Article Text

Abstract
AIM To assess the effect of nasal continuous positive airways pressure (CPAP) on the dimensions of the laryngeal opening.
METHODS Nine preterm infants who had previously received ventilatory support for respiratory distress syndrome (RDS) were studied. All were receiving nasal CPAP. The laryngeal opening was visualised using a fibre optic video camera system. The ratio of width to length of the opening was measured on and off CPAP.
RESULTS In eight of the infants the width: length ratio increased on CPAP; mean change for group +24.4% (95% CI +11.9 to +37.9).
CONCLUSIONS Nasal CPAP seems to dilate the larynx. This may explain the selective beneficial effects of CPAP on mixed and obstructive apnoea.
- nasal continuous positive airway pressure
- apnoea of prematurity
- laryngoscopy
- vocal cords
Statistics from Altmetric.com
The use of continuous positive airway pressure (CPAP) for the treatment of apnoea of prematurity was first described in 1975.1 Since then studies have shown that CPAP roughly halves the incidence of apnoeic episodes.2 Several mechanisms have been suggested to explain this effect. CPAP may stabilise the chest wall during breathing which could eliminate the suppressant effect of the intercostal–phrenic inhibitory reflex, stimulated by chest wall distortion in preterm infants.3An alternative explanation is that the improvement in oxygenation which often accompanies the use of CPAP is responsible.4 Other studies have suggested that stimulation of the Hering Breuer inflation reflex may be responsible.5 It is now well established that the apnoea of prematurity can be divided into three types—namely central, obstructive, and mixed.6 7 Miller and colleagues8 showed that CPAP was highly effective as a treatment for mixed and obstructive apnoea, but that it did not reduce the incidence of central apnoea. This raised the possibility that airway closure may be the primary event in mixed apnoea, acting via the intercostal–phrenic inhibitory reflex so that CPAP prevents airway closure rather than by directly affecting central respiratory drive.
The two most probable sites for upper airway obstruction are in the pharynx and at the level of the larynx. The pharynx is composed entirely of soft tissues and kept patent during inspiration by the opposing actions of the genioglossal and geniohyoid muscles.9 Any reduction in the tone of these muscles will tend to lead to obstruction. This has been well documented as the cause and site of obstruction in children and adults presenting with obstructive sleep apnoea.10 11 It is also well established that CPAP is a useful form of treatment in both adults and children with this problem.12 13
The larynx is the narrowest part of the neonatal airway. Although Mathew and colleagues14 documented high pharyngeal closure during mixed and obstructive apnoea in preterm infants, using pharyngeal catheters, Ruggins et al 15 showed that the entrance to the larynx was obstructed in preterm infants with problematic apnoea, due to adduction of the arytenoid masses and the aryepiglottic folds. These studies both suggest, therefore, that there is obstruction at both the laryngeal entrance and as a secondary phenomenon, in the pharynx. Whatever the site, CPAP may prevent apnoea by distending the upper airway, thus reducing airway closure. This study therefore aimed to assess the effects of 5 cm H2O of CPAP on the dimensions of the laryngeal opening.
Methods
A 2.2 mm fibre optic angioscope (Olympus PF-22) was used to visualise the laryngeal opening. The tip of the scope is flexible through about 120 degrees in one plane. This movement is controlled by a hand piece. The endoscope has a light source and is attached to a wide angle camera (OTV-S2 Olympus) which in turn is connected to a colour monitor so that images can be viewed continuously. The images from the screen were also recorded on a videotape recorder.
The technique required the presence of two investigators, one to pass and control the endoscope, the other to maintain the position of the baby, check the monitoring systems, provide suction, and record the readings of the video counter whenever CPAP was started or discontinued. A CPAP pressure of 5 cm H2O was used for all babies. Heart rate and transcutaneous saturation were recorded continuously.
If the babies were receiving oral feeds, their stomachs were aspirated to reduce the risk of aspiration. Oro-phayngeal suction was also carried out after the babies had been positioned supine, with mild neck extension using a neck support. While continuing to receive CPAP, the endoscope tip was passed through the lips into the mouth and passed to the pharynx. The flexible tip was then angulated so that the laryngeal opening was visible. The lips were closed around the endoscope so that a seal was maintained at all times during recordings. Once the baby had settled and recordings obtained of at least three respiratory cycles, the CPAP was discontinued without moving the nasal cannulae and further recordings of the laryngeal opening obtained. This procedure was repeated on at least two further occasions.
