Article Text

Abstract
BACKGROUND Involvement of the gut in chronic granulomatous disease (CGD) has been previously described and colitis highlighted. However, the nature and histopathology of the colitis are unclear and have been thought to be non-specific or similar to Crohn's disease.
METHODS Seven patients with CGD, suffering from gastrointestinal symptoms were prospectively studied.
RESULTS All patients had anaemia; other symptoms were failure to thrive (5/7) and diarrhoea (5/7). Most had microcytic anaemia (5/7), increased platelets (7/7), and increased erythrocyte sedimentation rate (6/6). Endoscopically there was a friable erythematous mucosa in 6/7. The histological features present in all patients consisted of a colitis with paucity of neutrophils, increased numbers of eosinophils, eosinophilic crypt abscesses, pigmented macrophages, and nuclear debris. In some granulomas were present (2/7).
CONCLUSIONS Colitis is a common cause of gastrointestinal symptoms in CGD and is caused by a non-infective inflammatory process. The histology has specific features, which are distinctive from those seen in Crohn's disease.
- chronic granulomatous disease
- colitis
- histology
- treatment
Statistics from Altmetric.com
Chronic granulomatous disease (CGD) is an inherited disorder characterised by an inability of phagocytes to kill ingested catalase positive microorganisms; it leads to frequent severe bacterial or fungal infections. Since the first description of CGD in 1954 by Janeway and colleagues,1 a number of case reports of patients with CGD and gut disorder have been described. Occasionally colitis has been reported.2-4 It has been suggested that the colitis may be an unusual association,4 ,5 or that it might be caused by infection,3 ,6 or that it is a manifestation of CGD.5-7 In a recent literature review of gastrointestinal (GI) manifestations in CGD, it was estimated that 50% of patients had intestinal obstruction or anal fissure and diarrhoea. In approximately 20% of cases perirectal abscesses were seen.7 The reported histopathological features of colitis in CGD are contradictory, sometimes being described as indistinguishable from Crohn's disease,8-10 and at other times quite different2 ,3 and non-specific.6In this study children with CGD and GI symptoms underwent colonoscopy to determine the involvement of the colon and to document the nature of the colitis.
Patients and methods
PATIENTS
We studied seven unrelated children, five boys and two girls, aged between 2 years and 8 years 4 months, affected by CGD who presented to Great Ormond Street Children's Hospital between 1993 and 1998 with GI symptoms (table 1). The diagnosis of CGD was made between 1 day and 30 months of age by the nitroblue tetrazolium (NBT) test.11Two patients were tested at birth because of the past family history. All five boys had an X linked CGD with abnormalities of gp91phox subunit of NADPH oxidase,12 detailed in table 1. Cases 2, 5, and 6 had single amino acid substitution, but had no oxidase function (0% NBT). The girls carried an autosomal trait, affecting either neutrophil cytosolic factor 1 or 2 (NCF1 or NCF2) genes, which code for p47phox or p67phoxsubunits respectively.13 ,14 All the children in the study suffered from intestinal symptoms from a minimum of 3 months up to 4.5 years prior to referral to us. The patients have been followed up for a maximum of five years.
Clinical characteristics of patients
CLINICAL METHODS
Children included in the study had GI symptoms and underwent ileoscopy and colonoscopy. Biopsy specimens were taken from the ileum and all regions of the colon. This study was approved by the ethical committee and informed consent was obtained for the investigations carried out.
LABORATORY METHODS
Histology
Biopsy specimens were fixed in 10% buffered formalin and processed into paraffin wax. Light microscopical examination of 4 μm thick haematoxylin and eosin stained sections was performed prospectively in a blinded randomised fashion by an experienced paediatric histopathologist and a paediatric gastroenterologist. Each specimen was classified using the guidelines for the Initial Biopsy Diagnosis of Suspected Chronic Idiopathic Inflammatory Bowel Disease of the British Society of Gastroenterology.15
DNA testing
Molecular characterisation was carried out at the Central Laboratory of the Netherlands Red Cross Blood Transfusion Service (see table 2).
Histological findings in patients
Results
CLINICAL
The patients had GI symptoms at the time of endoscopy; table 1presents a summary of the other relevant clinical information. The mean age of the onset of GI symptoms was 18 months (range: 1 month to 5 years). The mean time between the onset of GI symptoms and investigation was 21 months (range: 3 months to 4.5 years). Classical signs and symptoms of inflammatory bowel disease with bloody diarrhoea were present in five of the seven patients. Five had failed to thrive, and two had mouth ulcers. Other GI manifestations noted were abdominal distension, constipation, vomiting, anal skin tags, and recurrent perianal abscess.
