Article Text

Abstract
Objective To investigate the association between primary Sjögren's syndrome (pSS) and the risks of malignancy including overall malignancy and site-specific malignancies through a systematic review and meta-analysis.
Methods We searched Pubmed before January 2013, with a restriction to English language publications. Studies were included if they met the following criteria: (1) a cohort or observational study; (2) pSS as one of the exposure interests; (3) cancer as an outcome of interest; (4) relative risk (RR) or standardised incidence rate (SIR) with 95% CIs. We used a random or fixed effects model to calculate the pooled RR according to the heterogeneity test.
Results Fourteen studies involving more than 14 523 patients with pSS were included. Compared with the general population, patients with pSS had significantly increased risks of overall cancer (pooled RR 1.53; 95% CI 1.17 to 1.88), non-Hodgkin lymphoma (NHL) (pooled RR 13.76; 95% CI 8.53 to 18.99) and thyroid cancer (pooled RR 2.58; 95% CI 1.14 to 4.03). A significant association was found in various subgroup meta-analyses for NHL but, for overall malignancy, a significant association was only found in some groups. Additionally, the number of studies exploring the association of pSS with the risk of solid malignancies was so small that we could not carry out subgroup meta-analyses.
Conclusions This meta-analysis indicates that pSS is significantly associated with increased risks of overall malignancy, NHL and thyroid cancer. However, it is not yet known whether the apparent increased risk of overall malignancy in patients with pSS is due to the relatively high prevalence of NHL in that group.
- malignancy
- systematic review
- meta-analysis
Statistics from Altmetric.com
Primary Sjögren's syndrome (pSS) with a female preponderance is a systemic autoimmune disorder with secretory gland dysfunction characterised by dryness of the main mucosal surfaces including the mouth, eyes, nose and vagina.1 The disease is one of the three most common autoimmune disorders.2
Since Kassan et al3 first reported an increased risk of non-Hodgkin lymphoma (NHL) in patients with pSS, an increasing number of studies have explored this association. In 2005 the first meta-analysis preliminarily confirmed that pSS is closely associated with an increased risk of NHL development.4 However, the number of studies included in the previous meta-analysis was small (only five) and, since 2005, more studies have been published. Moreover, some studies also investigated the association between pSS and the risk of cancers other than NHL, although the results remained inconclusive. To obtain a better estimation of cancer risk in pSS, we carried out the present meta-analysis of all available cohort studies relating pSS to the risks of various cancers.
Materials and methods
PubMed was searched (updated to 31 December 2012) for English language articles by combinations of the following terms: ‘Sjögren's syndrome’, ‘SS’ and ‘cancer’, ‘malignancy’, ‘neoplasm’, ‘tumour’, ‘carcinoma’, ‘lymphoma’ and ‘relative risk’, ‘RR’, ‘standardised incidence rate’, ‘SIR’. All eligible articles were retrieved and their references were reviewed to identify additional relevant studies.
Studies were included if they fulfilled the following inclusion criteria: (1) a cohort or observational study; (2) pSS as one of the exposure interests; (3) cancer as one outcome of interest; (4) relative risk (RR) or standardised incidence rate (SIR) with 95% CIs available (or with data to calculate them). Studies were excluded if the effect size could not be calculated according to these studies.
All articles were retrieved and assessed independently by two reviewers (YL and ZY) who extracted data including authors, publication date, country of origin, characteristics of the study population including sex, age, diagnostic criteria for pSS, mean follow-up in years and other details of adjustment. Any disagreement was resolved by consensus.
Data extraction and statistical analysis
Publications that used established diagnostic criteria (table 1) for pSS and that reported RR or SIR with corresponding 95% CIs were selected for inclusion in the meta-analysis. The detailed method for calculating SIR and 95% CI has been described in a previous study.5 ,6
Characteristics of cohort studies on primary Sjögren's syndrome and risk of malignancies
Heterogeneity of effects across studies was assessed using the χ2 test statistic and quantified by I2, which represented the percentage of total variation across studies that was attributable to heterogeneity rather than chance.7 The pooled RR was estimated by a fixed effect model when there was no heterogeneity, otherwise a random effect model was used. If statistical heterogeneity was present, the Galbraith plot was used to detect potential sources of heterogeneity.8 Subgroup analyses were carried out according to region, diagnostic criteria for pSS, study design, mean age and mean duration of follow-up. A sensitivity analysis was performed to evaluate stability by sequential omission of individual studies. Publication bias was tested by the Egger linear regression test for funnel plot asymmetry and the Begg–Mazumdar test.9 All analyses were performed with STATA V.11.0 software.
