Article Text

Abstract
Objectives: To investigate the biodistribution and specific targeting for tumour necrosis factor (TNF) of a fully human, radiolabelled anti-TNF monoclonal antibody (anti-TNF mAb) in patients with active rheumatoid arthritis (RA). To assess whether this agent is suitable for visualisation of synovitis.
Methods: Ten patients with RA underwent whole body scintigraphy after administration of a tracer—subtherapeutic dose of 100 μg 99mTc human anti-TNF mAb. After two weeks, the procedure was repeated to assess the specificity of the radiolabelled antibody for TNF and its sensitivity for changes in inflammation. Therefore, a competition study was performed in five patients, who received excess unlabelled anti-TNF mAb before the tracer dose of 99mTc-anti-TNF. Another five patients received 120 mg methylprednisolone two days before the second scintigraphy.
Results: Radiolabelled anti-TNF mAb allowed clear visualisation of inflamed joints in patients with active RA with a high specificity. Concomitant administration of excess unlabelled anti-TNF reduced the joint uptake of 99mTc-anti-TNF mAb by a median of 25% as a percentage of the injected dose after 24 hours, whereas uptake in liver and spleen remained unchanged. Systemic corticosteroids reduced the disease activity, which was mirrored by a decreased joint uptake of the tracer. The anti-TNF mAb retained its high affinity for TNFα after labelling and was cleared from the circulation with an elimination half life of 48 hours. The procedure was well tolerated.
Conclusions: Radiolabelled human anti-TNF mAb allows visualisation of synovitis in patients with RA. Joint accumulation of this agent is partly due to specific TNF targeting and is highly predictive for inflammation.
- monoclonal antibodies
- rheumatoid arthritis
- scintigraphy
- tumour necrosis factor α
- DAS, disease activity score
- HPLC, high performance liquid chromatography
- HYNIC, hydrazinicotinamide
- ID, injected dose
- mAb, monoclonal antibody
- RA, rheumatoid arthritis
- TNFα, tumour necrosis factor α
Statistics from Altmetric.com
- DAS, disease activity score
- HPLC, high performance liquid chromatography
- HYNIC, hydrazinicotinamide
- ID, injected dose
- mAb, monoclonal antibody
- RA, rheumatoid arthritis
- TNFα, tumour necrosis factor α
Rheumatoid arthritis (RA) is characterised by a chronic and destructive polyarthritis. The role of proinflammatory cytokines such as tumour necrosis factor alpha (TNFα) in the pathogenesis of the disease is nowadays beyond question. Treatments aimed at neutralising TNF now used in clinical practice encompass chimeric monoclonal antibodies (mAbs) such as infliximab and TNF receptor-fusion proteins such as etanercept.
TNFα is produced as a soluble mediator and as a membrane bound molecule, and immunohistological studies in RA have shown that this cytokine and its receptors are present in inflamed synovial tissue.1,2 Nevertheless, there is a large inter- and intraindividual variability in the level of TNF expression,3,4 with the latter possibly having biological consequences. For instance, it is well known that a subset of patients with RA do not respond to TNF neutralisation. This might be due to lower levels of TNF expression or to a major involvement of other proinflammatory cytokines in the disease, or both. Accurate information on TNF expression in the joints might therefore be helpful to optimise and/or monitor the effect of TNF antagonism. Because RA is a polyarticular disease, immunohistological assessments cannot routinely be used to assess the degree and extent of TNF expression. Imaging studies aimed at targeting and visualising TNF in vivo would be an attractive alternative to other more invasive techniques.
Recent animal studies have shown that certain cytokines such as interleukin 1 and interleukin 8 specifically target their receptors in inflammatory foci and can be used for imaging studies.5,6 However, their use in humans is hampered by adverse events. In contrast, radiolabelled mAbs and cytokine antagonists can be used for specific targeting of membrane markers such as adhesion molecules7,8 or tumour antigens.9 Such agents can provide accurate information about the disease activity and localisation and some of them are nowadays used for imaging and for therapeutic purposes. To date, no imaging studies with TNF antagonists have been performed in humans.
