Article Text

Abstract
Objective: To study whether postnatal replacement of oestradiol and progesterone may help to prevent bronchopulmonary dysplasia (BPD).
Methods: This randomised placebo-controlled double-blind study enrolled 83 infants of <29 weeks gestational age and 1000 g birth weight requiring mechanical ventilation within 12 h after birth. Oestradiol (2.5 mg/kg/day) and progesterone (22.5 mg/kg/day) were given by continuous intravenous infusion of a standard lipid emulsion (15 ml/kg/day) in the replacement group (ESTRA-PRO). The placebo group received the same lipid emulsion without oestradiol or progesterone. A replacement period of at least 2 weeks but not >4 weeks was strived for and defined as “according to protocol”. The primary outcome variable was the incidence of BPD or death.
Results: The median birth weight was 670 g (min–max 400–990 g) and the gestational age 25 weeks (23.1–28.1 weeks). The incidence of BPD or death was 48% in the placebo group and 44% in the ESTRA-PRO group (p = 0.38, one-sided testing, intention to treat analysis). In infants treated according to protocol, 32% (9 of 28) in the placebo group and 14% (3 of 21) in the ESTRA-PRO group developed BPD (p = 0.08).
Conclusion: Replacement of oestradiol and progesterone was not effective for prevention of BPD or death in extremely preterm born infants. Better-powered trials are needed to evaluate this new approach.
- ATP, according to protocol
- BPD, bronchopulmonary dysplasia
- ESTRA-PRO, oestradiol and progesterone replacement
- ITT, intention to treat
- ROP, retinopathy of prematurity
- VEGF, vascular endothelial growth factor
Statistics from Altmetric.com
- ATP, according to protocol
- BPD, bronchopulmonary dysplasia
- ESTRA-PRO, oestradiol and progesterone replacement
- ITT, intention to treat
- ROP, retinopathy of prematurity
- VEGF, vascular endothelial growth factor
Bronchopulmonary dysplasia (BPD) remains a major factor for morbidity in extremely premature infants. The pathogenesis of BPD is multifactorial (eg the effect of mechanical ventilation, oxygen supply and inflammation on immature lung tissue), but has changed over the years so that the main hallmark of this condition is now reduced alveologenesis,1 as shown by histopathological studies in preterm infants dying from BPD who show an arrest of lung development.2 The concept has evolved that postnatal lung development in extremely preterm infants is arrested by a lack of factors that regulate lung differentiation and maturation in utero.
In a female rat model, it has been shown that ovariectomy reduced the gas exchange surface area by impaired formation of alveoli.3 This was prevented by oestrogen replacement. Moreover, ovariectomy-induced loss of alveoli could be regenerated by treatment with oestrogen.4 Oestrogen signalling by both known mammalian oestrogen receptors, ERα and ERβ, is required for alveolus formation, as ERα and ERβ knockout mice have diminished formation of alveoli during development.4 A decisive role of oestrogen and progesterone receptors in prenatal lung development is conceivable, as mRNA expression has been found to be highest in the prenatal mouse lung.5 Expression of ERβ has also been shown in the lung of the midgestational human fetus.6 The administration of oestradiol to pregnant rabbits increased alveolar maturation in the fetuses.7 Treatment of pig fetuses with oestrogen and progesterone receptor antagonists considerably impaired alveolar formation.8
It is known from umbilical cord blood measurements at different gestational ages that the human fetus is exposed to increasing amounts of both oestradiol and progesterone.9 Delivery disrupts the placental supply of these hormones. Within one day, the levels of oestradiol and progesterone decrease 100-fold.10 No other known biologically active steroid hormone shows these marked changes after birth; this is the physiological condition for the infant delivered at term. Preterm infants, however, are deprived of the placental supply of these hormones at a much earlier developmental stage. The oestradiol and progesterone withdrawn in preterm infants after delivery may be candidates for regulators lacking in postnatal lung development. Therefore, it is a reasonable approach to replace oestradiol and progesterone postnatally in extremely preterm infants who are most prone to develop BPD.
In a first randomised pilot study which focused on bone mineralisation, a trend towards a reduced incidence of BPD with the replacement was found,10 but in a Cochrane review of postnatal oestradiol and progesterone replacement, Hunt called for properly powered randomised controlled trials.11
INFANTS AND METHODS
Study infants
Infants admitted to the Section of Neonatology and Pediatric Critical Care, University of Ulm, Ulm, Germany, were enrolled in the study if the following criteria were fulfilled:
1. Gestational age <29 weeks.
2. Birth weight <1000 g.
3. Need for mechanical ventilation within the first 12 h of life.
4. Written informed consent of the parents.
Exclusion criteria were congenital malformations and chromosomal anomalies. This study was approved by the local ethics committee of the University of Ulm. It was based on the Guidelines for Good Clinical Practice and is in accordance with the Declaration of Helsinki.
