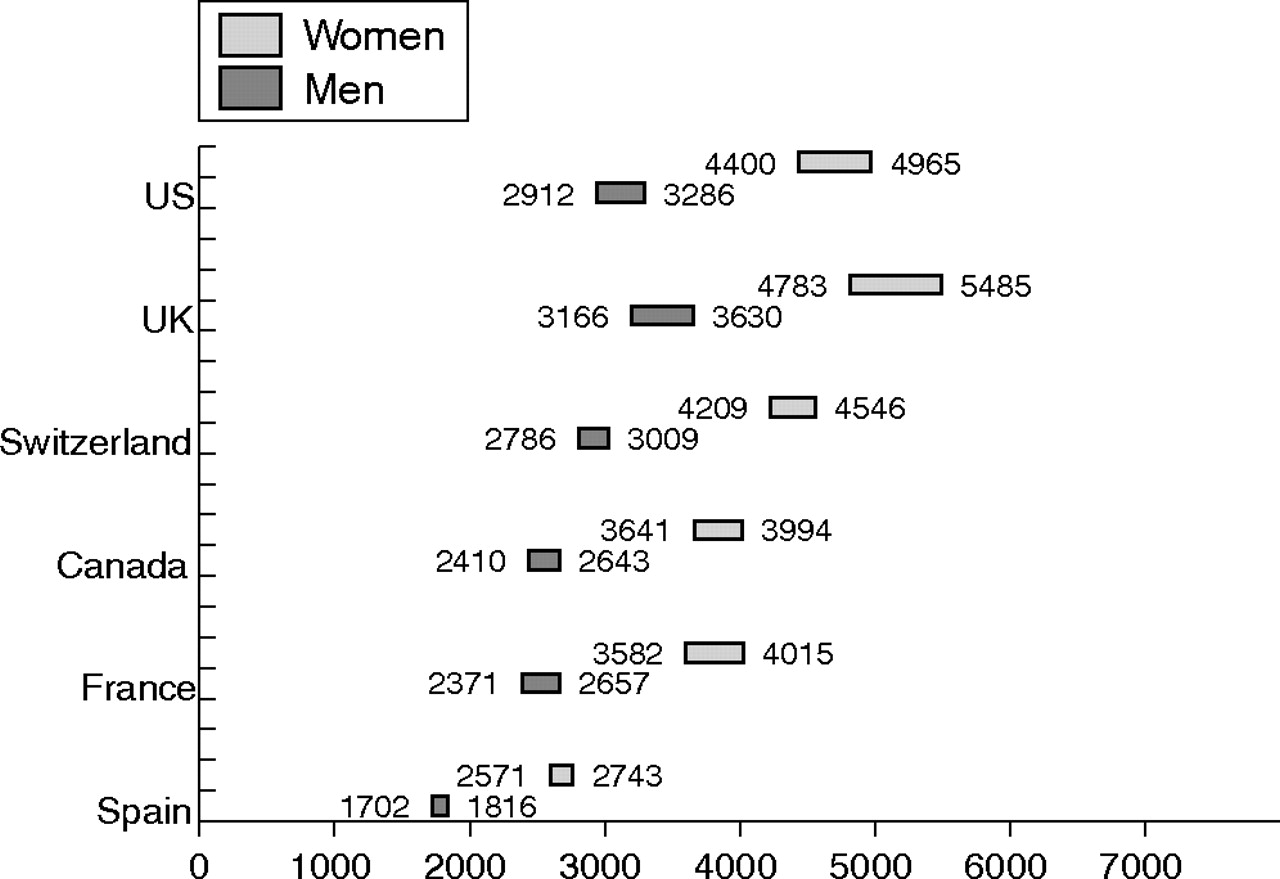
Sensitivity analysis had a significant effect on the cost-effectiveness of the pharmacotherapies, particularly when applied to the discount rate, treatment efficacy, and the natural quit rate. Regarding discount rate, applying a rate of 0% resulted in approximately 45% and 30% lower cost-effectiveness ratios for men and women, respectively, than the base case assumption of 3% discount rate. At a discount rate of 10%, the cost-effectiveness ratios were approximately 66% and 77% higher than at a rate of 3%. This effect was consistent across all countries and pharmacotherapies. For treatment efficacy, the effect of sensitivity analysis, based on the upper and lower bounds of the 95% confidence interval (CI) for the efficacy odds ratio, was significant across all countries and pharmacotherapies, as demonstrated for the patch (fig 1), which showed that the ratios have large ranges—for example, from 4967 to 5661 for women in Canada. The effect was particularly pronounced for the spray, inhaler, and bupropion, raising the cost-effectiveness ratio by 2–3 times at the lower bound for treatment efficacy. This effect was relatively large because the 95% CIs for these pharmacotherapies are wide, and the CIs are wide because there are at present relatively few efficacy studies to include in meta-analysis for these three pharmacotherapies. Cost-effectiveness