Article Text

Abstract
Aims: To determine the relation between lower airway infection and inflammation, respiratory symptoms, and lung function in infants and young children with cystic fibrosis (CF).
Methods: A prospective study of children with CF aged younger than 3 years, diagnosed by a newborn screening programme. All were clinically stable and had testing as outpatients. Subjects underwent bronchial lavage (BL) and lung function testing by the raised volume rapid thoracoabdominal compression technique under general anaesthesia. BL fluid was cultured and analysed for neutrophil count, interleukin 8, and neutrophil elastase. Lung function was assessed by forced expiratory volume in 0.5, 0.75, and 1 second.
Results: Thirty six children with CF were tested on 54 occasions. Lower airway infection shown by BL was associated with a 10% reduction in FEV0.5 compared with subjects without infection. No relation was identified between airway inflammation and lung function. Daily moist cough within the week before testing was reported on 20/54 occasions, but in only seven (35%) was infection detected. Independent of either infection status or airway inflammation, those with daily cough had lower lung function than those without respiratory symptoms at the time of BL (mean adjusted FEV0.5 195 ml and 236 ml respectively).
Conclusions: In young children with CF, both respiratory symptoms and airway infection have independent, additive effects on lung function, unrelated to airway inflammation. Further studies are needed to understand the mechanisms of airway obstruction in these young patients.
- respiratory function test
- cystic fibrosis
- infection
- inflammation
- BL, bronchial lavage
- CBA, chocolate bacitracin agar
- CF, cystic fibrosis
- CFU, colony forming unit
- FEV, forced expiratory volume
- GEE, generalised estimating equation
- IL, interleukin
Statistics from Altmetric.com
- BL, bronchial lavage
- CBA, chocolate bacitracin agar
- CF, cystic fibrosis
- CFU, colony forming unit
- FEV, forced expiratory volume
- GEE, generalised estimating equation
- IL, interleukin
Children with cystic fibrosis (CF) have structurally normal lungs at birth,1 but lower airway infection and inflammation may be present from the first weeks of life.2–4 Little is known about how these changes within the airways affect lung function.
Studies of lung function in infants with CF have frequently shown abnormalities from early infancy. However, limited subject numbers and differences in subject selection or measures of lung function make meaningful comparisons difficult.5 Several studies show that infants with CF have normal thoracic gas volume, specific compliance, and conductance at birth, but by the first year of life some have evidence of hyperinflation, with reduced compliance and conductance.6–9 In particular, hyperinflation and airway obstruction may be found in young children with respiratory symptoms at the time of testing.8,10 Nevertheless, when using the more sensitive technique of raised volume rapid thoracoabdominal compression, reduced forced expiratory volumes have also been detected in asymptomatic infants.11 While it might be expected that airway infection plays a key role in the relation between lung function and respiratory symptoms, this has not been shown. Indeed, one recent study found lung function in CF infants was not influenced by a history of clinically recognised lower respiratory illness.12
The present study examined the relation between airway infection and inflammation, respiratory symptoms, and lung function in infants and young children with CF using bronchial lavage (BL) and the raised volume rapid thoracoabdominal compression technique. Subjects were recruited from a population based birth cohort identified by newborn CF screening and had at most mildly symptomatic lung disease.
METHODS
Participants
The state of Victoria, Australia, has a newborn screening programme for CF, with diagnosis confirmed by gene mutation analysis and sweat chloride ≥60 mmol/l. The Victorian CF Clinic manages all newly diagnosed infants at one of two affiliated hospitals. From January 1997 until December 1999, the parents of newborn infants and children aged younger than 3 years were approached as outpatients for consent to participate in the study. Children with tachypnoea, respiratory distress, or abnormal chest ausculatory findings at the time of testing were excluded, as were those whose clinical care was compromised by extreme social difficulties. Parents of all participants gave informed consent and the ethics committees of the Royal Children’s Hospital and Monash Medical Centre approved the study.