Study design
This randomised, double-blind study had two parallel groups. Randomisation of the infants to the two treatment groups was carried out in the Department of Biometry and Medical Documentation of the University of Ulm (MK), ensuring that two of four consecutive patients were from each study group. Two study emulsions were supplied by the hospital pharmacy and infused at the same rate of 15 ml/kg/day:
1. ESTRA-PRO emulsion (Lipofundin 20%; B Braun, Melsungen, Germany; diluted with water to 5% (0.75 g/kg/day lipids) and containing 0.165 g/l oestradiol hemihydrate (2.5 mg/kg/day) and 1.5 g/l progesterone (22.5 mg/kg/day)).
2. The placebo emulsion contained the same amount of lipids, but no hormones.
The two study emulsions had identical appearance. We strived for a replacement time of 14–28 days. Infants who met this criterion formed the “according to protocol” (ATP) group. Infusion of the study emulsion was discontinued when there was no longer clinical indication for intravenous access.
Outcome variables
The primary outcome variable was BPD or death. BPD was defined as an oxygen saturation of <90% in room air for more than 30 min at a postmenstrual age of 36 weeks. Table 2 gives the secondary outcome variables.
Maintenance of in utero levels of oestradiol and progesterone by ESTRA-PRO
To document the maintenance of in utero levels of oestradiol and progesterone, these hormones were measured in plasma samples taken 1, 3 and 7 days after birth and, thereafter, once a week as long as the study emulsion was given, using the radioimmunoassay technique (17β Oestradiol 125I RIA Kit, Progesterone 125I RIA Kit; ICN Biomedicals, Costa Mesa, California, USA).12
Tolerability of the study emulsion and adverse events
Plasma triglyceride levels were determined every 2–3 days during the administration of the study emulsion. Hypertriglyceridaemia was defined as a triglyceride level >3 mmol/l. In the case of hypertriglyceridaemia, all other parenteral lipid administration other than the study emulsion was stopped. If hypertriglyceridaemia persisted for 12 h, administration of the study emulsion was stopped (violation of protocol). The incidence of cholestasis, hepatic cirrhosis and thrombosis was documented as adverse events.
Statistical analysis
In the pilot study,10 the incidence of BPD according to the definition at that time (requirement for additional oxygen later than the 36th week of postmenstrual age) was 29% in the placebo group. We expected to select a population with a higher risk of developing BPD when using the need for mechanical ventilation within 12 h after birth as an additional inclusion criterion. The Epicure study13 reported 74% additional oxygen requirement at 36 weeks postmenstrual age for infants of <26 weeks gestational age. On the basis of this information, we expected the incidence of BPD to be about 60% in our study. In our pilot study,10 there was no infant with BPD in the ESTRA-PRO group compared with four (29%) infants in the control group. To halve the incidence from 60% to 30% with oestradiol and progesterone replacement seemed an appropriate estimate and a clinically relevant difference. A sample size of 40 infants in each group was calculated (α = 0.05 one sided, power 80%). The outcome, incidence of BPD, that was shown to be reduced by the treatment in our pilot study was therefore tested with the one sided χ2 test to cut down the number of patients needed for confirmatory statistics.
For the descriptive statistical analysis, frequencies and percentages were calculated for qualitative characteristics, and median, minimum and maximum were given for quantitative characteristics. The primary end point was compared between treatment groups using a one-sided χ2 test. Secondary outcome variables were tested using either a two-sided χ2 test (or Fisher’s exact test if frequencies were small) or a two-sided Wilcoxon’s test for parallel groups. The dose–effect relationship between the occurrence of BPD at 36 weeks postmenstrual age and the duration of administration of the study emulsion was analysed by logistic regression taking into account possible confounders. The results are presented as odds ratios (ORs) with 95% confidence intervals (CIs) and p value of the Wald χ2 test. A p value of <0.05 was considered significant. Statistical analysis was carried out with SAS V.8.2.