Adalimumab (Humira, Abbott Laboratories) is a fully human, IgG1, anti-TNF mAb developed using phage display technologies. This compound has a high specificity and affinity for TNF (Kd 6×10−10 M) and specificity for TNF.10,11 Phase I to III studies have shown that repeated administration of this agent results in rapid and sustained clinical improvement and slows radiological progression in patients with RA.12–15
In this report we assess the scintigraphic imaging characteristics and the tissue biodistribution of systemically administered 99mTc-anti-TNF mAb in patients with active RA. Additionally, we assess whether imaging with this agent is sensitive to changes in disease activity and whether it targets TNF specifically.
PATIENTS AND METHODS
Patients
Enrolled patients had RA according to the American College of Rheumatology criteria,16 were aged 18 years or older, had active disease defined by a disease activity score (DAS17) >3.2, and had given informed consent. All patients received concomitant treatment with non-steroidal anti-inflammatory drugs and antirheumatic drugs at doses that were kept constant for at least four weeks before and during the study. Exclusion criteria were lactation or pregnancy, systemic or intra-articular corticosteroid administration within three months before the study, major surgery or infection in the past four weeks, history of tuberculosis, white cell counts <3.5×109/l, concomitant serious diseases, and previous treatment with TNF blockers or any other biological agent in the past.
Study protocol
Each patient underwent two scintigraphic sessions separated by an interval of two weeks. Clinical and laboratory assessments of disease activity were obtained immediately before, one day and two weeks after each scintigraphy. Just before imaging, patients received a single intravenous subtherapeutic dose of 100 μg (740 MBq) 99mTc labelled human anti-TNF mAb. The purpose of the first scintigraphy was to assess the biodistribution of anti-TNF in vivo. The purpose of the second scintigraphy was to assess (a) the specificity for TNF targeting by means of an excess anti-TNF mAb competition study and (b) the sensitivity to reflect decreased inflammation after administration of systemic corticosteroids. For the competition study, a subset of five patients received a therapeutic dose (10 mg/kg) of unlabelled human anti-TNF mAb immediately before the tracer dose of 100 μg 99mTc labelled anti-TNF. Another patient subset was treated with a single intramuscular dose of methylprednisolone 120 mg two days before the second scintigraphy. The study was approved by the institutional review board of the University Medical Centre, Nijmegen.
Imaging procedures
Whole body images and spot views of inflamed joints were obtained with a dual head gammacamera (MultiSPECT2, Siemens, Hoffmann Estates, IL) connected to a Scintiview image processor and ICON computer system at 5 minutes, 4 and 24 hours after injection. The scintigraphic images were collected in digital format (1024×256 and 256×256 matrix for whole body and spot views, respectively) and scored for joint uptake (0=no uptake, 1=uptake) without knowledge of the clinical scores. Analysis was performed by calculation of whole body clearance and ratios of uptake in regions of interest drawn over the positive joints and periarticular normal tissue and other organs showing uptake, normalised for the area of the region. Uptake data are expressed as a percentage of the injected dose (%ID).
Blood clearance
Radioactivity in blood samples, obtained at 1 minute, 1, 2, 4, and 24 hours after injection, was measured in the gammacounter and expressed as percentage of the injected dose per gram of blood (%ID/g) after correction for radioactive decay.