Anaemia was a common feature in all patients at presentation, with a mean haemoglobin of 79 g/l. Two patients, one of whom had bloody diarrhoea, required blood transfusion (cases 5 and 7). Anaemia was present before GI symptoms became apparent. In five of the patients the anaemia was microcytic; they were treated with oral iron supplements, without resolution of the anaemia. None of the patients presented with eosinophilia at the time of investigation. Six of seven patients had increased platelets ranging from 457 to 897 × 109/l. Erythrocyte sedimentation rate ranged from 13 to 100 mm/h. IgE was increased in four of five children, ranging from 91.9 to 983 UI/ml. Two children had a personal history of atopy. Stools were cultured repeatedly and examined for cysts, ova, and parasites. No pathogenic organisms were isolated, including Staphylococcus aureus or Clostridium difficile.
At endoscopy the colon was diffusely erythematous throughout in six patients. Occasional ulcers were seen in three patients. Interestingly in one patient the colon appeared completely normal.
HISTOLOGY
Histological examination showed distinct and specific features (see table 2).
All seven patients had evidence of a diffuse colitis involving all regions of the colon with differing degrees of severity. Cases 4 and 7 were clearly less severe than the other cases. Areas of flattened inflamed surface epithelium were seen in all patients and nuclear debris was apparent in the epithelial cells as well as in the underlying superficial lamina propria, but this was less notable in cases 4 and 7. Microscopic ulcers exuding eosinophilic pus were a feature in one patient (fig 1). Cryptitis, in some cases caused by eosinophils, was present in five and crypt abscesses were noted in two patients. The inflammatory cells in the lamina propria in all seven patients