Images of the laryngeal opening were then displayed on a frame by frame basis to identify the instant in the respiratory cycle at which laryngeal cord abduction was at its greatest. An independent investigator, who was blind to whether the recording was during or after discontinuing CPAP, then measured the maximum width and length of the space bounded by the posterior laryngeal wall and the vocal cords (fig 1). The individual measurements on each baby were used to calculate the coefficient of variation of the measurement, both on and off CPAP. In each baby the measurements on and off CPAP were averaged separately. From these results the mean values for the whole group were calculated and the data for on and off CPAP compared using the paired Student’s t test. A value of p < 0.05 was regarded as significant. The 95% confidence intervals of the differences were calculated.
{kind=link}
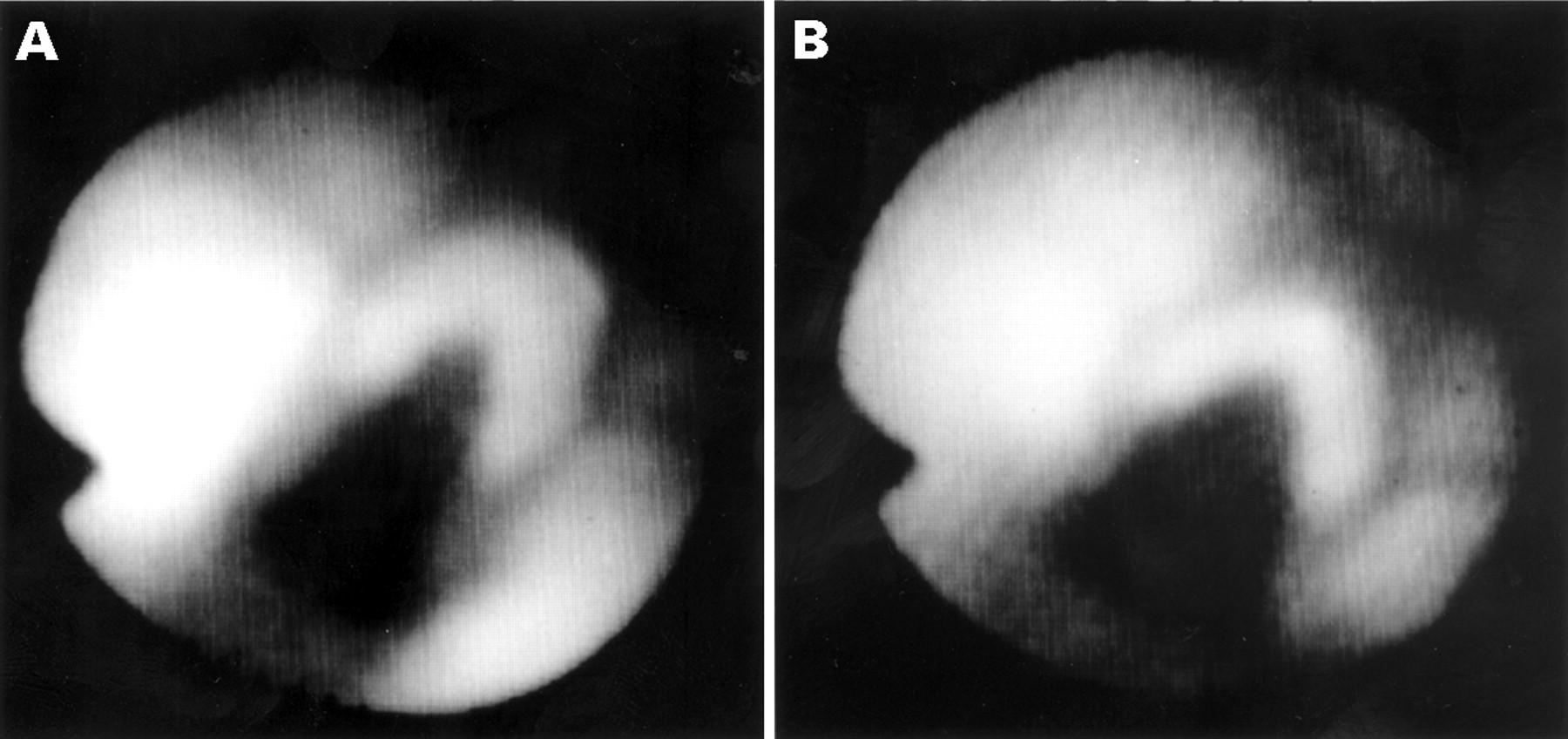
Photographs of maximal laryngeal opening: (A) off and (B) on CPAP in the same infant.