ratios changed between 11–18% when pharmacotherapy cost was raised and lowered by 20%, as showed in the case of patch in fig 2. Cost-effectiveness was also very sensitive to variations in the natural quit rate. In each case and across all pharmacotherapies, the cost-effectiveness ratio was approximately twice as high as the base case at a rate of 1% and was approximately one quarter lower at a rate of 4%. For example, among women in Spain, the cost-effectiveness ratio for nicotine gum, which was $3370 according to the base case assumptions, varied from $7007 to $2512 at natural quit rates of 1% and 4%, respectively. And for men in Canada, the cost-effectiveness ratio for bupropion was $792 according to base case assumptions, and $1661 and $585 at natural quit rates of 1% and 4%, respectively. Varying the lifetime relapse rate to 10% and 50% lowered and raised, respectively, cost-effectiveness by approximately 25%. Cost-effectiveness ratios were relatively insensitive to changes in GPs’ fees, changing by approximately 3–6% when GPs’ fees were raised and lowered by 15%, as showed for the patch in fig 3. Variations in the relapse rates during the first and second months of treatment had only minor effects.
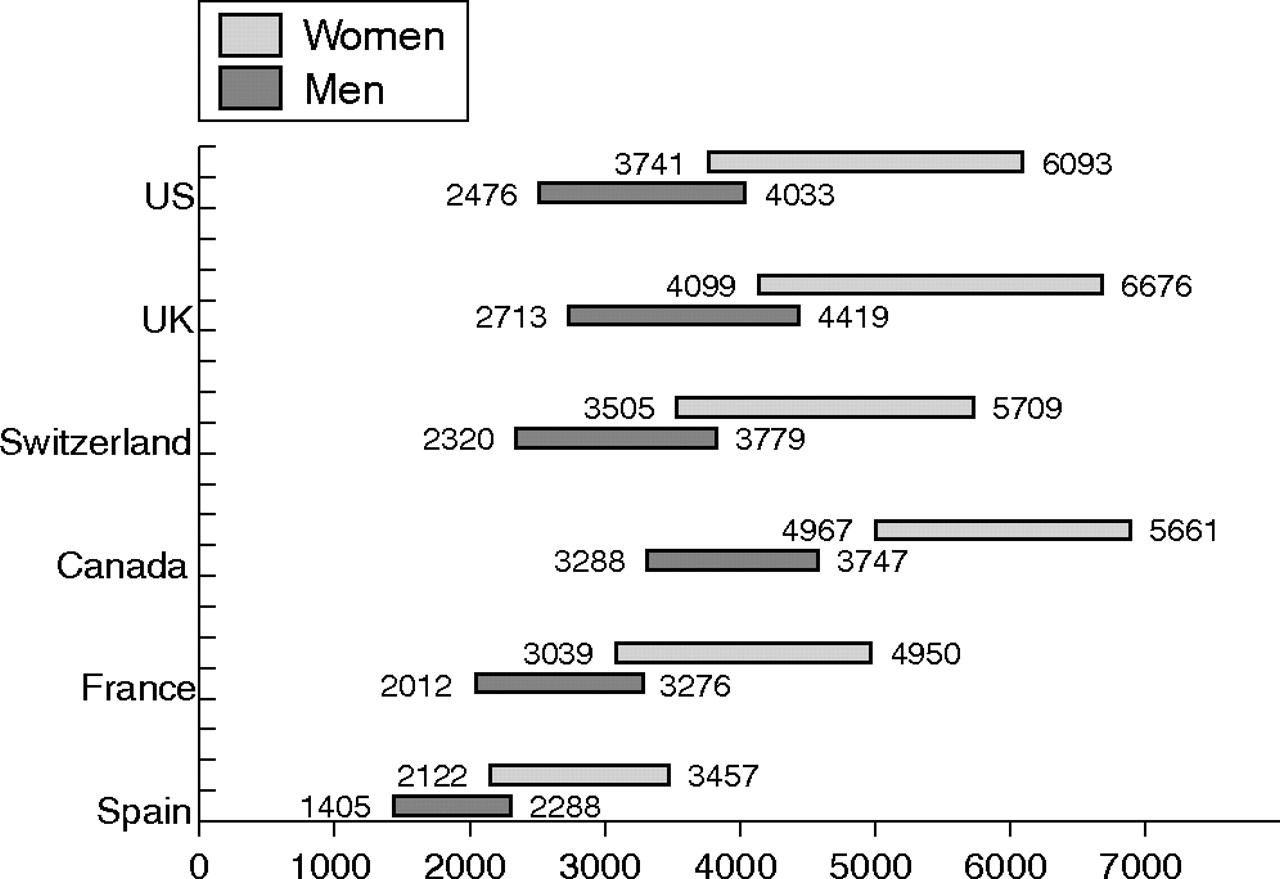
Sensitivity of cost-effectiveness of nicotine patch to 95% confidence intervals for pharmacotherapy efficacy odds ratios (US$).