were mostly degranulating eosinophils, large macrophages, and lymphocytes. Many of the eosinophils were degranulating and free eosinophilic granules were present in the lamina propria. Apart from eosinophils the other major component of the inflammatory infiltrate was large macrophages which had either brown granular cytoplasm or pink eosinophilic crystalline cytoplasmic inclusions (fig 2). A distinctive and common feature was the paucity of neutrophils in all patients, making this colitis different from that seen in other forms of inflammatory bowel disease. Epitheloid granulomas were encountered in only two patients. One of these, case 2, had exuberant granulomas throughout the colon, replacing large areas of the lamina propria. In the other (case 5), only a few granulomas were seen in the left colon. Plump, possibly activated endothelial cells were a common feature and eosinophils were seen to traffic freely through the vessel walls, as they did through the mucosal epithelium (fig 3).
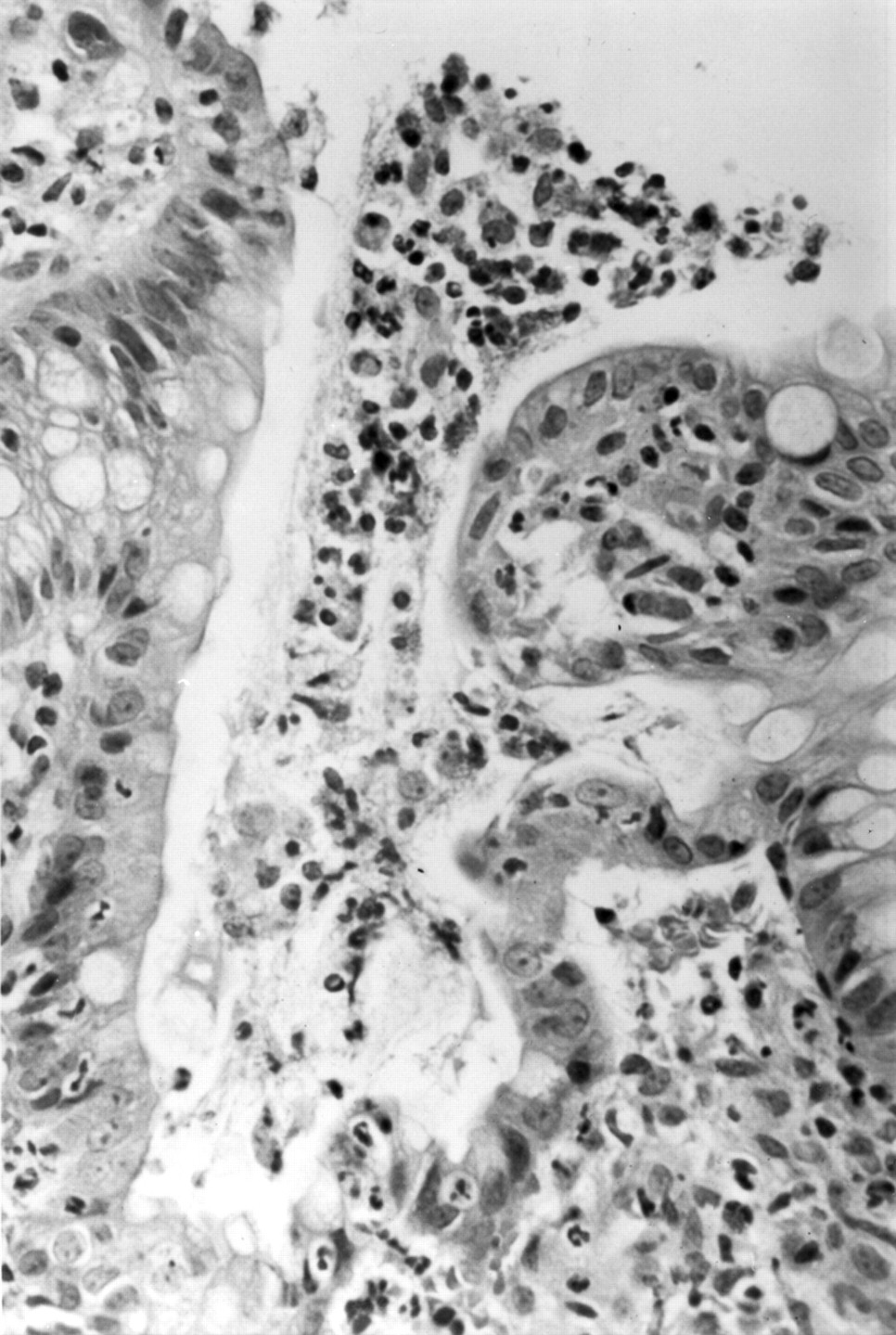
Sections of colonic mucosa showing a microulcer exuding pus containing eosinophils. Haematoxylin and eosin stain. Original magnification × 500.

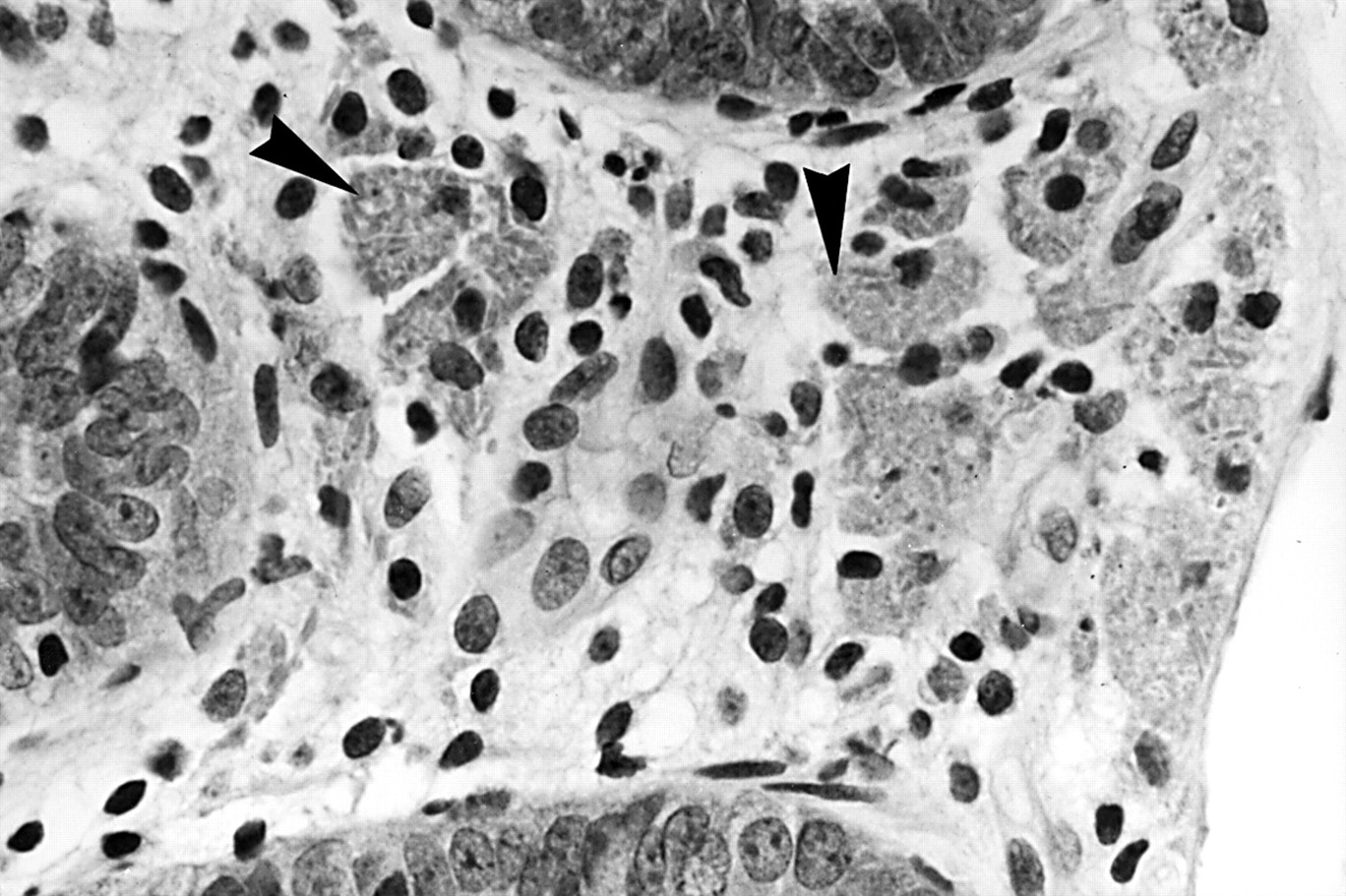
Colonic mucosal lamina propria showing the presence of many large macrophages with eosinophilic crystalline inclusions (arrowheads). Haematoxylin and eosin stain. Original magnification × 800.

{kind=link}
{kind=link}
{kind=link}
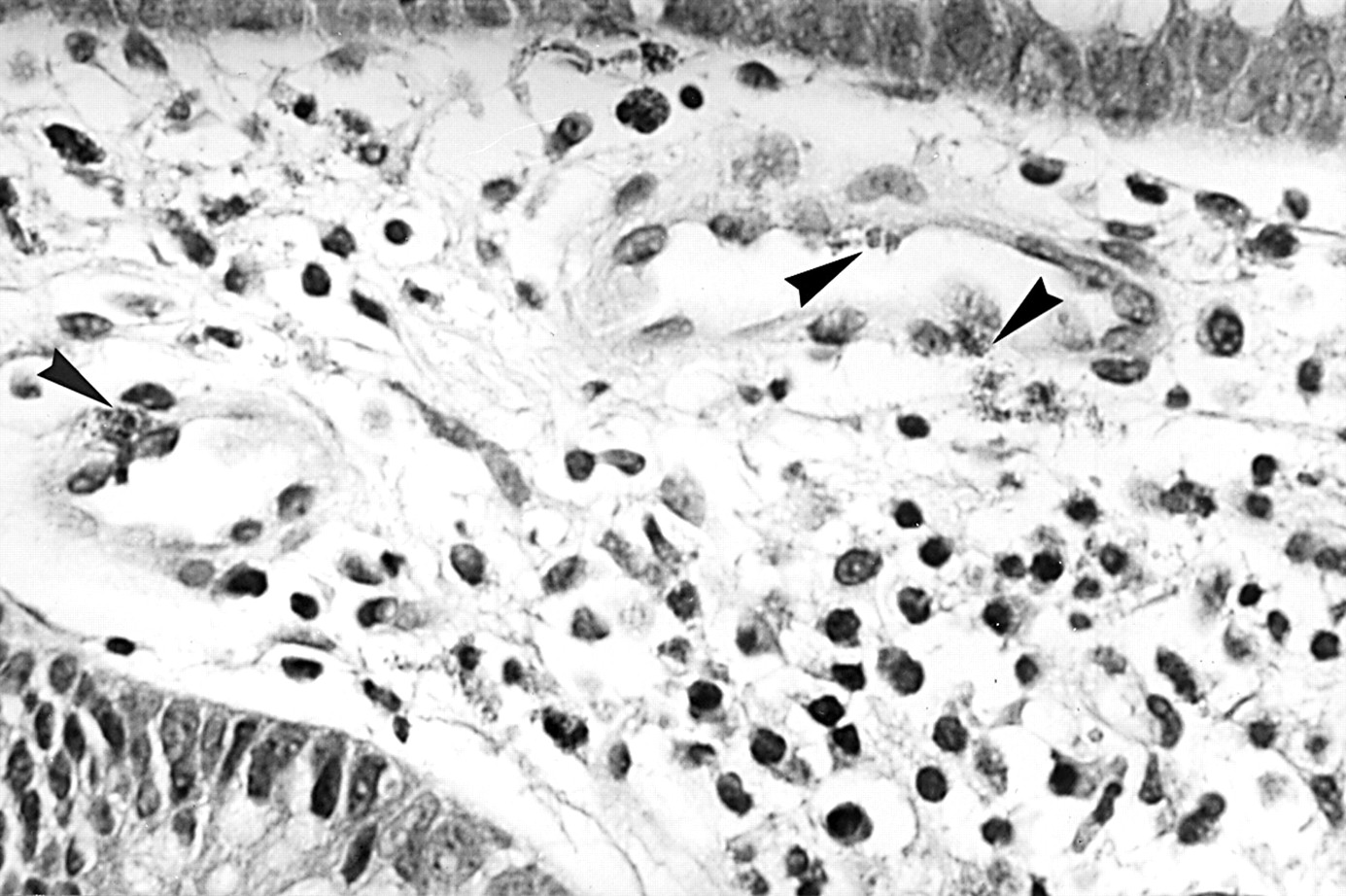
Colonic mucosal lamina propria showing blood vessels with plump endothelial cell nuclei. Eosinophils (arrowheads) are seen to migrate through the vessel walls. Haematoxylin and eosin stain. Original magnification × 800.
TREATMENT