Testing was performed on an elective basis shortly after diagnosis and, in older children, as close as possible to the ages of 12, 24, or 36 months. At presentation for testing, parents were asked about respiratory symptoms in their child. For the purposes of the study, symptomatic children were those with a daily moist cough in the week prior to testing. Oral antibiotics given for this cough were also recorded. No child had received inhaled or systemic steroids, or ibuprofen.
Anthropomorphic measurements were compared with population normal ranges and converted to a standard deviation score, where each individual’s weight and height are expressed in units of the standard deviation of the population’s normal range for that measurement.13,14
Lung function testing
Lung function testing and bronchoscopy were performed under general anaesthesia, induced with sevofluorane gas or intravenous propofol, and maintained with intravenous propofol. Propofol has been shown in older children to have no effect on respiratory system resistance or compliance.15 Opioids and benzodiazepines were avoided because of their potential bronchodilating effects.
Lung function testing was performed using the raised volume rapid thoracoabdominal compression technique.11,16–18 Briefly, lung volume was raised above the tidal range to an inflation pressure of 20 cm H2O. Three raised volume breaths were delivered prior to thoracoabdominal compression by an inflatable jacket at end inspiration. The jacket inflation pressure was progressively increased in 5–10 cm H2O increments until a transmitted compression pressure of 20 cm H2O was measured at the airway opening during a 0.15 second airway occlusion. This produces a total standardised driving pressure for expiration of 40 cm H2O. The procedure was repeated until at least three technically satisfactory recordings had been made (no evidence of leak at the mask, adequate transmission pressure, and inflation and expiration uninterrupted by a sigh or glottic closure).19
Flow was measured using an infant pneumotachograph (Hans Rudolph series 3719, calibrated for 0–100 l/min) and forced expiratory volumes (FEV0.5, FEV0.75, and FEV1) were calculated by the LABDAT-ANADAT 5.2 data acquisition and analysis software package (Montreal, Canada). Despite setting of the delivered inflation pressure at 20 cm H2O, slight variability in the recorded pressure at the mask at end inspiration occurs.16 For this reason, forced expiratory volumes were standardised to an exact inflation pressure of 20 cm H2O using linear regression of forced expiratory volume versus inflation pressure for each individual, to allow for comparison of forced expiratory volumes between infants at the same inflation pressure.11,16
Bronchial lavage
Flexible bronchoscopy was performed immediately after lung function testing.4 As described previously,20 a single volume BL of 1 ml/kg of non-bacteriostatic normal saline was performed in the right middle lobe and repeated in the lingula. The lavage fluid from each site was pooled and transported on ice to the laboratory for immediate processing.
Laboratory methods
As previously reported,4,20 BL fluid was plated onto selective and non-selective media (horse blood, MacConkey, mannitol salt, chocolate bacitracin agar (CBA), cetrimide, and Burkholderia cepacia selective agar) for the counting and identification of respiratory pathogens by standard quantitative and qualitative microbiological methodologies respectively. Viral culture and immunofluorescence for a panel of respiratory viruses (influenza A and B, parainfluenza 1, 2, and 3, respiratory syncytial virus, and adenovirus) were also performed on BL fluid. Infection was defined by ≥105 colony forming units (CFU) of bacterial respiratory pathogens per ml of BL fluid20 or if respiratory viruses were detected. Airway inflammation was measured by total and differential cell counts, enzyme linked immunosorbent assay (ELISA) for interleukin 8 (IL-8), and chromogenic assay for free neutrophil elastase concentrations.4
Statistical methods
Between group comparisons of all variables were performed using regression models fitted by the method of generalised estimating equations (GEE) to allow for repeated measures on some subjects.21 A linear regression model was used for continuous outcomes (after log transformation where necessary), and a logistic regression model for dichotomous outcomes. These analyses provide natural generalisations of the standard approaches based on t test and χ2 to correlated data. This modelling approach was used to produce estimates of mean forced expiratory volumes by group, adjusted for height by analysis of covariance. Further adjustment for weight or gender did not affect results and was therefore not included. GEE was also used to examine the association between lung function and inflammatory markers. Raw values of IL-8 and free neutrophil elastase concentration exhibited positively skewed distributions, and logarithmic transformation was therefore performed prior to analysis by GEE. All analyses were performed using the Stata statistical software package.22
The intrasubject variability of the lung function measurements was calculated by one way analysis of variance following logarithmic transformation of the raw data recorded during technically acceptable manoeuvres.23 This produced an estimate of intrasubject variability for FEV0.5 of 5.1%.
