Article Text

Abstract
Background Immunogenicity of aTNFs is one of the mechanisms behind treatment failure.
Objective To assess the effect of anti-drug antibodies (ADA) on drug response to infliximab, adalimumab and etanercept, and the effect of immunosuppression on ADA detection, in patients with Rheumatoid Arthritis, Spondyloarthritis, Psoriasis and Inflammatory Bowel Diseases.
Data sources PubMed, EMBASE, Cochrane databases, article reference lists (through August 19 2012).
Study selection Out of 2082 studies, 17 were used in the meta-analysis (1RCT; 16 observational studies).
Data extraction Two reviewers extracted data. Risk ratios (RR), 95% CI, using random-effect models, sensitivity analysis, meta-regressions and Egger's test were calculated.
Data synthesis Of 865 patients, ADA against infliximab or adalimumab reduced drug response rate by 68% (RR=0.68, 95% CI=0.12 to 0.36), an effect attenuated by concomitant methotrexate (MTX): <74% MTX+: RR=0.23, 95% CI=0.15 to 0.36; ≥74% MTX+: RR=0.32, 95% CI=0.22 to 0.48. Anti-etanercept antibodies were not detected. Of 936 patients, concomitant MTX or azathioprine/mercaptopurine reduced ADA frequency by 47% (RR=0.53, 95% CI=0.42 to 0.67), particularly when ADA were assessed by RIA (RR=0.36, 95% CI=0.23 to 0.55) compared with ELISA (RR=0.63, 95% CI=0.53 to 0.74).
Conclusions ADA reduces drug response, an effect that can be attenuated by concomitant immunosuppression, which reduces ADA frequency. Drug immunogenicity should be considered for the management of patients receiving biological therapies.
- Autoimmune Diseases
- Anti-TNF
- Methotrexate
Statistics from Altmetric.com
Introduction
Anti-Tumor Necrosis Factor (aTNF) biological therapies, such as infliximab, adalimumab and etanercept, are effective in treating Rheumatoid Arthritis (RA), Spondyloarthritis (SpA), Psoriasis (Ps) and Inflammatory Bowel Diseases (IBD), such as Crohn's Disease and Ulcerative Colitis. Some patients maintain active disease and others show loss of efficacy after continued treatment.1 Recent studies have highlighted drug immunogenicity as a mechanism behind treatment failure.2–4
Immunogenicity is the ability that biotechnology-derived therapeutic proteins have in generating antibodies against themselves, since they contain unique sequences that can elicit an immune response.5
The European Medicines Agency and Food & Drug Administration define the assessment of immunogenicity as mandatory for the approval of biopharmaceuticals; however, clinical trials may not reflect true immunogenicity induced by long-term treatment.
Quantification of such antibodies is challenging and undertaken by different assays6–10; assays have been optimised with improved sensitivity and specificity.11–15 New evidence reveals a significant impact of immunogenicity on treatment response to biologics.2
A systematic review (SR) and meta-analysis (MA) were undertaken to evaluate the impact of anti-drug antibodies (ADA) on therapeutic response and the effect of immunosuppression (IS) on ADA detection.
Methods
We followed the PRISMA guidelines for reporting SRs and MAs and Meta-analysis Of Observational Studies in Epidemiology recommendations for observational studies.16 ,17
Eligibility criteria
To be included in this review, studies had to meet the following predefined eligibility criteria, defined according to the ‘PICOS’ strategy.17 The rationale for these criteria is also provided—table 1.
Eligibility criteria for studies included in the systematic review (SR)
Data sources
A comprehensive search strategy was designed to retrieve relevant clinical data from published literature. The following databases were examined up to 19 August 2012: PubMed, EMBASE and Cochrane Library. Article reference lists were also scanned. The following search terms were used: ((‘Arthritis, Rheumatoid’) OR (‘Spondylitis, Ankylosing’(Mesh)) OR (‘Arthritis, Psoriatic’(Mesh)) OR (‘Psoriasis’(Mesh)) OR (‘Colitis, Ulcerative’(Mesh)) OR (‘Crohn Disease’(Mesh))) AND ‘Treatment Outcome’(Mesh) AND ((‘TNFR-Fc fusion protein’(Substance Name)) OR (‘infliximab’(Substance Name)) OR (‘Adalimumab’(Substance Name))).