All patients were on co-trimoxazole as a prophylactic antibiotic for their underlying condition. Six of the seven patients were also taking itraconazole at the time of the GI investigations. In four patients (cases 1–4) sulphasalazine was added to their therapy after the biopsies showed evidence of colitis. Three responded well and did not need any other treatment. Case 4 continued to have bloody diarrhoea and was commenced on antibiotics (metronidazole and ciprofloxacin), without success. She was then put on low doses of prednisolone and azathioprine, which dramatically improved her symptoms.
Two patients were treated with metronidazole and ciprofloxacin as a first choice of treatment. Although the GI symptoms disappeared after one course in one of them (case 7), this treatment could also have been potentiated by the immunosuppressive therapy she was receiving for another problem (cyclosporine A for a liver transplant). The other child needs further investigations, because of the recurrence of the symptoms.
The last patient was in a poor nutritional state, with height between the 25th and 50th centiles and weight below the 3rd centile. His blood showed low copper, zinc, iron, and selenium concentrations. For this reasons overnight feeds were introduced and he received a course of isoniazid and rifampicin initially, but the diarrhoea persisted. He was then given mesalazine, which resulted in resolution of his symptoms.
Discussion
We have shown that if a patient with CGD suffers from anaemia or fails to thrive, in addition to searching for occult infection, GI investigation including colonoscopy is required. In all seven patients studied with anaemia and/or failure to thrive, GI disease was present in the form of colitis. Interestingly macroscopic endoscopic examination gave insufficient information and in one case was misleadingly normal (case 6). Our study shows that as with other colitic disorders, biopsies should always be performed and histopathological investigations undertaken.