Sensitivity of cost-effectiveness of nicotine patch to 20% change in pharmacotherapy cost (US$).
{kind=link}
{kind=link}
{kind=link}
Sensitivity of cost-effectiveness of nicotine patch to 15% change in general practitioners’ fees (US$).
DISCUSSION
The key features of our study are the following: (1) the cost-effectiveness of counselling highly varied across the six countries due to substantial differences in GPs’ fees; (2) pharmacotherapy as an adjunct to counselling yielded a greater number of life-years saved as compared to average gains from counselling only; (3) the most cost-effective pharmacotherapies for each country and both sexes were bupropion, followed by the patch; (4) the greater burden of smoking-caused death and disease among men translated into more unit life-years saved from cessation than women, which resulted in the intervention being more cost-effective for men; (5) the cost-effectiveness ratio was highest among 20–34-year-olds and lowest among 35–49-year-olds due to the mortality curve related to smoking; (6) the sensitivity analysis highlighted a significant effect of discount rate, treatment efficacy, and natural quit rate on the cost-effectiveness ratio.
One of the primary advantages of this multi-country analysis is its broad perspective, providing current estimates of cost-effectiveness of pharmacotherapies across several countries, which is useful in assessing generalisability to other settings. The variation in cost-effectiveness across the selected countries is significant, with the difference in some cases approaching a factor of three—for example, $1935 per life-year saved for the spray in Spain versus $5275 in the US. However, when viewed in a broader context, namely in comparison to other preventive medicine interventions, the cost-effectiveness ratios for these pharmacotherapies would be considered favourable for each study country. For example, a 1998 Canadian study found the cost-effectiveness of lovastatin for the primary prevention of cardiovascular disease to range from CAD$11 040 to CAD$52 463 (US$8212 to $39 020 in 2002 US$).49 A 1995 Canadian study found the cost per life-year saved for hypercholesterolaemia drug therapies to range from CAD$17 231 to CAD$155 891 (US$18 293 to $199 892 in 2002 US$),50 and a 2000 US study found the cost per quality-adjusted life-year saved to range from $54 000 to $1 400 000 ($56 415 to $438 780 in 2002 US$).51 Furthermore, hypertension and hypercholesterolaemia drug therapies (and their costs) continue throughout the remainder of the patient’s life, while smoking cessation treatment (and its costs) lasts only a few months. This reflects a substantial difference in total lifetime expenditures per patient between the two types of interventions. Furthermore, the cost-effectiveness of these pharmacotherapies is likely to improve as generic versions—usually significantly lower in cost than name brand versions—become more widely available.
A second important value of this multi-country analysis is that it reveals the specific effects of health care costs on cost-effectiveness in six unique settings. Both physicians’ fees and pharmacotherapy prices vary significantly across the selected countries, by as much as factors of 4.5 and 3.4, respectively. Overall, pharmacotherapy price has a stronger influence on the cost-effectiveness ratio than physicians’ time since it comprises a larger proportion of the total cost of the intervention. For example, in the case of Spain, the total cost of GPs’ time for the intervention is $55, while the total cost of pharmacotherapy ranges from $214 to $432. Even in the case of the UK, which has the highest GPs’ fees of the six countries, the total cost of the physician’s time for a three-month course was estimated to be $223, while pharmacotherapy costs range from $253 to $649. In an effort to maximise the cost-effectiveness of this intervention, it may be useful for policymakers in countries where the proportion of physicians’ cost is relatively high—for example, the UK and the US—to consider training lower-cost health care professionals to oversee treatment.
The sensitivity analysis stresses the role of assessing not only the usual variables in such analysis (that is, discount rate and treatment efficacy), but also baseline or natural probability of having the clinical outcome (that is, quitting rate in our case), since the cost-effectiveness ratio of pharmacotherapies increases by a factor of three when natural quit rate goes from 4% to 1%.