Study selection
Two independent authors selected studies and extracted data. Disagreements were resolved by discussion between the two reviewers. To ascertain the validity of eligible studies and to minimise the risk of bias, two blinded reviewers determined the adequacy of study characteristics. We decided to use more broad inclusion criteria and then to perform meta-regressions, subgroup analyses and sensitivity analysis, rather than using highly restrictive study quality assessment scores.16
Data extraction
The following information was extracted from each study: (1) population demographic characteristics: age, gender; (2) clinical data: diagnostic criteria and disease activity; (3) treatment: aTNF, duration, dose, schedule, route of administration, immunosuppressors; (4) exposure and outcome: therapeutic response, serum trough ADA, time of assessment, assay; (5) publication: study design, follow-up period, author, year.
Statistical analysis
Data were analysed by calculating risk ratios (RR) for each study and performing forest plots; uncertainty was expressed by 95% CI. Assuming clinical and methodological heterogeneity in the available body of evidence, random-effects models, according to the Laird method, were used to cluster the results. Heterogeneity of study results was examined by calculating the χ2 test for heterogeneity (when the χ2 test had a p<0.1) and the I2 measure of inconsistency.18 Potential sources of heterogeneity were explored through analysis of the following predefined subgroups and confirmed through meta-regression: (1) primary diagnosis; (2) proportion of patients co-treated with IS: methotrexate (MTX) or azathioprine/6-mercaptopurine (AZA/MCP); (3) proportion of patients who underwent aTNF dose escalation; (4) proportion of patients who started with higher initial doses of aTNF; (5) scheduled treatment regimens; (6) assay for ADA detection; (7) population characteristics and (8) study characteristics. Publication bias was analysed through the Egger's plot and test.
STATA V.SE 12 was used.
Results
Figure 1 shows the flow of studies through the SR process. Search of literature databases yielded 2082 references. Seventeen eligible studies were evaluated quantitatively, through MA. Five additional studies were exclusively qualitatively assessed because of significant missing data, but considered important evidence.

Flow of studies through the systematic review (SR) process. Access the article online to view this figure in colour.
To address the impact of ADA on drug response, 865 patients (540 RA, 132 SpA, 58 Ps, 130 IBD) from 12 observational prospective cohort studies were analysed;2 ,3 ,12 ,14 ,19–26 and five additional studies were described qualitatively27–31—table 2.
Study and baseline patient characteristics
Two publications used the same cohort of patients.2 ,20 We selected ‘Bartelds 2007’ for the MA based on it being the original study and showing less heterogeneity in the pooled analysis—online supplementary figures S1 and S2.
Two studies had multiple time points of assessment.14 ,24 The 12-month time point was selected for the MA, because of consistency with the included studies and less heterogeneity in the pooled analysis—online supplementary figures S3–S5.
Overall, detectable ADA reduced the drug response rate by 68% (RR=0.32, 95% CI=0.22 to 0.48)—figure 2. Significant between-study heterogeneity was observed (I2=45.5%, p=0.037). Seeking for potential sources of heterogeneity, we observed a trend to an increased effect size in studies where the proportion of patients co-treated with IS (%IS) was <67%—online supplementary figure S6. However, univariate meta-regression did not detect %IS as a significant effect modifier of the effect of ADA on response rates—table 3. A closer look at these subgroups showed that among studies where %IS <67%, detectable ADA was associated with a reduction in therapeutic response by 78% (RR=0.22, 95% CI=0.12 to 0.39) and in studies where %IS ≥67%, the effect size reduction of drug response was attenuated to 59% (RR=0.41, 95% CI=0.27 to 0.62)—online supplementary figure S6.