Results
Characteristics of included studies
Of the 591 publications initially identified in PubMed, 14 studies were included in the meta-analysis (figure 1),3 ,10–22 8 involving 11 889 patients for overall malignancy, 11 involving 12 325 patients for NHL and 5 involving 10 953 patients for myeloma. Two studies were from Asia, two from the USA and 10 were from Europe (table 1).

Flowchart of study selection.
pSS and risk of overall malignancy
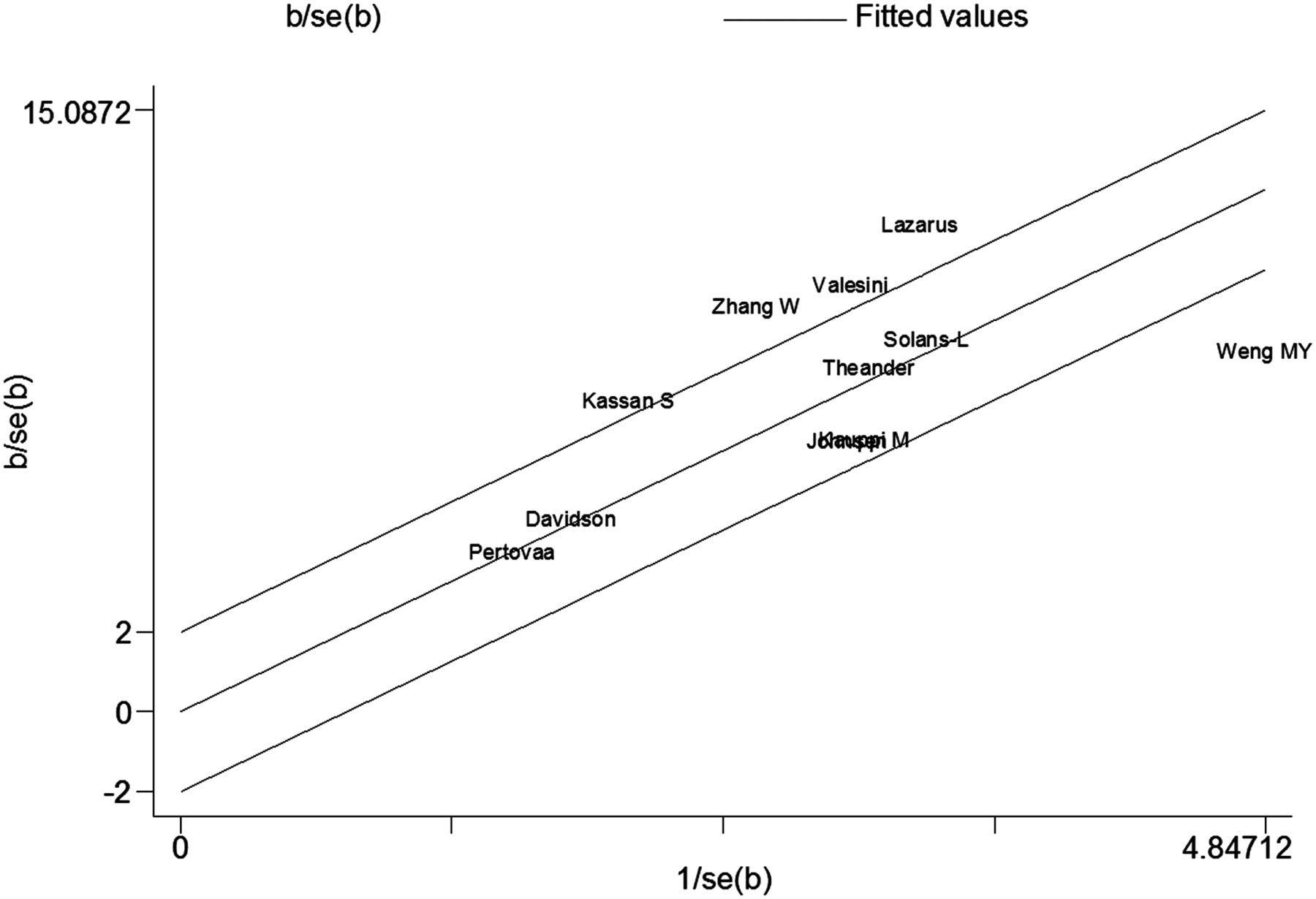
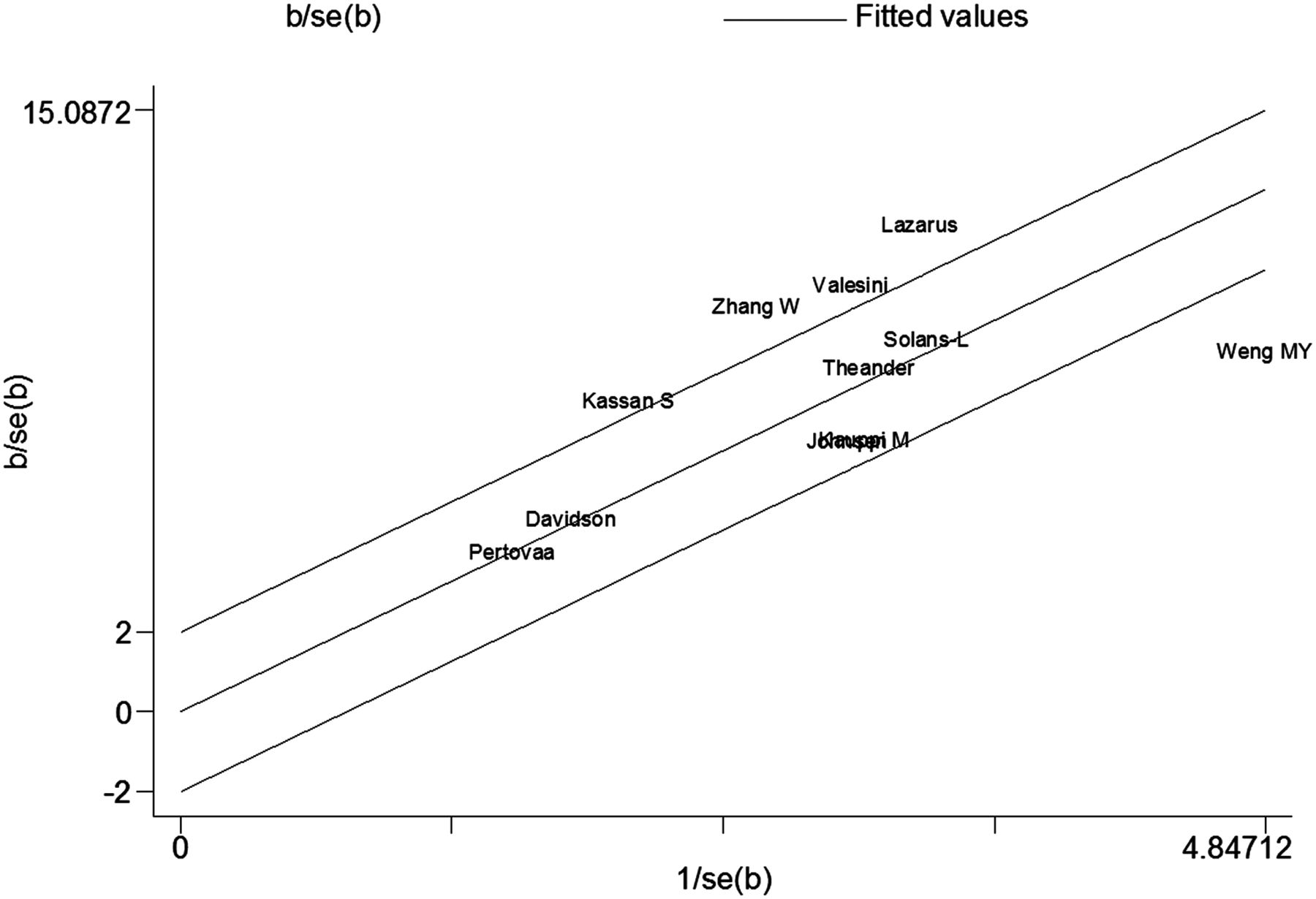
Owing to significant heterogeneity, we used the random effect model. The result indicated that pSS was associated with a 53% increased risk for overall malignancy (table 2). The Galbraith plot showed that three studies might be major sources of heterogeneity (figure 2), two of which were conducted in Asia18 ,22 and one in Europe.16 Subgroup analysis showed that there was significant heterogeneity between the two studies in Asia but no heterogeneity in Europe (table 3). Only one study which gave a SIR of 2.23 (95% CI 1.25 to 3.67) was conducted in the USA.3 Furthermore, pSS was significantly associated with an increased risk of overall malignancy in Europe but not in Asia.