Radiolabelling and characterisation of the anti-TNF mAb
The human anti-TNF mAb was labelled using the indirect approach described by Abrams et al.18 Briefly, succinimyl-hydrazinicotinamide (S-HYNIC), a bifunctional chelator, was conjugated to the anti-TNF antibody at a 1:3 molar ratio in 0.1 M NaHCO3, pH 8.2 during 30 minutes at room temperature. Unconjugated HYNIC was removed by extensive dialysis against sterile acetate buffer, pH 5.0. Subsequently, 100 μg aliquots of mAb-HYNIC conjugated antibody were stored at −20°C until use. The anti-TNF mAb-HYNIC conjugate was radiolabelled with 99mTc just before each imaging session by mixing an aliquot of 100 μg conjugate with 10 μg SnSO4, 10 mg tricine, and 750 MBq (20 mCi) TcO4− and incubation for 15 minutes at room temperature. Labelling efficiency was determined by instant thin layer chromatography on silica gel strips. The stability of the radiolabelled antibody was tested by high performance liquid chromatography (HPLC; Phenomenex 2000 size exclusion column, 300×4 mm) and by transchelation assays,19 in which the 99mTc-anti-TNF mAb was incubated for four hours at 37°C in the presence of increasing concentrations of glutathione and cysteine. The choice of 99mTc was based on its ideal physical characteristics (140 keV γ emission, t½12 six hours) and on its wide use for antibody mediated imaging.9,21,21
RESULTS
99mTc-anti-TNF mAb allows visualisation of affected joints in patients with RA
Ten patients with active RA were enrolled in this study and all underwent a first imaging with a tracer dose of 100 μg 99mTc-anti-TNF mAb alone. Thereafter, patients were subdivided into two groups—the first examined in a competition study and the second in repeated scintigraphy after steroid administration. Table 1 shows that the patients’ characteristics in both groups were similar.
