Article Text

Abstract
Objective: To study the levels of procalcitonin (PCT) in various inflammatory states seen in an internal medicine department and to evaluate the possible discriminative role of PCT in differentiating bacterial infection from other inflammatory processes.
Methods: PCT, C reactive protein (CRP), and white blood cell count (WBC) were measured in patients admitted to the department for fever or biological inflammatory syndrome, or both. The serum of 173 consecutive patients was analysed according to the aetiological diagnosis. The patients were divided into two groups: group I (n=60) with documented bacterial or fungal infection; group II (n=113) with abacterial inflammatory disease.
Results: PCT levels were >0.5 ng/ml in 39/60 (65%) patients in group I. In group II, three patients with a viral infection had slightly increased PCT levels (0.7, 0.8, and 1.1 ng/ml) as did two others, one with crystal arthritis and the other with vasculitis (0.7 ng/ml in both cases). All other patients in group II had PCT levels <0.5 ng/ml. In this study a value of PCT >0.5 ng/ml was taken as the marker of bacterial infection (sensitivity 65%, specificity 96%). PCT values were more discriminative than WBC and CRP in distinguishing a bacterial infection from another inflammatory process.
Conclusion: PCT levels only rose significantly during bacterial infections. In this study PCT levels >1.2 ng/ml were always evidence of bacterial infection and the cue for starting antibiotic treatment.
- procalcitonin
- C reactive protein
- abacterial inflammatory processes
- CI, confidence interval
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- PCT, procalcitonin
- ROC, receiver operating characteristic
- TNFα, tumour necrosis factor α
- WBC, white blood cell count
Statistics from Altmetric.com
- CI, confidence interval
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- PCT, procalcitonin
- ROC, receiver operating characteristic
- TNFα, tumour necrosis factor α
- WBC, white blood cell count
Procalcitonin (PCT), the precursor of the hormone calcitonin, is produced under normal conditions in the C cells of the thyroid gland. In healthy subjects, PCT levels are <0.10 ng/ml. PCT determination was first performed by in 1993 Assicot et al in children to differentiate bacterial from viral meningitis.1 Since that date, PCT has become a marker of bacterial infection and there is a widening range of indications for its use.2,3 Determination of the PCT level is now routinely performed in intensive care and surgery units to provide rapid evidence of bacterial origin or a shock or a respiratory distress syndrome; to differentiate pancreatitis with infected necrosis more easily from non-complicated pancreatitis; and for early detection of infectious postoperative complications.4–6 However, little work has been done on the usefulness of PCT in diseases other than infectious states. Thus we carried out a study of PCT in various inflammatory states seen in an internal medicine department. This work aimed at evaluating the possible discriminative use of PCT in differentiating bacterial infection from other inflammatory processes.
SUBJECTS AND METHODS
Subjects
From October 1999 to December 2001 we conducted a prospective study at the internal medicine department of the teaching hospital of Clermont-Ferrand, France. PCT serum levels were measured within 24 hours of admission in patients admitted to hospital for fever >38° and/or for an inflammatory syndrome as defined by a rise in erythrocyte sedimentation rate (ESR) according to Miller’s formula (normal for age: female ESR = (age + 10)/2, male ESR= age/2) and/or by C reactive protein (CRP)>20 mg/l. PCT, white blood cell count (WBC), and CRP obtained on admission were analysed according to the final aetiological diagnosis of bacterial infection or inflammatory process of a different nature.
Patients who had received antibiotic treatment before admission were excluded.
Only documented infections were analysed. The diagnosis of bacterial or fungal infection was only established if a pathogen was isolated in various bacterial samples (blood cultures, sputum, pus, stool, or urine) or if serum samples were positive for Chlamydia pneumoniae, Coxiella burnettii, Brucella melitensis, and Legionella pneumoniae infections.
The diagnosis of viral infection was established in a patient with positive serum samples or positive polymerase chain reaction tests from cerebrospinal fluid.
Patients with suspected bacterial or viral infection but in whom no pathogen could be identified were excluded from the study. In the same way, in order to be in a position to explain the results of this study, patients with an inflammatory syndrome without a clear cut diagnosis were excluded.
Measurements
PCT was measured by an immunoluminometric assay (Lumitest-PCT, Brahms-Diagnostica, Berlin, Germany). The threshold of detection of PCT defined by our laboratory is 0.1 ng/ml. Values of PCT levels >0.5 ng/ml were considered as abnormal.