Pooled relative risks of various malignancies
Stratified analyses of pooled relative risks of overall malignancy and NHL in patients with primary Sjögren's syndrome (pSS)

Galbraith plots of association between pSS and risk of overall malignancy.
We also performed a subgroup analysis by diagnostic criteria for pSS. The results indicated that only patients with pSS diagnosed by other criteria had an increased risk of overall malignancy (pooled RR 1.38; 95% CI 1.12 to 1.63), but those diagnosed by preliminary European criteria and the criteria of the American-European Consensus Group (AECG) did not. Additionally, subgroup analysis on study design produced large and moderate heterogeneity for hospital-based studies and population-based studies, respectively. The pooled RR was larger in hospital-based studies (pooled RR 2.25; 95% CI 1.27 to 3.22) than in population-based studies (pooled RR 1.12; 95% CI 1.00 to 1.23). Subgroup analysis showed a significant association in studies in which the mean duration of follow-up was >6.9 years but not for those with a mean follow-up of ≤6.9 years. Furthermore, significant heterogeneity was found for studies with a mean follow-up of ≤6.9 years but not for those with a mean follow-up of >6.9 years. Of note, subgroup analysis by mean age could not produce a significant result because some studies did not report the mean age of patients with pSS at entry (table 3).
pSS and NHL risk
Eleven studies explored the association of pSS and NHL risk and all showed that pSS was significantly associated with an increased risk of NHL. The pooled RR was 13.76 (95% CI 8.53 to 18.99) for NHL in a random effect model for patients with pSS compared with the general population. The possible major source of heterogeneity could not be found by the Galbraith plot because too many of the studies were outliers (figure 3). Subgroup analyses by region, diagnostic criteria for pSS, study design, mean age and mean duration of follow-up showed that patients with pSS had a significantly increased risk of NHL in various subgroups. Subgroup analysis showed significant heterogeneity among studies in Asia, population-based studies, studies on patients with pSS diagnosed by AECG criteria, with mean age ≤54 years and with shorter mean duration of follow-up (≤7.6 years) (tables 2 and 3).
{kind=link}
{kind=link}
{kind=link}
Galbraith plots of association between pSS and NHL risk.
pSS and other malignancy risks
The pooled RRs for other malignancies are summarised in table 2. The results showed that pSS was significantly associated with an increased risk of thyroid cancer (pooled RR 2.58; 95% CI 1.14 to 4.03) but not with other malignancy risks.
Sensitivity analysis and publication bias
No significant change in pooled RRs was found by sequential omission of individual studies, indicating that our results are stable and reliable.
Since funnel plots may be of no use in meta-analyses containing fewer than five studies,23 funnel plots and Egger tests were used to evaluate publication bias only for meta-analyses of pooling five or more individual studies. There was no obvious funnel plot asymmetry. All the p values of the Egger tests were >0.05, suggesting that publication bias was not evident in various meta-analyses (see online supplements 1–3).
Discussion
To our knowledge, this is the first meta-analysis to assess pSS and malignancy risks. We found that pSS is significantly associated with increased risks of overall malignancy, NHL and thyroid cancer.
Some studies examined the association between pSS and overall malignancy risk but no consistent conclusion was drawn.3 ,11 ,13 ,14 ,16–18 ,22 The present meta-analysis with more strong evidence confirmed that pSS is closely associated with an increased overall risk of malignancy. Patients with pSS may have an increased risk of overall malignancy of about 53%. However, this association seemed to be influenced by different diagnostic criteria for pSS. Patients with pSS diagnosed by preliminary European criteria and AECG criteria did not show a significant association. Therefore, when exploring the association between pSS and overall malignancy risk, the diagnostic criteria must be considered. Admittedly, the number of studies included in our various subgroup analyses was too small to draw firm conclusions and the association remains to be further investigated in patients with pSS by various diagnostic criteria. In addition, this significant association must be confirmed in both population-based and hospital-based studies. The RR from hospital-based studies is far higher than that from population-based studies. The reason may be that hospitalised patients with pSS have more severe disease, which suggests that more severe pSS is more likely to develop into malignancy. Subgroup analysis by region showed that the association could only be confirmed in European populations. However, a larger number of studies are needed to investigate the association in regions other than Europe. In addition, our subgroup analyses indicated that the association is also influenced by follow-up duration. If the mean duration of follow-up is not long enough (≤6.9 years), pSS may not show an association with the risk of overall malignancy. This may be because of the possibility of overlooking cases of pSS-associated malignancy that developed later in the disease process.