RESULTS
Participants
Of 43 eligible children with CF attending the Royal Children’s Hospital CF clinic, 30 (70%) took part in the study, including 78% of those diagnosed following newborn screening. Six (14%) families were not approached because of either illness sufficiently severe to preclude elective general anaesthesia (n = 4) or extreme social difficulty (n = 2). The remaining seven families (16%) declined to be involved. Eleven additional children were recruited to the study: four who were born in 1995, two following transfer from other states, and five from the affiliated CF centre within the city. Of the 41 subjects recruited, five (12%) were subsequently excluded because of technically unsatisfactory lung function tests. Lung function testing and BL were performed on the remaining 36 subjects (21 females) on 54 occasions (14 were tested twice at different ages and two were tested on three occasions). Table 1 presents clinical characteristics.
Characteristics of 36 subjects with CF
Lung function in the whole group
No significant difference in lung function was found based on gender, homozygosity for the ΔF508 deletion, method of diagnosis, exposure to tobacco smoke in the home, or a family history of asthma. Ten children were tested aged 6 months or younger, and the lung function adjusted for height for these infants was not significantly different from the group as a whole (p = 0.76). Maternal smoking during pregnancy was associated with a mean FEV0.5 16% lower than in those who were not exposed (p = 0.08).
Relation between infection, inflammation, and lung function
Lower airway infection was detected by BL on 15/54 (28%) testing occasions in 13/36 (33%) subjects. Infection by a single pathogen was diagnosed on 11 occasions: Staphylococcus aureus in three, Hemophilus influenzae in four, Moraxella catarrhalis in one, Pseudomonas aeruginosa in two, and parainfluenza virus type 3 in one. Mixed infection was diagnosed on the remaining four occasions: P aeruginosa and H influenzae in one, and H influenzae and M catarrhalis in three.
Table 2 presents clinical characteristics, BL, and lung function results according to infection status. Children with lower airway infection were older, but the frequency of infection was not associated with gender, CF genotype, cigarette smoke exposure, or a parental history of asthma. Lower airway infection was associated with a reduction in forced expiratory volumes of approximately 10%. This difference only approached statistical significance for FEV0.5 (p = 0.06), but a difference of 10% is considered a clinically important difference and is twice the intrasubject variability. Small numbers precluded examination of lung function results according to infecting pathogen, however the lowest lung function was seen in a 20 month old child with P aeruginosa infection. Although BL inflammatory indices were increased among infected subjects, no direct relation was observed with lung function (p ≥ 0.1).
Clinical characteristics, bronchial lavage, and lung function results from 36 CF subjects on 54 occasions, by infection group
Respiratory symptoms and lung function
A moist cough over the previous week was reported at the time of testing on 20/54 (37%) occasions from 18/36 (50%) subjects. All children were otherwise well, and no subject had wheeze reported or detected on examination. Table 3 shows characteristics of children by symptom group. Infection was identified in a minority of BL specimens obtained from symptomatic children (7/20, 35%). Conversely, only 7/15 (47%) infections shown by BL were associated with symptoms, including all three subjects with P aeruginosa infection.
Clinical characteristics, bronchial lavage, and lung function results from 36 CF subjects on 54 occasions, by symptom group
Respiratory symptoms were associated with significantly reduced lung function (p ≤ 0.001).