RESULTS
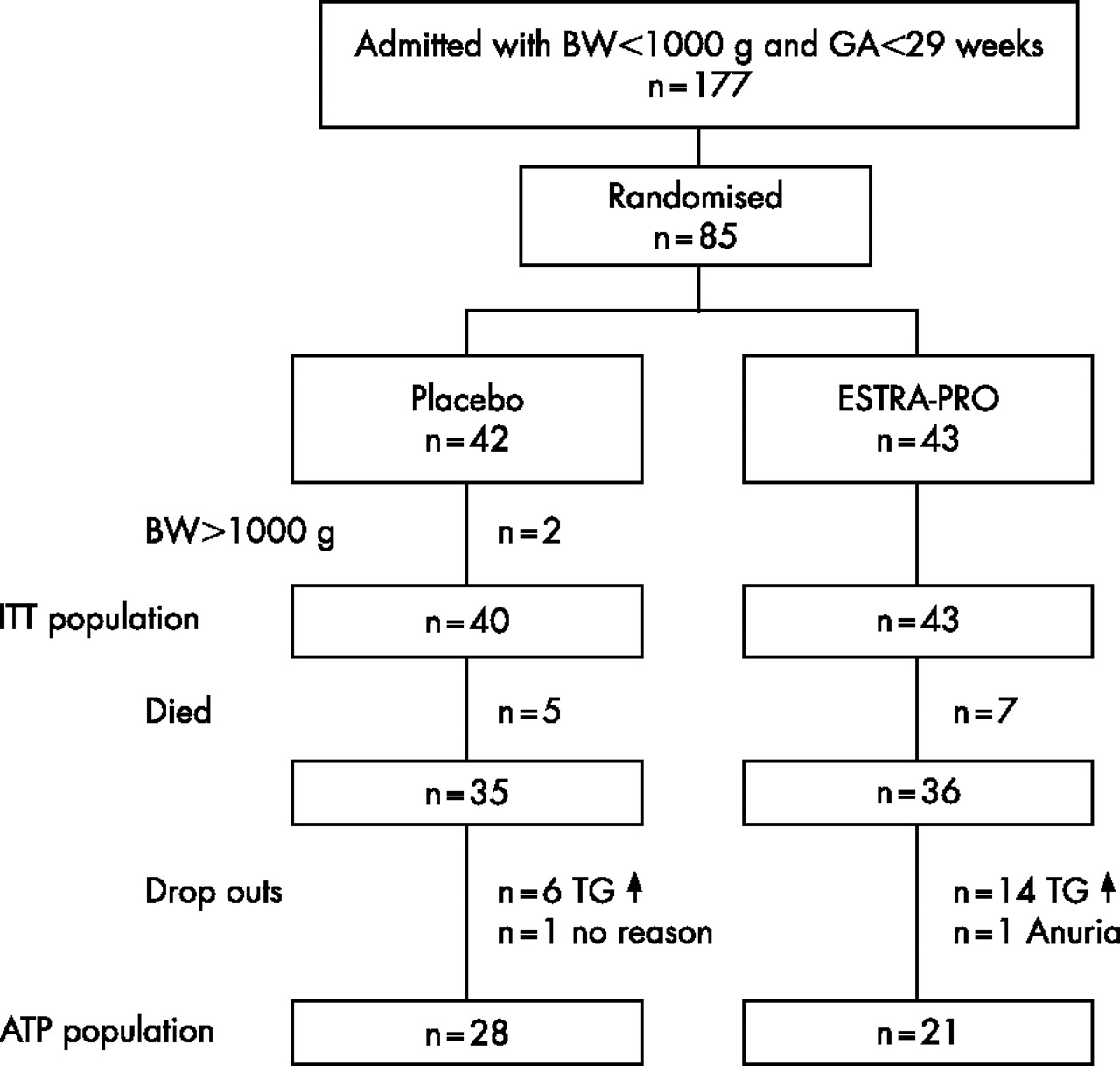
During the study period, from July 1999 through February 2003, 177 infants of <29 weeks gestational age and <1000 g birth weight were admitted. Many of the infants were not eligible for the study, as mechanical ventilation was not initiated within 12 h of birth. Eighty five infants were randomised, but inclusion criteria were violated in two infants with a birth weights of 1040 and 1110 g, respectively, leaving 83 infants (fig 1). No difference was seen in mortality between the groups (five of 40 (13%) in the placebo group v seven of 43 (16%) in the ESTRA-PRO group). A total of 11 of the 12 infants who died were not treated ATP because they died within the first 14 days. One infant (ESTRA-PRO group) treated ATP died 17 days after birth because of sepsis-associated respiratory failure. During administration of the study emulsion, seven (18%) infants from the placebo group and 16 (37%) infants from the ESTRA-PRO group developed hypertriglyceridaemia (p = 0.05, reason for stopping the administration of the study emulsion in six and 14 surviving infants, respectively). Administration of the study emulsion was stopped in one infant from the placebo group accidentally and in one infant from the ESTRA-PRO group because of anuria to minimise the fluid load. This left 28 infants in the placebo group and 21 infants in the ESTRA-PRO group for ATP analysis.

During the enrolment period, 177 patients with a birth weight (BW) of <1000 g and a gestational age (GA) of <29 weeks were admitted. Out of 85 infants, 42 were allocated to the placebo group (two drop-outs because violation of an inclusion criteria) and 43 to the ESTRA-PRO group (intention to treat (ITT) population). Of these 28 and 21, respectively, were treated according to protocol (ATP population). TG↑,hypertriglyceridaemia.