Statistical analysis
Statistical analysis was performed with SPSS 10.1 package.
The values of the three variables of inflammation are expressed as median and range. Because of non-normal distributions of the variables, we used the Mann-Whitney U test to compare the two diagnostic groups: bacterial infection and abacterial inflammation. The diagnostic value of PCT and other inflammatory variables for detecting bacterial infection was established by a receiver operating characteristic curve (ROC). Finally, a logistic regression was used to study the relation between the final diagnosis and the three biological variables.
RESULTS
One hundred and seventy three consecutive patients were included (98 women, 75 men; mean age 68 years).
On the basis of the final diagnosis, two different groups were established. Group I comprised 60 patients with documented bacterial (n=59) or fungal (n=1) infection and group II 113 patients with abacterial inflammation. Tables 1 and 2 show the different inflammatory processes and the corresponding median values of PCT, CRP, and WBC for groups I and II.
Biological variables of group I: bacterial or fungal infections
Biological variables of group II: abacterial inflammatory diseases
In group I, 65% of patients (39/60) with bacterial or fungal infection had PCT levels >0.5 ng/ml. Of these patients, three had autoimmune disease treated by immunosuppressive drugs (one vasculitis, one lupus, one rheumatoid arthritis), one was being treated with cyclosporin for cardiac transplant, and one other was receiving chlorambucil for lymphoid leukaemia. All five of these infected patients had PCT levels >0.5 ng/ml. Table 3 gives the PCT values according to the pathogen isolated.
PCT levels according to pathogen isolated
In group II, 96% of patients (108/113) with abacterial inflammatory disease had PCT levels ≤0.5 ng/ml. Five patients had false positive results. Three patients with viral infection—one with cytomegalovirus infection, one with Epstein-Barr virus, and one with Enterovirus meningitis—had slightly increased PCT (0.8, 1.1, and 0.7 ng/ml, respectively). One patient with crystal arthritis and the other with digestive vasculitis had PCT levels >0.5 ng/ml (0.7 ng/ml in both cases).
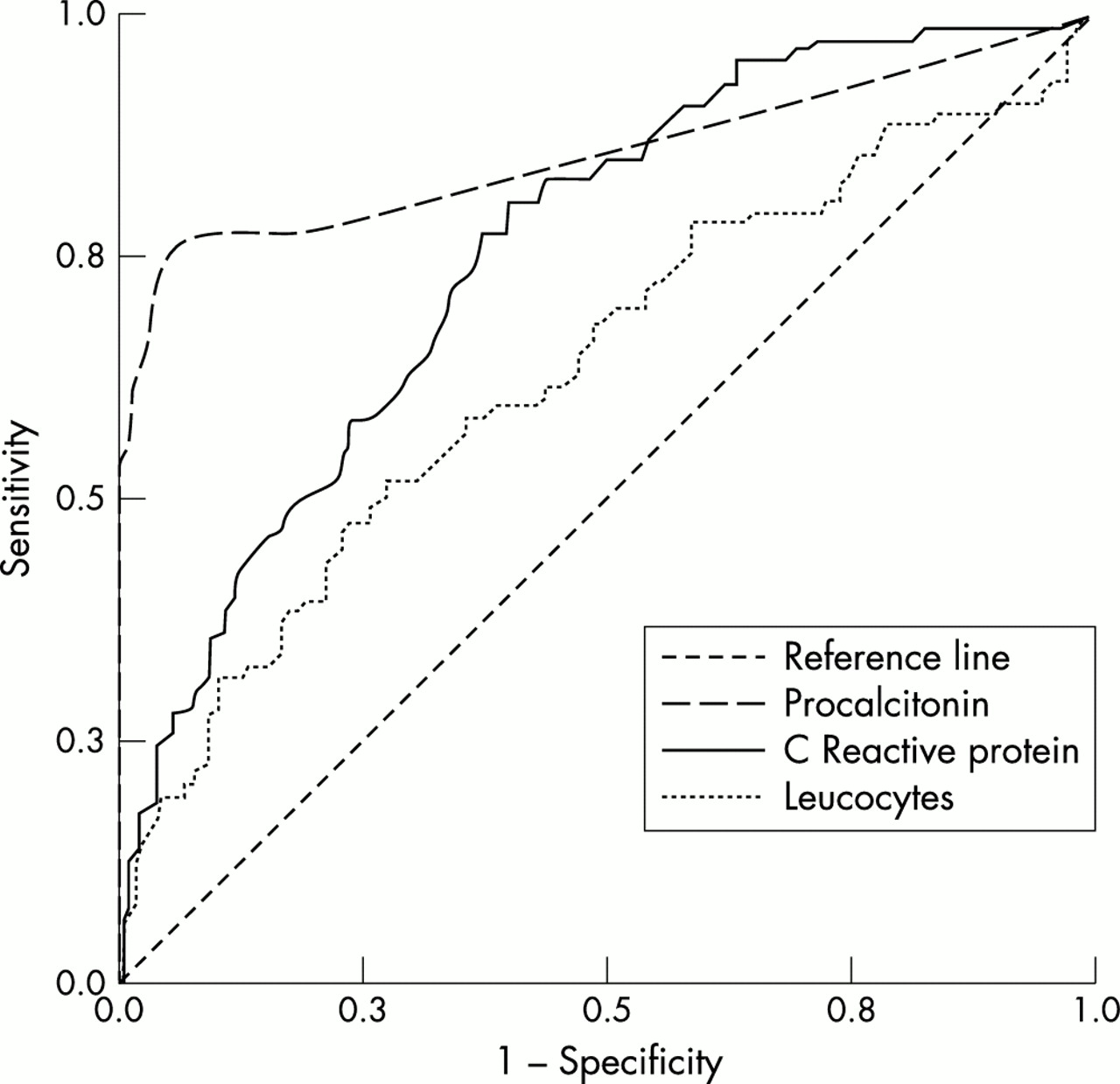