The histopathology of the colitis was similar in all patients, even if the severity differed from one case or one region of the colon to another. The most specific features were the apparent paucity of neutrophils and the eosinophilic inflammatory infiltrate, together with large pigment containing macrophages. The degranulating eosinophils appeared as large clumps in the lamina propria, to which they gained access by trafficking through its microvasculature. The vascular endothelium appeared plump and apparently activated to allow eosinophils to pass through. They were also present in the epithelium, causing cryptitis and crypt abscesses. Our observations would suggest that the inflammatory response in CGD promotes eosinophilic involvement rather than neutrophils, but this study does not provide an explanation for this. We speculate that vascular endothelium and epithelium express adhesion molecules, which allow activated eosinophils to traffic through vessels and epithelium rather than neutrophils. Several studies have suggested that eosinophil products from degranulating eosinophils play an active role in the production of the gut tissue injury.16-19 In eosinophilic gastroenteropathy, there are increased numbers of activated and degranulating eosinophils associated with the enterocolitis.19 In asthmatic patients there is evidence that eosinophil products contribute to bronchial epithelial damage.20 ,21 The increased number of eosinophils in the gut of our patients was not associated with peripheral blood eosinophilia. The high IgE concentrations are difficult to interpret as in all four patients with a raised IgE, there was a personal history of atopy and RAST tests were positive in two of them. This suggests that the high IgE concentrations were caused by atopy rather than CGD.