The two treatment groups showed similar baseline characteristics (table 1, ITT population). Baseline characteristics were similar for the ATP group (data not shown). The ITT analysis showed no difference for the primary outcome variable BPD or death (44% in the ESTRA-PRO group and 48% in the placebo group, p = 0.38, one-sided testing). For surviving infants treated ATP, the incidence of BPD in the ESTRA-PRO group was half that found in the placebo group (14% v 32%, p = 0.08). The incidence of BPD in surviving infants not treated ATP was five of seven (71%) infants in the placebo group and nine of 15 (60%) infants in the ESTRA-PRO group.
Characteristics of the infants in the intention to treat (ITT) population (placebo group n = 40, ESTRA-PRO group n = 43)
Table 2 gives a comparison of the secondary outcome variables for surviving infants. None of the infants of the ESTRA-PRO group developed severe retinopathy, whereas some in the placebo group did (p = 0.13, two-sided testing). Infants in the ESTRA-PRO group were discharged home earlier (p = 0.01) with correspondingly lower body weights (p = 0.03).
Secondary outcome variables of surviving infants for the ATP population (placebo group n = 28, ESTRA-PRO group n = 21; two sided testing)
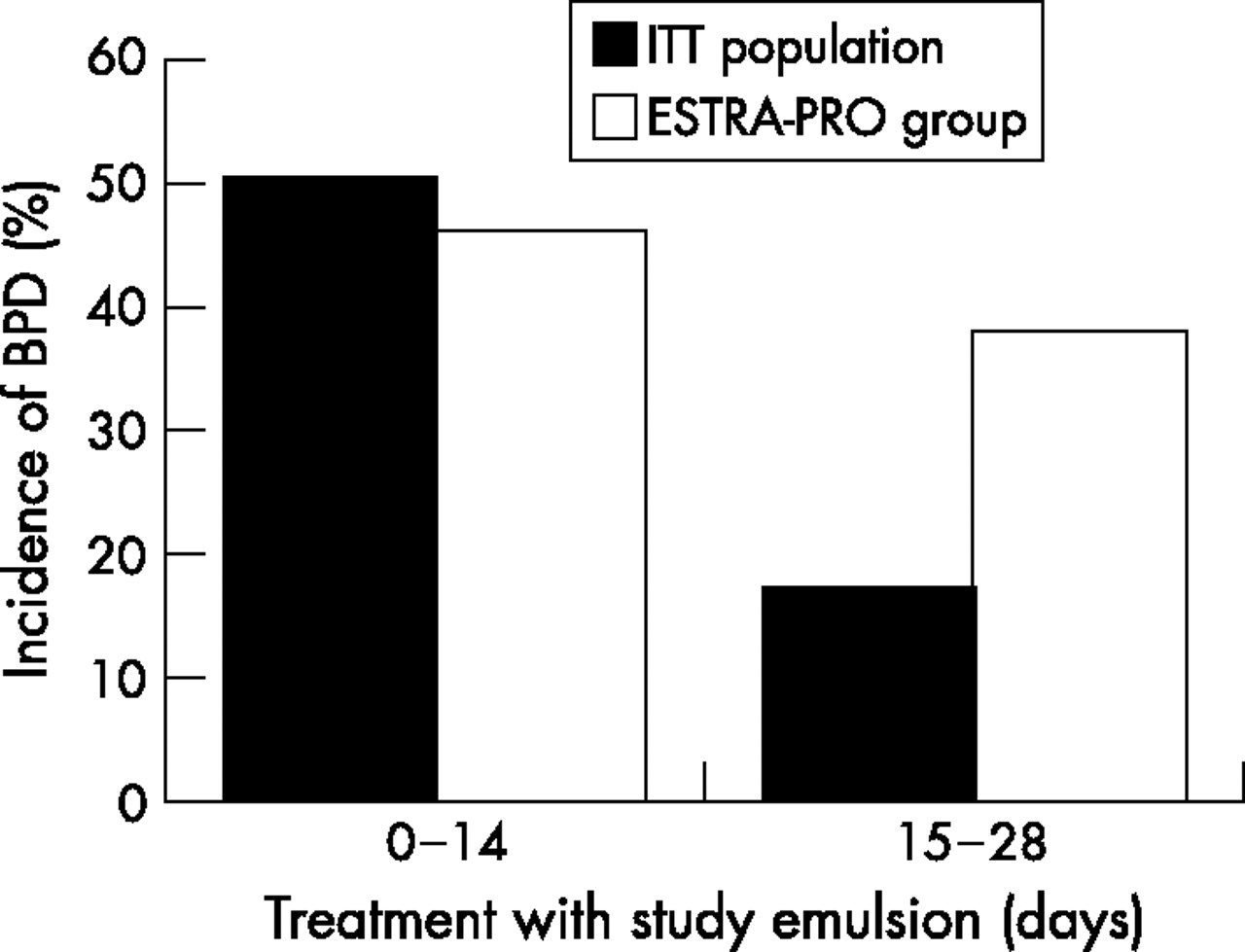
The dose–response relationship between “duration of administration of the study emulsion” and the outcome BPD was studied by logistic regression in all patients of the ESTRA-PRO group discharged alive (n = 36). Postnatal replacement of oestradiol and progesterone showed a significant dose–response relationship (OR = 0.9, 95% CI 0.8 to 1.0, p = 0.04). With every day of replacement, the odds of developing BPD was reduced by 10%. After adjustment for the potential confounders, gestational age ⩽24 weeks 6 days versus ⩾25 weeks (OR = 2.6, 95% CI 0.5 to 13.4, p = 0.24), and administration of dexamethasone, yes versus no (OR = 1.4, 95% CI 0.3 to 7.4, p = 0.67), the dose–response relationship remained nearly the same (OR = 0.9, 95% CI 0.8 to 1.0, p = 0.07). Figure 2 shows that the longer the administration of hormone replacement, the lower the risk of developing of BPD, an effect that was not present in the placebo group.