The mean difference in FEV0.5 between the symptomatic and asymptomatic groups was nearly twice the magnitude of the infection related difference. No association was observed between gender, CF genotype, exposure to tobacco smoke, or parental history of asthma and the presence of respiratory symptoms (p > 0.1). Markers of inflammation were not increased in the children with respiratory symptoms (p > 0.5).
The majority of subjects with respiratory symptoms were receiving antibiotics (70%), but the results were not significantly affected by adjustment for antibiotic use in the regression analysis. Of the 13 children with daily cough in the absence of infection, nine (69%) were receiving oral antibiotics at the time of testing compared with 18/54 (33%) testing occasions in the CF group as a whole. However, only 2/13 (15%) had any respiratory pathogens detected by culture (102 CFU/mL S aureus and 103 CFU/ml P aeruginosa respectively). This finding, and the observation that inflammatory indices were not different between symptom groups, suggests that resolving or partially treated infection does not fully explain the lower lung function seen in children with respiratory symptoms.
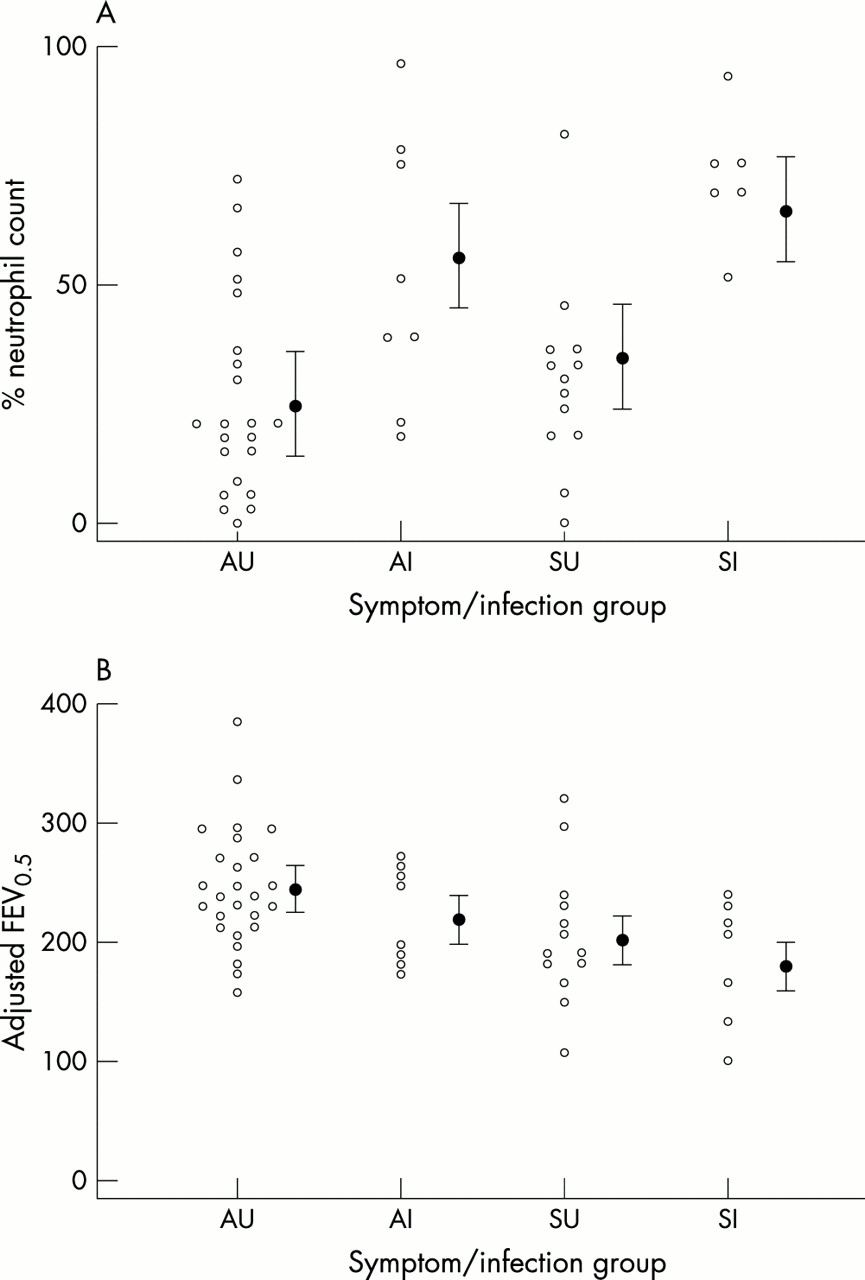
When the linear regression (GEE) method was used to examine the joint effect of infection and the presence of cough, the evidence for an association of infection with FEV0.5 was somewhat increased (p = 0.02 compared with unadjusted p value of 0.06), although the magnitude of the estimated differences (infected versus uninfected, and symptomatic versus asymptomatic) was unchanged. There was no evidence for an interaction effect, such as a greater difference between symptomatic and asymptomatic among those infected, although numbers were small for assessing this. Figure 1 shows neutrophil percentages for BL cell counts and FEV0.5 results in a subgroup analysis including both symptoms and infection.
{kind=link}
(A) Neutrophil percentages in bronchial lavage fluid, by symptom and infection group. AU, asymptomatic/uninfected (n = 22); AI, asymptomatic/infected (n = 8); SU, symptomatic/uninfected (n = 13); SI, symptomatic/infected (n = 6). Open circles represent individual values; closed circles are geometric means following adjustment for repeated measures, with 95% CI. (B) Lung function by symptom and infection group. Open circles represent individual values for each subject; closed circles represent the mean FEV0.5 adjusted by analysis of variance for height for each group, with 95% CI. AU, n = 26; AI, n = 8; SU, n = 13; SI, n = 6).
DISCUSSION