In this study, PCT levels >0.5 ng/ml were a marker of bacterial infection with a specificity of 96%, a sensitivity of 65%, a positive predictive value of 89%, and a negative predictive value of 84%. Area under the ROC curve for the prediction of bacterial infection was 0.84 (95% confidence interval (CI), 0.76 to 0.91; p=0.0001) for PCT, 0.62 (95% CI 0.53 to 0.71; p=0.011) for WBC, and 0.73 (95% CI 0.65 to 0.80; p=0.0001) for CRP (fig 1). On the ROC curve the PCT level that combined greatest sensitivity and comparatively good specificity was 0.35 ng/ml (specificity 88.5%, sensitivity 72%). Because of the distributions of inflammatory variables we used the Mann-Whitney U test to compare the variables in the two groups. Values of WBC, CRP, and PCT were significantly higher (p=0.011; p=0.0001; and p=0.0001, respectively) in group I (WBC: median 10.0×109/l, range (3.0–32.7)×109/l; CRP: median 137 mg/l, range 3–509; PCT: median 0.9 ng/ml, range 0.1–458 ) compared with group II (WBC: median 8.1×109/l, range (2.3–20.6)×109/l; CRP: median 71.5 mg/l, range 0.9–403; PCT: median 0.1, range 0.1–1.1). A logistic regression was performed to determine the relation between the three biological variables and the two diagnostic groups, with the group as the character to be explained and WBC, CRP, and PCT as the explanatory variables. In our series, 84% of the patients were correctly classified by the regression. The variable in the equation was PCT with a significance of 0.001 (WBC: p=0.250; CRP: p=0.487) (Hosmer-Lemeshow’s test: χ2=0.99; p=0.91).

{kind=link}
Prediction of bacterial infection ROC curves, with area under curve for procalcitonin=0.84, WBC=0.618, CRP=0.729.
DISCUSSION
It has been shown that PCT has a good specificity and a good positive predictive value for systemic bacterial infection. With a cut off level for PCT of >0.5 ng/ml for diagnosis of bacterial infection, only five patients in our series (three with viral infections, one with crystal arthritis, and one with vasculitis) had false positive results. In previously published reports, the cut off level beyond which a bacterial infection is considered as definite ranges between 1 and 2 ng/ml, except in patients receiving OKT3, in whom PCT levels are increased without infection.3,7,8 Hence, in our series, for PCT levels >1.2 ng/ml, there were no false positive results. It is the level we routinely use as a reference value once biological investigations have been done and before empirical antibiotic treatment is started.