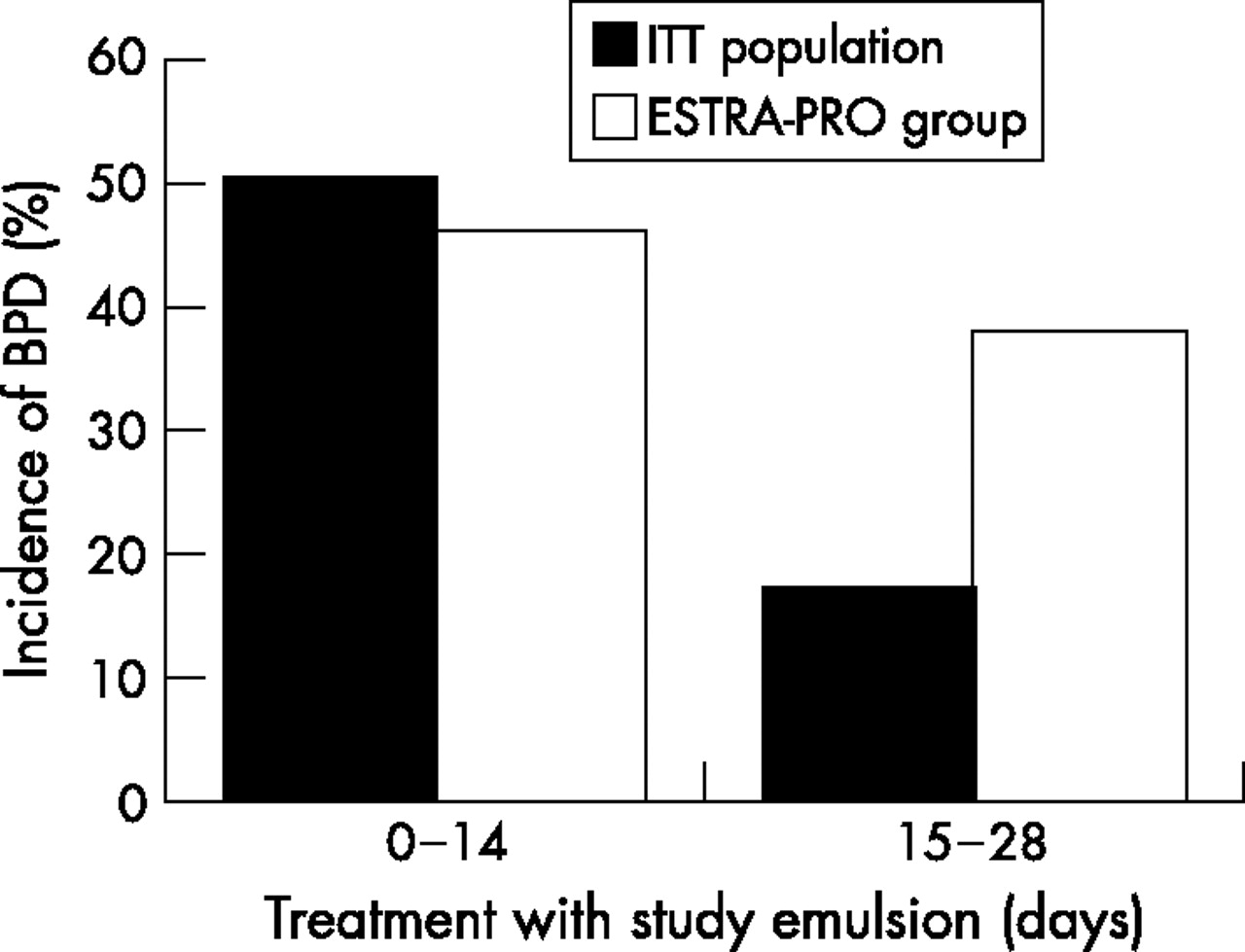
Dose–response relationship between the duration of administration of the study emulsion and the incidence of bonchopulmonary dyusplasia (BPD) ITT survivors, intention to treat; ESTRA-PRO, oestradiol and progesterone replacement.