Several studies have shown a significantly increased risk of NHL in patients with pSS, particularly in women and in mixed sex groups of patients. Our meta-analysis confirmed this result with a more precise estimate. Similar results were found in various subgroup analyses. However, there are three noteworthy points to address. First, the number of studies in regions other than Europe is too small so further studies are needed in other regions. Second, the RR from hospital-based studies is much higher than from population-based studies, suggesting that the severity of pSS is significantly associated with an increased risk of NHL. Third, only one study examined the risk of NHL in male patients with pSS and found that pSS is not associated with NHL risk.22 It is therefore essential to investigate the association in men with pSS, although this is difficult due to the large predominance of women in pSS.
The present meta-analysis of five studies without between-study heterogeneity confirmed that pSS has no association with the risk of myeloma, which at least partly suggests that the aetiology between NHL and myeloma may be different. In addition, we carried out meta-analyses on the association of pSS with risks of several solid tumours and our results suggested that pSS is significantly associated with an increased risk of thyroid cancer but not with other solid tumours. However, we have to acknowledge that the number of studies on the association between pSS and the risk of solid tumours is too small to draw firm conclusions and more studies are needed.
The fact that some studies could have mixed populations of primary and secondary SS must also be addressed and may profoundly influence the final results. Among our included studies, only one on the risk of NHL and two on the risk of overall malignancy may have had mixed populations of patients. Sensitivity analysis by omitting these studies confirmed that they had no impact on the results (data not shown). For studies on other cancer risks, sensitivity analysis could not be carried out due to the small number of studies (only two or three).
Some limitations must be addressed. First, some studies that failed to provide data from which SIR could be calculated were not included in the meta-analysis. The exclusion of such studies may reduce the power of our analysis but is unlikely to bias our results. Second, several variables such as body mass index, smoking, alcohol consumption and immunosuppressive therapy cannot be excluded because of an inherent flaw in these included studies which might bias the results. Third, as described in a previous study, we were unlikely to completely exclude potential publication bias even though no significant publication bias was found by funnel plot analysis in this study. This is because small studies with null results tend not to be published.24 Fourth, some information such as age and duration of follow-up was not available from some studies so subgroup meta-analyses could only be conducted based on mean values, which may have had an impact on the estimated accuracy. Finally, data regarding pSS and the risk of solid malignancies were extremely sparse, limiting our ability to draw firm conclusions.
In summary, this meta-analysis shows that pSS is significantly associated with the increased overall risk of malignancy, especially NHL. However, it remains undetermined whether the association between overall malignancy and pSS is due to excess occurrence of NHL. Only one study investigated the association between pSS and the risk of malignancy other than NHL and did not find a significant association (SIR 1.53, 95% CI 0.89 to 2.63).16 Two studies examined the association of pSS with the risk of non-haematological tumours rather than non-NHL tumours; one found a positive result (SIR 2.12, 95% CI 1.27 to 3.31)18 but the other did not (SIR 1.1, 95% CI 0.8 to 1.5).13 We therefore cannot conduct a meta-analysis to evaluate whether the increased risk of overall malignancy with pSS is due to the presence of NHL and further studies are required. A significant association might also exist between pSS and the risk of thyroid cancer, but this needs to be confirmed by further studies.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figures
Footnotes
Handling editor Tore K Kvien
YL, ZY and BQ contributed equally.
-
Contributors ZY initiated the study design and wrote the manuscript. YL performed the analysis. BQ and RZ checked it. All authors saw and approved the final manuscript.
-
Funding This study was supported by two grants from the China National Natural Science Foundation Council (81001333 and 81102262) and Changzheng Hospital Funds for Young Scholar (2011CZQN06).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.