Presently, the time spent by physicians counselling patients to quit smoking, prescribing, and following up pharmacotherapy is reimbursed by public or private insurance in each country as time spent in patient consultation (table 1). In each case, however, there is evidence that 50% or more of GPs do not recommend quitting and pharmacotherapy to their patients for whom it is indicated. On the contrary, the cost of the pharmacotherapies is in most common circumstances not reimbursable and is therefore paid out-of-pocket by the patient in each of the six countries. The keys to increasing the use and coverage of pharmacotherapies will be twofold: encouraging GPs to systematically recommend quitting and using pharmacotherapies to the smoking patients, and making pharmacotherapy as accessible as possible to appropriate smokers.
It is also useful to compare our results with existing cost-effectiveness analyses of NRT, bearing in mind that methodological differences play a significant role in the variation across results. One US study found the incremental cost per life-year saved associated with nicotine gum to range from $4167 to $9473 ($6840 to $15 549 in 2002 US$).34 Two other US studies found the incremental cost per life-year saved associated with the nicotine patch to be $1796 to $4391 ($2013 to $4922 in 2002 US$) and $4390 to $10 943 ($5034 to $12 547 in 2002 US$), respectively.31,32 Both these studies of the patch assumed a treatment course of two months (versus three months in our study), which alone itself would lower cost-effectiveness ratios by one-third as compared to ours. A 2002 UK study estimated that the incremental cost per life-year saved for NRT was £2399 ($3598 in 2002 US$) and for bupropion was £1969 ($2953 in 2002 US$).52 Another 2002 UK study calculated the incremental cost per life-year saved associated with bupropion to be between US$920 to US$2150.53
Our study has some limitations. First, due to a lack of available evidence, we were unable to account for variations in treatment effectiveness across individuals or countries. Some potential influences could be age, cigarette consumption, socioeconomic status, and race, or social value given to cessation as related possibly to a country’s tobacco control policies, such as level of cigarette tax or restrictions on advertising and smoking in public places. Second, we used life-years saved as the measure of benefit and not disability-adjusted life years (DALYs), which also account for time spent living with tobacco-caused disease. Applying DALYs is likely to improve cost-effectiveness of pharmacotherapies. We opted instead to take the more conservative approach because there exists some debate regarding the derivation of the measure, in particular the disagreements among researchers with either the assumptions behind DALYs or the methods of calculation.54,55 Third, instead of using exchange rates to convert national currencies to US dollars, we might have used purchasing power parity, a parameter also appropriate for international comparison. However, using one current device, such as US dollars, to enable cross country comparisons let us put our results in an important perspective—that is, the comparison with cost-effectiveness ratios of other medical and preventive interventions, as mentioned above. Furthermore, our option ensures international Tobacco Control readers are able to compare data for their own country to other data they may know in other health care fields from the medical literature. Overall the data would have been on the same magnitude, albeit the differences between countries would have been a little bit smaller. Finally, a single, standardised data source for all study countries was not available, so there was some variability in the level or method by which data were collected (for example, pharmacy survey versus government data versus private consulting service data for treatment prices). We did, however, compare pharmacotherapy price data to those collected by another, independent source and confirmed that they were acceptably similar.
What this paper adds
Pharmacologic smoking cessation therapies have been shown to be cost-effective only in single settings.
Our Markov-chain cohort model simulating two cohorts of smokers shows that the incremental cost-effectiveness of the first-line pharmacotherapies (nicotine gum, patch, spray, inhaler, and bupropion) varied significantly across Canada, France, Spain, Switzerland, the United States, and the United Kingdom, with the difference in some cases approaching a factor of three. However, in each case, the results would be considered favourable as compared to other common preventive pharmacotherapies. Sensitivity analysis shows that changes in discount rate, treatment effectiveness, and natural quit rate have the strongest influences on cost-effectiveness.
Conclusion
The cost-effectiveness of the first line pharmacotherapies for smoking cessation varied significantly across Canada, France, Spain, Switzerland, the United Kingdom, and the United States. In each case, bupropion and secondly the patch were the most cost-effective treatments. In each country, pharmacotherapies for smoking cessation would be considered favourable in terms of cost-effectiveness as compared to several other common preventive drug treatments.
Acknowledgments
The authors thank Milca Gikic, Martin Jarvis, Jean-Marc Leder, Anne Stoebner-Delbarre, Bertrand Dautzenberg, Simon Galton, and Ruth Loewen for their help getting data.
REFERENCES
Supplementary materials
Footnotes
-
Competing interest: none to declare