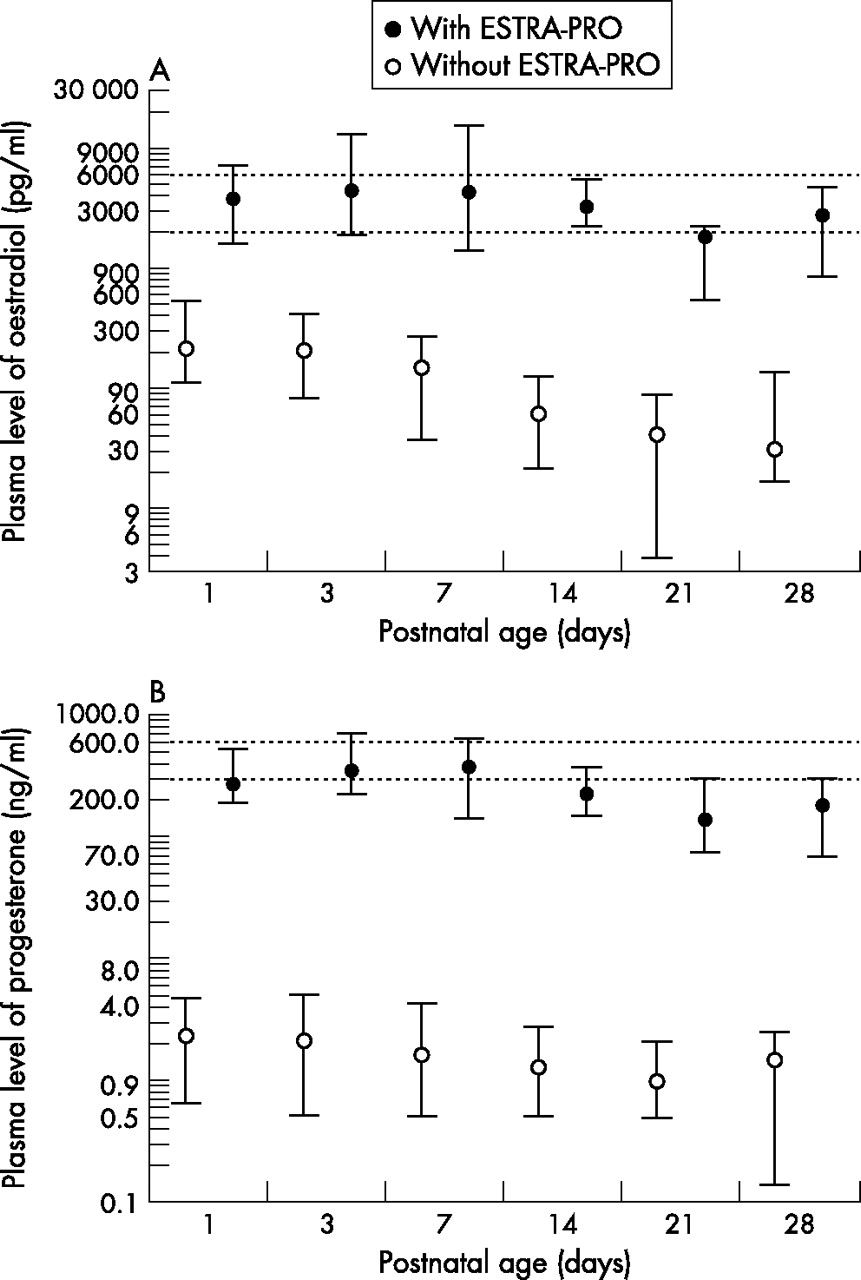
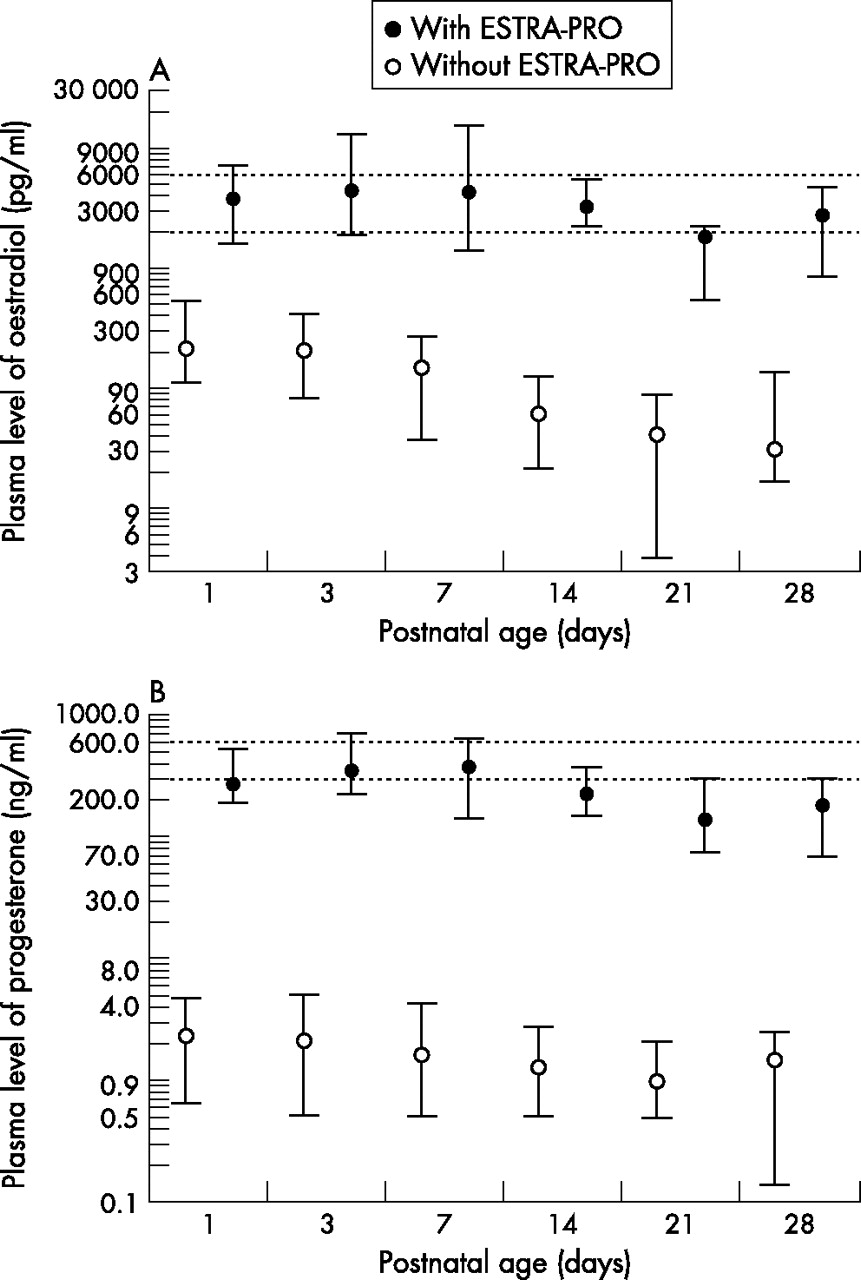
Plasma levels of oestradiol were widely maintained within the in utero ranges in the replacement group (dotted lines, fig 3A). Plasma levels of progesterone were also maintained, but showed a distinct decline after 2 weeks of treatment (fig 3B). The placebo group infants showed plasma oestradiol and progesterone levels 100-fold lower than the ESTRA-PRO group.
{kind=link}
{kind=link}
{kind=link}
Plasma levels of oestradiol (A) and progesterone (B) in preterm infants with and without replacement of oestradiol and progesterone at different postnatal ages. Medians, 10th and 90th centiles (conversion factors to SI –units, oestradiol ×3.67 and progesterone ×3.18). The dotted lines indicate the plasma levels of oestradiol and progesterone aimed at, which are derived from umbilical cord blood measurements.12 ESTRA-PRO, oestradiol and progesterone replacement
The incidence of adverse events was similar in the placebo and ESTRA-PRO group (cholestasis 6 v 3, liver cirrhosis 1 v 0, thrombosis 4 v 4, respectively, ITT population).
DISCUSSION
Maintenance of in utero plasma levels of oestradiol and progesterone was achieved with the ESTRA-PRO emulsion as in our previous study.10 Surviving infants who received the hormone replacement ATP showed a trend to less BPD (p = 0.08), which is in accordance with the result from the pilot study.10 The effect of the hormone replacement was associated with the number of days with hormone replacement (p = 0.04). Altogether, the goal of the study was not reached.
Twenty two infants survived but were not treated ATP. The incidence of BPD was higher in this subgroup (five of seven (71%) in the placebo group and nine of 15 (60%) in the ESTRA-PRO group) compared with 32% and 14%, respectively, in the ATP population. In this subgroup, increased markers of bacterial infection (for definition see table 1) were found postnatally in 91% (71% in the placebo and 100% in the ESTRA-PRO group) compared with 67% in the ATP group. Infection has been recognised as a risk factor for the development of BPD14 and may have contributed to the high rate of BPD in the non-ATP subgroup.