Characteristics of the patients studied. Data are given as mean (SD) unless indicated otherwise
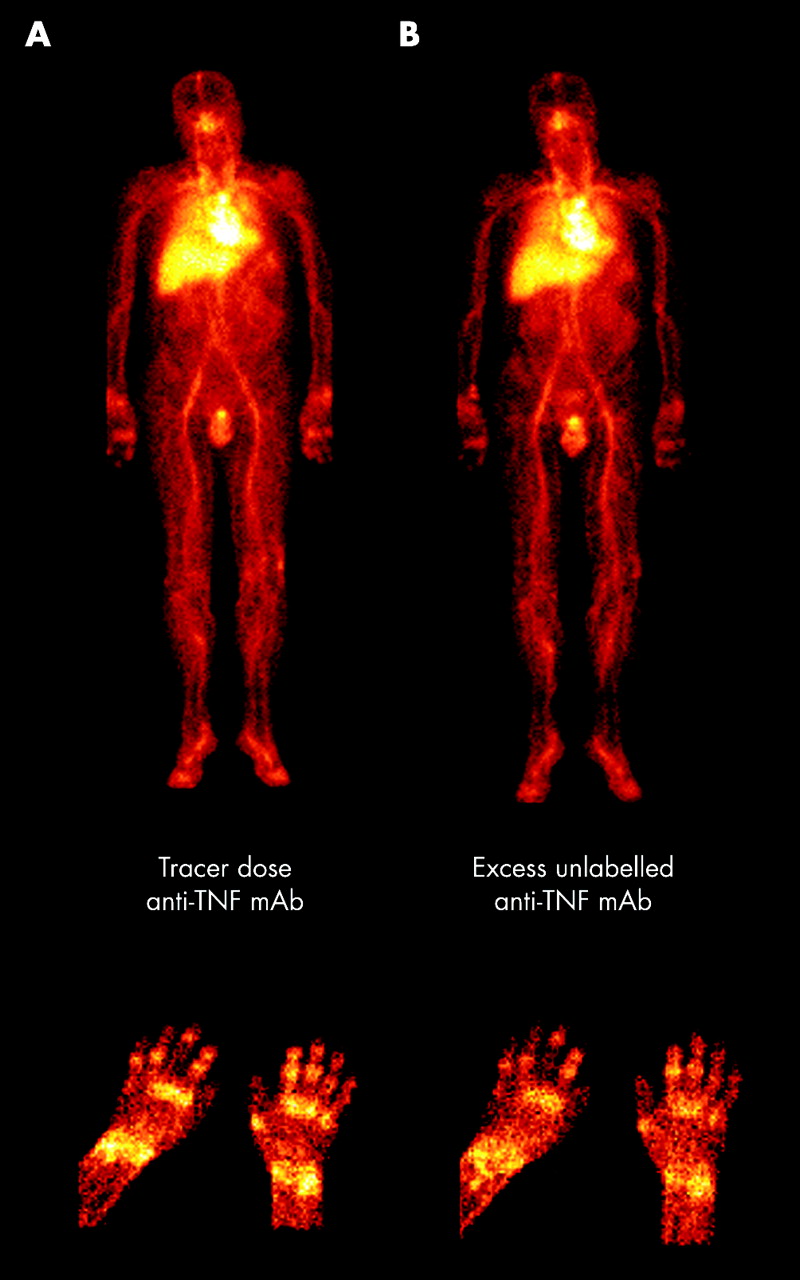
Figure 1 shows the biodistribution of 99mTc-anti-TNF mAb illustrated by the anterior whole body images. In all 10 patients 99mTc-anti-TNF mAb localised in inflamed joints within minutes after injection. Joints were clearly visualised at 4 and 24 hours after injection and the median percentage increase in uptake between these two times was 30%. The uptake of 99mTc-anti-TNF mAb in inflamed joints (fig 1, hand joints detail) was at least two- to threefold higher than in periarticular normal tissue and reached peak values of around fourfold. Uptake of radiolabelled anti-TNF mAb was also noticed in the liver and spleen (mean (SD) 13.8 (4.7) %ID and 2.1 (1.2) %ID, respectively). The 99mTc labelled anti-TNF mAb cleared from blood with a median elimination t½12α of 48 hours.
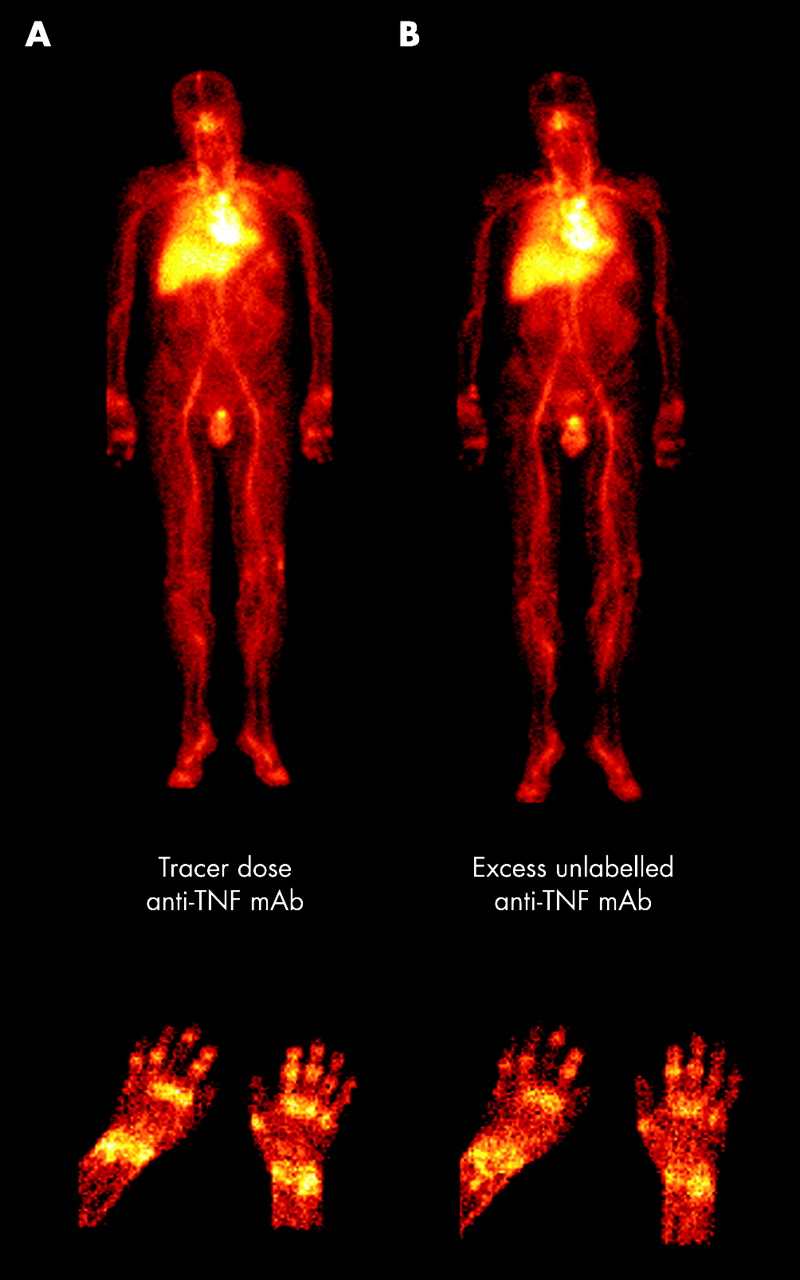
Scintigraphic images of the whole body and hands of a patient with active RA after injection of 99mTc human anti-TNF mAb. (A) The first imaging session. (B) Decreased uptake in joints after administration of an excess unlabelled anti-TNF mAb (hands detail), whereas the uptake in the reticuloendothelial organs remains unchanged (whole body).
No uptake of 99mTc-anti-TNF mAb was seen in clinically unaffected joints of any of the patients examined. Conversely, not all clinically affected joints showed 99mTc-anti-TNF mAb uptake and this was especially true for the small joints in the hands and feet. Systemic administration of 99mTc anti-TNF mAb was well tolerated and no adverse events occurred. As expected, the tracer subtherapeutic dose of 99mTc labelled anti-TNF mAb used in the first imaging sessions did not yield significant changes in disease activity parameters. This was reflected by similar DAS values at baseline and before the second scintigraphy in the anti-TNF group (fig 2).