The specificity (96%) and the sensitivity (65%) of PCT in our series, for PCT levels >0.5 ng/ml, are comparable with those reported elsewhere.3,8 False negative results may occur. PCT is not raised in localised bacterial infections. The nature of the causative infectious agent also influences the rise in PCT levels. In a human experimental study, PCT levels were raised after injection of bacterial endotoxin. The rise in PCT was preceded by raised cytokine tumour necrosis factor α (TNFα), suggesting a role of TNFα in PCT secretion. Furthermore, it is during infections associated with marked TNFα release, such as Gram-negative infections and malaria, that the highest PCT levels are seen.9,10 In malaria, PCT levels may rise to 1000 times the normal value. Infections in which other inflammatory pathways are activated do not increase PCT levels. This observation has been well documented in tuberculosis, as in our four patients with proven evidence of the disease.11 In addition, PCT levels do not increase in Lyme disease or mycobacterial infections.3,12 In our series, two patients who had endocarditis, one due to Streptococcus anginosus and the other to Staphylococcus aureus, had normal PCT levels. Lastly, the short half life (22 hours) of the PCT may explain why PCT levels recorded shortly after the beginning of antibiotic treatment are sometimes normal.2
Except in antineutrophil cytoplasmic antibody associated vasculitis and connective tissue disease, PCT levels have not been studied during abacterial inflammatory processes.13,14 In the patients studied, PCT levels, unlike those of CRP, stayed normal or increased only slightly, thereby making it possible to differentiate between a flare of the inflammatory disease and systemic bacterial infection. In Wegener’s granulomatosis, a moderate increase in PCT levels was seen in the very active forms.15 Hence, it is recommended that PCT levels >1 ng/ml should be used to distinguish between a flare vasculitis and bacterial infection.16 None of our five patients with flare Wegener’s granulomatosis had an increase in PCT levels. There is little published information on PCT levels in other autoimmune diseases and inflammatory processes. Because of the additional cost, the usefulness of measuring PCT levels in proven cases of bacterial infection is a matter of debate. However, PCT can be useful to differentiate between bacterial infection and other inflammatory processes in patients who have a rise in classic inflammatory markers without isolation of an infectious agent in the biological samples. Giant cell arteritis presenting as isolated fever, crystal arthritis, and Still’s disease are disorders that are sometimes difficult to distinguish from true bacterial infection. In these three diseases, as seen in findings from our patients, there is a marked inflammatory syndrome (median values of CRP and WBC respectively 84.6 mg/l and 9.1×109/l, 234 mg/l and 10.1×109/l, 229.5 mg/l and 12.2×109/l). These inflammatory variables were similar to those of the patients with septicaemia or skin infection or pneumonia (table 1). In contrast, PCT levels were greatly different between the two groups. Median values of PCT were always <0.5 ng/ml in patients with abacterial inflammatory disease, whereas values of PCT were 6.5 ng/ml in septicaemia, 4.2 ng/ml in skin infection, and 1 ng/ml in pneumonia. Likewise, median values of CRP and WBC were high in the neoplasm group and in patients with pulmonary embolism, whereas the median value of PCT was <0.5 ng/ml. It seems, therefore, that normal PCT levels during severe inflammatory disease argue in favour of an abacterial cause of the disorder. In contrast, during inflammatory processes in which CRP levels and WBC are raised less (as in our patients with vasculitis or ulcerative colitis, who had inflammatory variables comparable with those of patients with endocarditis), normal PCT levels are not a sufficient cause for ruling out localised bacterial infection or Gram positive infection.
PCT levels were always raised in the five patients with bacterial infection receiving immunosuppressive treatment. One patient had septicaemia, one had skin infection, one had diarrhoea and two others had pneumonia. All five patients had fever and raised inflammatory variables, which were evocative of an inflammatory disease flare and infectious complication. We started antibiotic treatment in all cases before the results of bacterial studies establishing the bacterial or fungal origin of the fever were obtained. PCT can also help in detecting bacterial infection during febrile or inflammatory periods in patients with previous inflammatory disease even when they are receiving immunosuppressive treatment. This finding is unsurprising because increased PCT levels have been found in patients with neutropenic fever and bacterial infection.17 Although the site of procalcitonin production during sepsis is uncertain, it does not seem to be in the leucocytes.
PCT levels only rose significantly during systemic bacterial or fungal infection. In patients with fever or inflammatory syndrome who have PCT levels >1.2 ng/ml, we consider that bacterial infection should be sought and antibiotic treatment started even before the results of the bacteriological investigations are obtained. This approach is even more strongly recommended in patients with inflammatory disease given immunosuppressive treatment. In contrast, once tuberculosis and mycobacterial infection have been ruled out, normal PCT levels do not argue in favour of bacterial infection.
Acknowledgments
We thank Jeffrey Watts for help with the English version of the manuscript.