In the pilot study,10 there was no difference in plasma triglyceride levels between the replacement (mean 1.3 mmol/l, min–max 0.3–4.8 mmol/l) and the control group (1.47 mmol/l, 0.3–4.9 mmol/l) in the first 28 days after birth, and transient hypertriglyceridaemia (>3.0 mmol/l) was present in 20% of the infants of both groups (unpublished data). In this study, the incidence of hypertriglyceridaemia in the ESTRA-PRO group was twice as high as in the placebo group (p = 0.05). As all other parenteral lipid administration was stopped before withdrawal of the study emulsion, the difference in the incidence of hypertriglyceridaemia between the groups was not explained by a different total lipid supply. For a long time it has been known that plasma triglycerides rise markedly during pregnancy,15 and this was confirmed by more recent investigations.16 Removal of triglycerides may be impaired by diminished activity of lipolytic enzymes. The activity of lipoprotein lipase has been shown to be decreased in pregnant women.17 Oestradiol and progesterone have been shown to decrease the activity of lipoprotein lipase in vitro18 and in vivo.19,20 Possibly, the response to oestradiol and progesterone is the same in the preterm infant as in the mother, which decreases lipolysis and leads to hypertriglyceridaemia. Sepsis in preterm infants has been associated with reduced ability to use lipids,21 and this effect may be explained by downregulation of lipoprotein lipases.22 In the ESTRA-PRO group, there was a trend for higher rates of prolonged rupture of membranes (49% v 28%, p = 0.07, table 1) and increased markers of bacterial infections postnatally (81% v 65%, p = 0.14, table 1). This may provide an alternative explanation for the higher incidence of hypertriglyceridaemia. In addition, the higher rate of early-onset infections in the ESTRA-PRO group may have diminished the potentially beneficial effects of oestradiol and progesterone replacement on the incidence of BPD.14
Interestingly, none of the surviving infants of the ESTRA-PRO group treated ATP developed severe retinopathy of prematurity (ROP). This may be an incidental observation and ROP was not a primary outcome variable. However, in vitro and in vivo studies suggest that oestradiol may prevent ROP.23,24 Preterm birth leads to delayed retinal vascular growth with insufficient vascularisation. This results in hypoxia of the retina, with release of factors stimulating new and abnormal blood vessel growth.25 Vascular endothelial growth factor (VEGF) is an important oxygen-regulated factor that, if suppressed, inhibits normal vessel growth, but, if in excess, results in retinal neovascularisation. Recently, oestradiol has been shown to function as a significant stimulator of VEGF mRNA expression in retinal endothelial cells.23 In a mouse model of ROP, treatment with oestradiol under different oxygen conditions significantly improved retinopathy by acting on VEGF expression.24
Infants of the ESTRA-PRO group were discharged home nearly 2 weeks earlier (ITT and ATP population). Early discharge may be a surrogate for achievement of several conditions of preterm infants not further elaborated in this study. A role of oestradiol and progesterone in the prenatal development of the central nervous system is conceivable.26 The follow-up investigation of the infants of our first pilot study at the corrected age of 15 months showed improved psychomotor development in those infants who had received oestradiol and progesterone replacement after birth.27 Most recently, oestradiol has been recognised as a potentially preventive neuroprotective agent in sick preterm infants who need to be exposed to oxygen or drugs with neurotoxic side effects.28
Several limitations of the study need to be considered. A significant loss of study participants for the ATP analysis was observed because of hypertriglyceridaemia. A major flaw of this study is that we did not compensate for this. The incidence of multiple births in the placebo group was twice as high as found within the verum group (NS), which may have biased the results. On the other hand, no difference was found with regard to birth weight and gestational age between the groups. The protocol violations by hypertriglyceridaemia were seen more often in the replacement group, and this may have biased the results for the ATP analysis. However, the outcome BPD within the surviving dropouts was the same for both groups. Within the ATP population, postnatal dexamethasone was more often used in the ESTRA-PRO group. During the study period, criteria for use of dexamethasone were not strictly defined. Because the adjusted dose–response relationship between “duration of administration of the study emulsion” and the outcome BPD was virtually unaffected using dexamethasone as a potential confounder, we consider this difference to have occurred by chance. As in our pilot study,10 a trend towards reduced incidence of BPD was seen with the replacement if infants were treated ATP. No obvious serious adverse side effects were observed with the replacement, but lipid metabolism needs to be monitored carefully. Further basic research and sufficiently powered clinical trials are needed to evaluate this new approach in the management of preterm infants.
What is already known on this topic
-
From in vitro and animal models, it is known that oestradiol and progesterone may have a major effect on lung development and function.
What this study adds
-
This study adds clinical data that preterm infants may benefit in lung development from replacement of oestradiol and progesterone after birth
-
A larger better-powered study will be required to determine this reliably
Acknowledgments
We thank the “Deutsche Forschungsgesellschaft” for supporting this study. We also thank Mrs M Schulz (Endocrinological Laboratory, Department of Obstetrics and Gynecology, University of Ulm) for excellent technical assistance.
REFERENCES
Supplementary materials
Please find PDF of the edited version of figure 2.
Files in this Data Supplement:
Footnotes
-
Published Online First 11 August 2006
-
Funding: This work was supported by the “Deutsche Forschungsgesellschaft”, DFG 395/2-1, 2-2.
-
Competing interests: None.
Linked Articles
- Fantoms