{kind=link}
{kind=link}
Course of the DAS during the study. Patients with active RA underwent a first scintigraphy with a tracer dose of a fully human anti-TNF mAb radiolabelled with 99mTc. Two weeks thereafter, a subset of patients (n=5, rhomboids) received a therapeutic dose of the same antibody (grey arrow) before the second imaging session to assess the TNF targeting in the joints. Another patient subset (n=5, squares) was treated with systemic steroids two days before the second scintigraphy (white arrow).
TNF mediated uptake of anti-TNF mAb in RA
Two weeks after the first scintigraphic procedure a subset of five patients underwent a competition study to assess to what extent the uptake and retention of 99mTc labelled anti-TNF mAb in inflamed joints was mediated by specific binding to TNF. To this aim, an excess of unlabelled anti-TNF mAb (at a therapeutic dose of 10 mg/kg) was given immediately before the second injection of a tracer dose of 100 μg 99mTc-anti-TNF mAb.
As shown in fig 1B, the joint uptake of radiolabelled anti-TNF decreased after excess of unlabelled anti-TNF. Quantitative analysis of the uptake in positive joints showed a decrease by a median of 16% and 25% (expressed as %ID) at 4 and 24 hours after injection, respectively, whereas the pharmacokinetics and the uptake in liver and spleen did not change when the label was given with a saturating dose of anti-TNF (data not shown). This rapid decrease in joint uptake could not be explained by changes in disease activity or in pharmacokinetics: the DAS (fig 2) and the number of swollen joints (median 20 and 19 before and 1 day after the second scintigraphy, respectively) remained unchanged within this period and the elimination t½12α was similar in both imaging sessions.