Meta-regression stratified by clinical characteristics to address the effect of ADA on drug response and the effect of IS on ADA detection
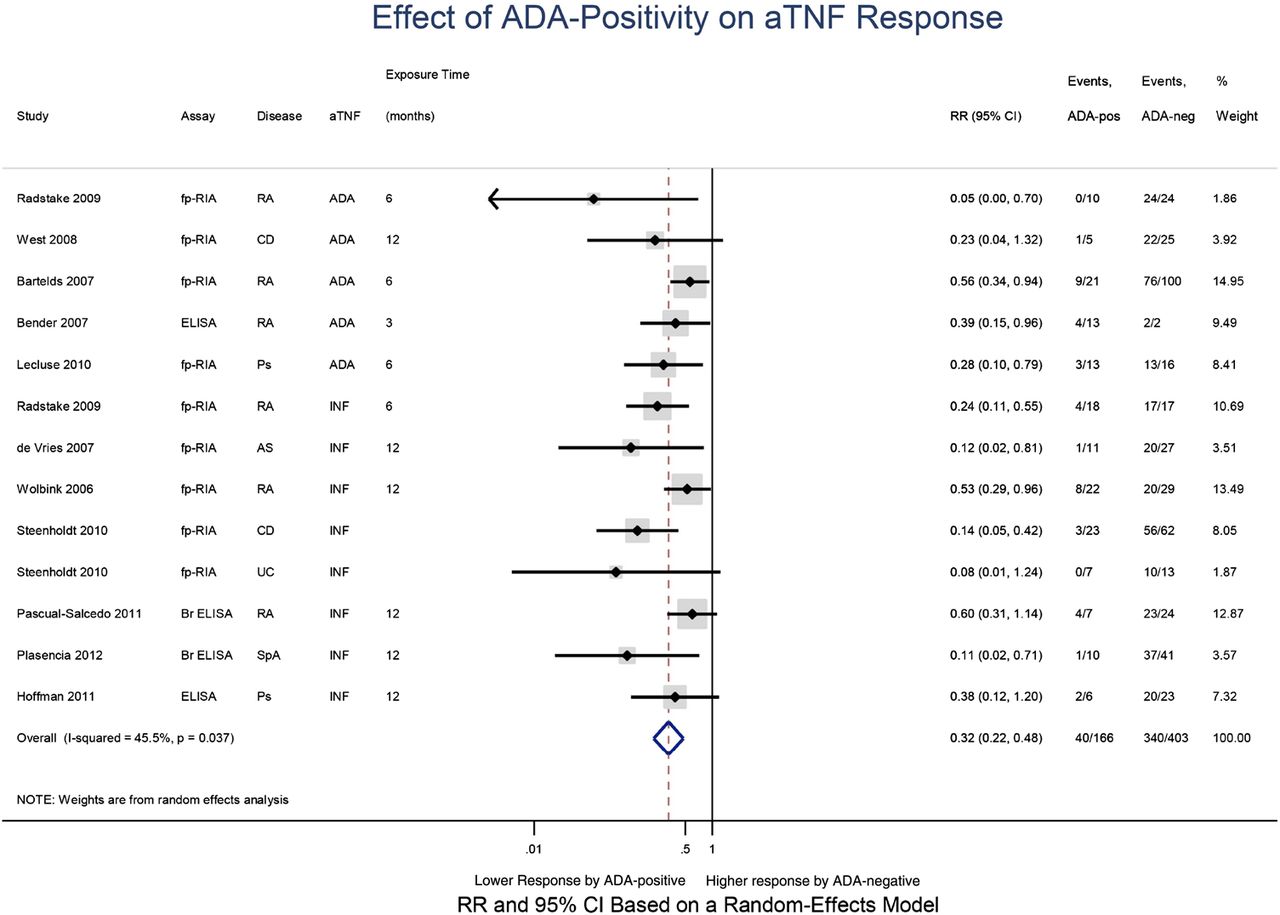
Effect of ADA positivity on aTNF response. ADA, anti-drug antibodies; AS, Ankylosing Spondylitis; Br ELISA, Bridging enzyme-linked immunosorbent assay; CD, Crohn's Disease; ELISA, enzyme-linked immunosorbent assay; fp-RIA, fluid-phase radioimmuno assay; INF, Infliximab; MTX, Methotrexate; Ps, Psoriasis; RA, Rheumatoid Arthritis; SpA, Spondyloarthritis; UC, Ulcerative Colitis. Access the article online to view this figure in colour.