Nine babies were recruited. All were preterm with a mean gestational age of 28.8 weeks (range 24–35 weeks). Their mean birthweight was 1117 g (range 520–1840 g). At the time of study their mean age was 11.8 days (range 2–32 days). All the babies had previously been ventilated for RDS and had been extubated for at least 24 hours. All had received nasal CPAP using the EME flow driver for over 24 hours. The inspired oxygen concentration at the time of study ranged from 21 to 30%. Babies who were regarded as unstable were excluded. This included those with any evidence of sepsis, severe intraventricular haemorrhage, clinically significant patent ductus arteriosus, frequent apnoeas or desaturations, or metabolic or respiratory acidosis
The study was approved by the hospital ethics committee and informed, written consent was obtained from at least one parent of each baby.
Results
Initially the introduction of the endoscope stimulated a gag reflex but this was short lived and the babies tolerated the presence of the endoscope well. The picture obtained of the larynx was intermittently lost as a result of swallowing, the build up of secretions, or changes in posture of the baby. The mean number of breaths analysed in each baby was 6.1 on CPAP and 5.1 off CPAP.
Eight of the nine babies studied had a mean width:length ratio greater on than when off CPAP. (table 1). The mean difference in the ratio produced by CPAP for the total group was +24% with 95% confidence intervals of +12 to +37.1%.
Width:length ratios of the laryngeal opening, off and on CPAP (mean and coefficient of variation) and percentage change in ratio in nine infants studied
Discussion
Our results show that CPAP increases the laryngeal opening of preterm infants during inspiration. Direct measurements on pharyngeal structures cannot be made, using this technique, as there are no identifiable markers, and no means for directly calibrating the size of objects or spaces. We therefore used the ratio of the width to the length of the laryngeal opening during maximum abduction of the vocal cords. This consistently occurred during inspiration. Of the eight babies who showed this change in response to CPAP, the ratio of width to length increased by 12.5 to 47%. The remaining baby had a reduction of 6%. This represented less than half the mean coefficient of variation for the measurements off CPAP. We are unable to state the extent to which these changes are pressure sensitive as measurements were only obtained at a single pressure of 5 cm H2O.
Although CPAP could have produced these changes by stimulating greater abduction of the vocal cords, the most likely explanation for the changes observed is that CPAP has a distending effect on the upper airway, holding open the relatively compliant larynx of the preterm baby. Studies on adults show that this distending pressure would also prevent pharyngeal collapse, although for the reasons stated above, we were unable to confirm this due to the limitations of our technique. The implications of this study are that CPAP will tend to prevent spontaneous upper airway closure in preterm babies. We have evidence from our previous study11 that upper airway closure occurs at the entrance to the larynx both in mixed as well as obstructive apnoea. We postulate that this airway closure is an important aetiological factor in mixed apnoea, leading to significant deformation of the chest wall as the baby makes respiratory efforts against the obstructed airway. This will stimulate the central apnoea component of mixed apnoea via the intercostal–phrenic inhibitory reflex, a respiratory suppressant reflex produced by chest wall deformity.3 This is fully consistent with the findings of Miller and colleagues8 and goes some way to explaining their observation that CPAP only reduces the incidence of mixed and obstructive apnoea.
Our study could be criticised on the grounds that we did not select preterm babies who had troublesome apnoea, in whom it might have been possible to show a direct link between the observed changes and the prevention of apnoeic attacks. This would have been a more difficult and time consuming task, and we have no reason to consider that the changes would have been different. A further possible criticism is that all these babies had recently received intermittent positive pressure ventilation via an endotracheal tube which could have persisting effects on laryngeal function. This again we consider unlikely as all the babies had been extubated for over 24 hours.
In conclusion, we have shown that nasal CPAP tends to increase the width of the laryngeal opening, and consider that this provides an explanation for the selective preventive effect of CPAP on mixed and obstructive apnoea in preterm babies.
Acknowledgments
We thank the Tommy’s Campaign who generously funded S Lee, the Foundation for the Study of Infant Death who funded S Hannam, and provided the funds for the equipment, and The Special Trustees of St Thomas’s Hospital who funded D Ingram.