Scintigraphy with 99mTc-anti-TNF mAb is sensitive to changes in disease activity
To assess whether imaging with 99mTc-anti-TNF mAb could detect clinically significant changes in disease activity, a single dose of systemic corticosteroids was given to another subset of five patients two days before the second scintigraphy. As expected in this group, a decrease in DAS (fig 2) and its individual components was seen at the time of the second scintigraphy. This was also reflected by a lower uptake of 99mTc-anti-TNF mAb in inflamed joints (median decrease in %ID 25% and 8% at 4 and 24 hours after the second imaging respectively). The uptake in liver and spleen remained unchanged after corticosteroid administration.
Comparison of disease activity parameters seen two weeks after the second scintigraphy with those at study baseline in the whole group of 10 patients showed significant decreases in swollen joint counts (p=0.002), DAS, and erythrocyte sedimentation rate (p<0.02). Although the samples were too small for statistical comparisons, the clinical response to a single therapeutic dose of anti-TNF mAb and to systemic steroids was roughly similar at study termination (fig 2). The efficacy of the procedures, assessed by the patients on a visual analogue scale, was also similar (median of 67 and 64 for the anti-TNF and steroid group, respectively).
Radiolabelling and characterisation of the 99mTc human anti-TNF mAb
The radiochemical purity of each batch of 99mTc-labelled anti-TNF mAb, determined by thin layer chromatography, was always higher than 95%. The radiolabelled antibody was highly stable in serum. HPLC analysis showed only a minimal release (<3%) of the radiolabel after 24 hours’ incubation at 37°C. In the transchelation assay the 99mTc label remained associated with the anti-TNF mAb and a 10 000-fold molar excess of glutathione was needed to detect some evidence of 99mTc release.
DISCUSSION
In this study we show that radioimmunoscintigraphy with a 99mTc labelled, human anti-TNF mAb is feasible, can be used to image affected joints in patients with active RA, and is highly predictive for inflammation. Additionally, this procedure can detect clinical relevant changes in disease activity as reflected by the DAS.
Such results were not totally unexpected because adalimumab, the anti-TNF antibody used in this study, is an IgG1 molecule. Non-specific IgG labelled with the radioisotope 99mTc has been used now for years to image inflammation.20,21 The localisation of the latter to inflammatory foci is mainly due to non-specific mechanisms such as increased vascular permeability.21,22 None the less, the selectivity of IgG and other radiopharmaceutical agents can be increased by targeting them at certain molecules.23 The choice to target TNF in arthritis is attractive because the safety and efficacy of the human antibody used in our study and of other TNF blocking agents is now widely accepted.
In this study we investigated whether the localisation of 99mTc labelled anti-TNF mAb in inflammatory foci might be due to interaction with TNF present in the target tissue. Our results show that the uptake and retention of this radiolabelled agent in arthritis is to a large extent due to targeting TNF in the joint. This is supported by the fact that the uptake of 99mTc labelled anti-TNF in inflamed joints, expressed as %ID, was reduced by 25% when excess unlabelled anti-TNF was coadministered, whereas the uptake in the reticuloendothelial organs, such as liver and spleen, and the pharmacokinetics remained unchanged. Furthermore, the imaging could detect changes in inflammation because the joint uptake decreased markedly after administration of systemic corticosteroids, reflecting a decrease in disease activity. We also show that imaging with 99mTc human anti-TNF mAb is highly predictive for inflammation because, in all patients studied, uptake of this agent occurred exclusively in inflamed joints. The reason why not all clinically affected joints showed uptake of radiolabelled anti-TNF remains speculative but might be explained by the absence of TNF because this cytokine is not always seen in inflamed synovial tissue.3,4,24
Taken together, our results show that anti-TNF mAb does target TNF in inflamed joints of patients with RA. It seems very likely that this is also the case in other inflammatory conditions. The use of this agent as radiopharmaceutical agent to monitor inflammation may therefore offer advantages over non-specific IgG, especially in diseases where TNF is involved, including RA, juvenile chronic arthritis, seronegative spondyloarthropathies, and Crohn’s disease.