Univariate meta-regression detects the proportion of patients co-treated with MTX (%MTX) as a significant effect modifier of ADA on drug response—table 3. In the subgroup analysis, we observed that in studies where %MTX<74%, the presence of ADA reduced therapeutic response by 77% (RR=0.23, 95% CI=0.15 to 0.36), while in studies where that proportion was ≥74%, the effect size reduction was attenuated to 68% (RR=0.32, 95% CI=0.22 to 0.48)—figure 3.
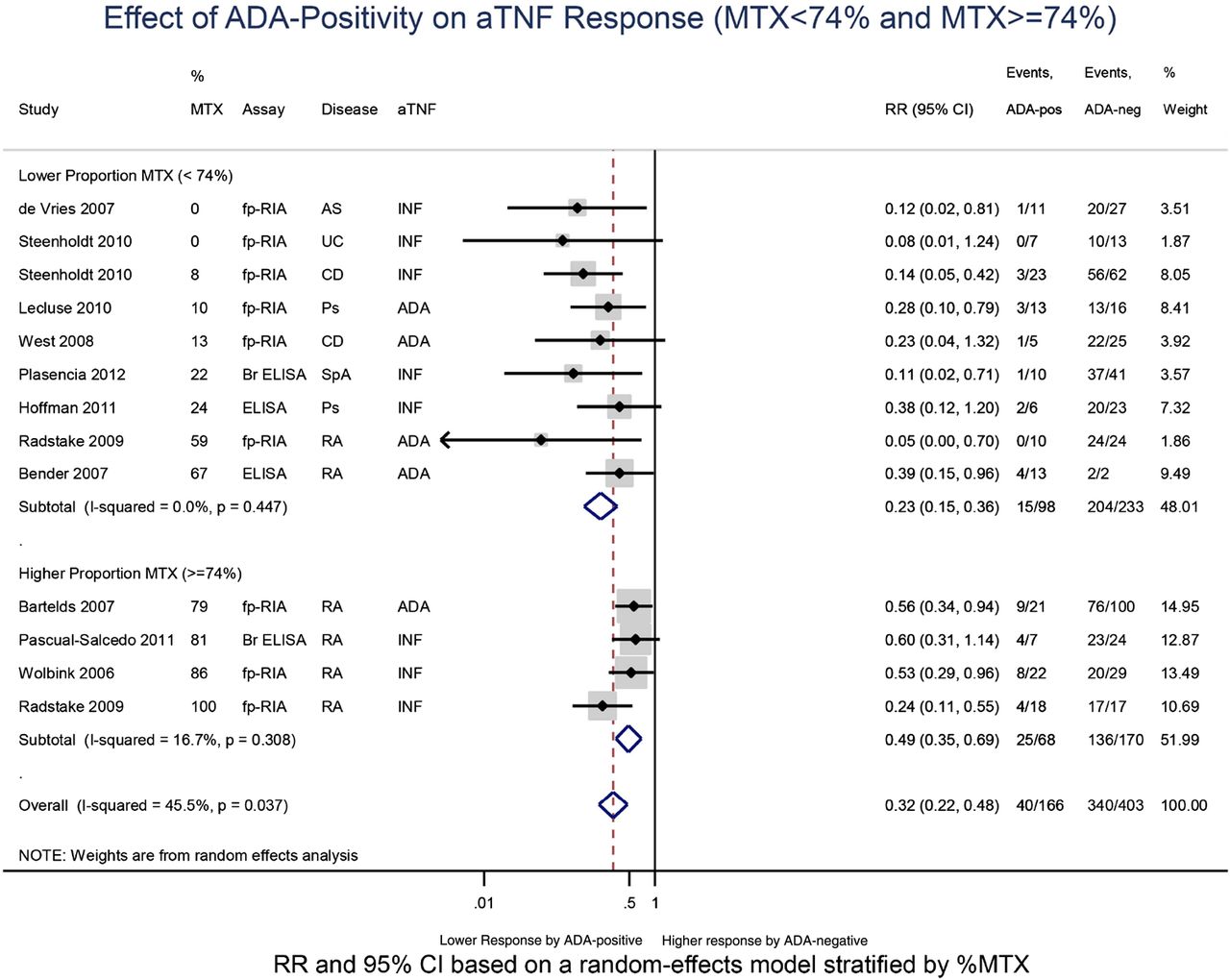
Effect of ADA positivity on aTNF response (MTX<74% and MTX ≥74%). ADA, anti-drug antibodies; AS, Ankylosing Spondylitis; BR ELISA, Bridging enzyme-linked immunosorbent assay; CD, Crohn's Disease; ELISA, enzyme-linked immunosorbent assay; fp-RIA, fluid-phase radioimmuno assay; INF, Infliximab; MTX, Methotrexate; Ps, Psoriasis; RA, Rheumatoid Arthritis; SpA, Spondyloarthritis; UC, Ulcerative Colitis. Access the article online to view this figure in colour.