This study examines the relation between lung function and lower airway infection in a CF population aged younger than 3 years who were diagnosed principally by newborn screening and where BL identified infection. At the time of testing the children were clinically stable with at most mildly symptomatic lung disease. The study confirms earlier reports of lower lung function in some infants with CF,11,12,24,25 in particular, those with respiratory symptoms.26,27 It extends those findings by showing that airway infection and inflammation do not fully explain the reduced lung function previously described in infants and young children with respiratory symptoms. Lower respiratory infection and respiratory symptoms had an independent and additive adverse effect on lung function, which was not related to the degree of airway inflammation.
Another recently published study from Australia also used BL to examine the relation between lower airway infection and lung function.28 Tests were performed in 22 infants and young children with CF and an association between abnormal lung function (reduced respiratory system compliance and air trapping) and bacterial load was detected. However, unlike our study, there was also a correlation between reduced lung function and airway inflammation. Unfortunately, the relation between respiratory symptoms and lung function was not examined. These contradictions in results might be explained by differences in study subjects. Overall, the children in that study were slightly older and sicker (73% had chronic respiratory symptoms and 27% had P aeruginosa infection), with evidence of greater airway inflammation, than subjects in the current study. This suggests more advanced lung disease was present. It is possible that chronic infection and established inflammation masked other effects on lung function. In contrast, our younger study population with minimal CF lung disease allowed a greater opportunity to identify other potential influences on lung function.
Several explanations are possible for the reduced lung function seen in the symptomatic group in this study. In accordance with advice given to parents in our clinic, most children with moist cough had started oral antibiotics before bronchoscopy. This raises the possibility of partially treated or resolving infection in the symptomatic, but uninfected children. However, only two subjects in this group had detectable pathogens on BL, and inflammatory markers were no different between symptomatic and asymptomatic participants. Moreover, findings were unaltered by adjustment for antibiotic use. Previous studies in our clinic population have indicated that oral antibiotics do not appear to alter BL culture results,20 and while there may be an unequal distribution of bacterial numbers within CF lungs, airway inflammatory changes are more likely to be generalised.29 Thus, partially treated infection is an unlikely explanation for the differences in lung function observed between the symptomatic and asymptomatic groups.