Another important hallmark of this colitis are the granulomas, which resulted in the previous descriptions of a Crohn's like colitis.8 ,10 However, they were not seen in all patients but when present the accumulations of macrophages appeared to be both much more prominent and prolific than those seen in Crohn's disease. This feature, together with their pigment content and the lack of neutrophils makes them quite distinct from those observed in Crohn's disease.
Interestingly the severity of the colitis did not depend on either the age of the patient or on the length of time the patient has had GI symptoms. There may however be some relation between the histological phenotype and genotype. The autosomal recessive cases with absent p47phox or p67phox had less severe inflammation on histology than the X linked cases, with no granulomas and little nuclear debris in and under the epithelium. This did not appear to be a function of time or age. The numbers of cases are, however, small and this area merits further study.
It was surprising that more neutrophils were not seen in the lamina propria. It can only be assumed that neutrophils and endothelial cells were not activated to allow binding and passage of neutrophils through vessels into the lamina propria and that this required different molecules than those required for eosinophils. There do not appear to be any previous studies of the molecular nature of the inflammation in CGD, which would provide an explanation for the findings in our patients.
Treatment of the colitis in CGD is not well established; the literature does not provide clear recommendations as it mainly consists of single case reports.
In the past the excessive inflammatory response was believed to be in response to recurrent infections.7 Therefore, most patients have received an empirical course of antibiotics, perhaps combined with other treatments, which has produced a very variable response.2 ,4 When intestinal contents have been cultured they have usually been negative for bacterial growth or inconclusive,2 ,5 ,8 ,22 thus making infections an unlikely cause of the inflammatory process. However, we cannot exclude a triggering role for the normal flora nor for organisms not killed by CGD phagocytes.
Since the first descriptions of the disease, the colitis was believed to be an association with Crohn's disease. As a consequence, sulphasalazine has been used as a first line treatment.2 ,4 ,9 However, reports of the efficacy of sulphasalazine are contradictory, but in our study five of seven patients responded to a 5-acetylsalicylic acid (5-ASA) preparation. Immunosuppressive drugs have largely been avoided because they were regarded as dangerous in patients with defective neutrophils.7 Despite this there are some reports of the use of corticosteroids and cyclosporin.4 ,9 ,22 These drugs reduce the excessive inflammatory response by their effects on T lymphocytes, and thus eventually impair migration of granulocytes and macrophages.22 Rosh et aldescribed a case in which remission of colitis was obtained with cyclosporine, after steroids had failed to improve the symptoms.9 However, the patient experienced severe infective complications of the treatment and developed a life threatening pneumonia. We would recommend that a 5-ASA preparation be used for first line treatment, with immunosuppressive agents only being used when 5-ASA drugs fail to induce remission.
Colitis has also been described in other conditions with defective neutrophils, especially glycogen storage disease type 1b.23 ,24 Granulocyte colony stimulating factor (G-CSF) is helpful in this condition. This is a tempting approach, as it would avoid the disadvantage of further immunosuppression. Recently a course of G-CSF gave good results in two adult patients with CGD.25 The mechanism by which the G-CSF resulted in improvement of the colitis is however not clear.
We have shown that patients with CGD and a variety of GI symptoms may have severe colitis with unique histological features. Infection appears to play little role in the active stage, although we cannot rule out an infectious trigger. Treatment of the GI manifestations has been varied but our study shows that conventional anti-inflammatory treatments can be effective. The number of subjects in this study is however still quite small and larger numbers of patients are required if rational therapy is to be defined.
Acknowledgments
This work was undertaken by Great Ormond Street Hospital for Children NHS Trust who received a proportion of its funding from the NHS Executive; the views expressed in this publication are those of the authors and not necessarily those of the NHS Executive.