Airway inflammation may persist for a variable period following clearance of infection in CF,3,4 and may lead to cough and reduced lung function. No relation was apparent however, between markers of airway inflammation and lung function in this study, and markers of inflammation were not increased in symptomatic children. Gastro-oesophageal reflux is common in children with CF.30 No child in this study had clinical evidence of significant aspiration of gastric contents, but the possibility of reflux with microaspiration was not specifically examined. This condition might be expected to lead to both cough and reduced lung function accompanied by airway inflammation. The latter, however, was not increased in symptomatic children.
Factors other than airway infection and inflammation may contribute to small airways obstruction in infancy, such as impaired prenatal lung growth, reactive airways disease, increased airway wall thickness, and mucus plugging. In this study, no subjects were born preterm or had another respiratory disorder. Exposure to tobacco smoke in utero was associated with evidence of small airways obstruction, as it is in healthy infants.31,32 However, smoke exposure in utero or at home was not associated with increased cough and therefore cannot explain the reduced lung function in the symptomatic group. Familial atopic disease is also associated with lower lung function in infancy.32–34 No subjects were wheezy at the time of testing, but reactive airways disease cannot be excluded. However, children with asthmatic parents had neither lower lung function nor an increase in reported cough, making reactive airways disease an unlikely explanation for the study’s findings.
Bronchial wall thickening is one of the most frequent early findings on computed tomography of the lungs in children with CF,5 and may be expected to lead to airway obstruction detectable by lung function testing. While there were no differences between inflammatory markers in the BL fluid from children with or without respiratory symptoms, persisting abnormalities of the airway wall may still have been present in symptomatic subjects. Reduced lung function in symptomatic young children may then more accurately reflect established bronchial wall pathology than intraluminal inflammation. Alternatively, previous airway infection can also lead to persistent abnormalities in the quantity or quality of airway mucus,35,36 contributing to airway obstruction. Others have described increased highly sulphated mucin within airway secretions of adults with CF,37 its possible role in impaired mucociliary clearance,38 and association with bacterial burden and disease severity.35,39 Treatment with antibiotics and mucolytic therapy,27 or bronchodilators and chest physiotherapy,40 has been shown to improve lung function in infants with CF, suggesting that enhancing clearance of secretions may have a role in treatment of symptomatic infants and young children without airway infection.
Because of the invasive nature of the testing involved in this study, tests were only performed on an annual basis, precluding more detailed longitudinal tracking of changes in airway infection and inflammation, and in lung function. Therapeutic interventions were not standardised, but if anything, the symptomatic children had received more aggressive therapy, and despite this they had lower lung function.
In summary, lower respiratory infection and the presence of a moist daily cough in young children with mild CF lung disease are independently associated with a reduction in lung function that is not explained by airway inflammation. While respiratory infections still influence the prognosis of children with CF,41 this finding suggests that other factors that may contribute to cough, such as increased airway mucus or submucosal inflammation, should be considered. Further investigations into the underlying causes of cough and reduced lung function are essential for the development of new therapies to improve airway obstruction in young children with CF. Long term follow up of infants with respiratory symptoms in the absence of lower airway infection will help determine subsequent correlates of early cough and reduced lung function and their influence on the course of CF lung disease.
Acknowledgments
The authors thank the Department of Anaesthesia, Royal Children’s Hospital, Melbourne, for their assistance with BL and lung function testing. G Nixon received the Grand Lodge of New Zealand Freemasons Child Health Fellowship. The study was supported by a grant from the Murdoch Children’s Research Institute and the JB Were Charitable Fund, Melbourne.
REFERENCES
Linked Articles
- CORRECTION