Univariate meta-regression also showed primary diagnosis (RA vs others) and initial higher doses of biologicals to be significant effect modifiers of the effect of ADA on drug response—table 3. We verified a decreased effect size in studies evaluating RA patients and in studies where patients received initial lower doses of biologicals—online supplementary figures S7–S9). These studies are also those with lower proportion of patients receiving IS and MTX. Significant heterogeneity in the pooled analysis was abrogated by dividing the studies according to the proportion of patients receiving IS, and particularly MTX, independently of the disease or the doses of biologicals that were used.
The impact of ADA on drug response was not significantly affected by the proportion of patients who underwent aTNF dose escalation—table 3.
We could not test the effect size modification by scheduled treatment regimens or by the assay used for ADA detection since most studies used schedule regimens and radioimmuno assays (RIAs) to assess ADA.
The Egger's test provided evidence for no significant publication bias—online supplementary figure S10.
Studies with Etanercept were not analysed quantitatively because they did not fit the eligibility criteria and/or because no anti-etanercept antibodies were detected. Three studies are described qualitatively. Both described absence of anti-etanercept antibodies, by using Bridging ELISA and fluid-phase RIA, in a total of 332 RA patients,29 ,30 and 53 Ankylosing Spondylitis (AS) patients27 treated with 25 mg twice weekly or 50 mg weekly—table 1. The absence of anti-etanercept antibodies persisted 3 months after therapy withdrawal.27
We found two additional studies among Ps patients, which could not be included in the MA due to missing data. In a study enrolling 15 Ps patients receiving infliximab, those with detectable ADA had higher Psoriasis Area and Severity Index values than patients without such antibodies (Psoriasis Area and Severity Index (mean, sd)=10(4.9) vs 5.3(2.4); p=0.02).31 Similarly, another study, among 22 PsA patients, revealed that ADA-positive patients had a significantly worse disease activity score in 28 joints (DAS28) at 12 months of adalimumab therapy, when compared with patients without such antibodies (DAS28 (SEM)=5.05 (0.84) vs 2.58 (0.32); p=0.01).28
To address the influence of IS on the detection of ADA 936 patients (376 RA, 94 SpA, 29 Ps, 437 IBD) from 12 studies were analysed quantitatively2 ,4 ,20–25 32–35—table 2.
MTX (dose range: 7.5–25 mg/week) was the main immunosuppressor used in RA patients; AZA (2–2.5 mg/kg/day) or MCP (1–1.25 mg/kg/day) were the main immunosuppressors used in IBD patients.
ADA were assessed through slightly different fluid-phase RIAs20 ,22 ,25 ,34 and three different ELISA methods.4 ,21 ,22 ,24 ,32 ,33 ,35
Two of the included studies used the same cohort of patients.2 ,20 ,34 We selected ‘Bartelds 2007’ for the MA based on the fact that it was the original study and also the one that offered lower heterogeneity in the pooled analysis—online supplementary figures S11–S13.
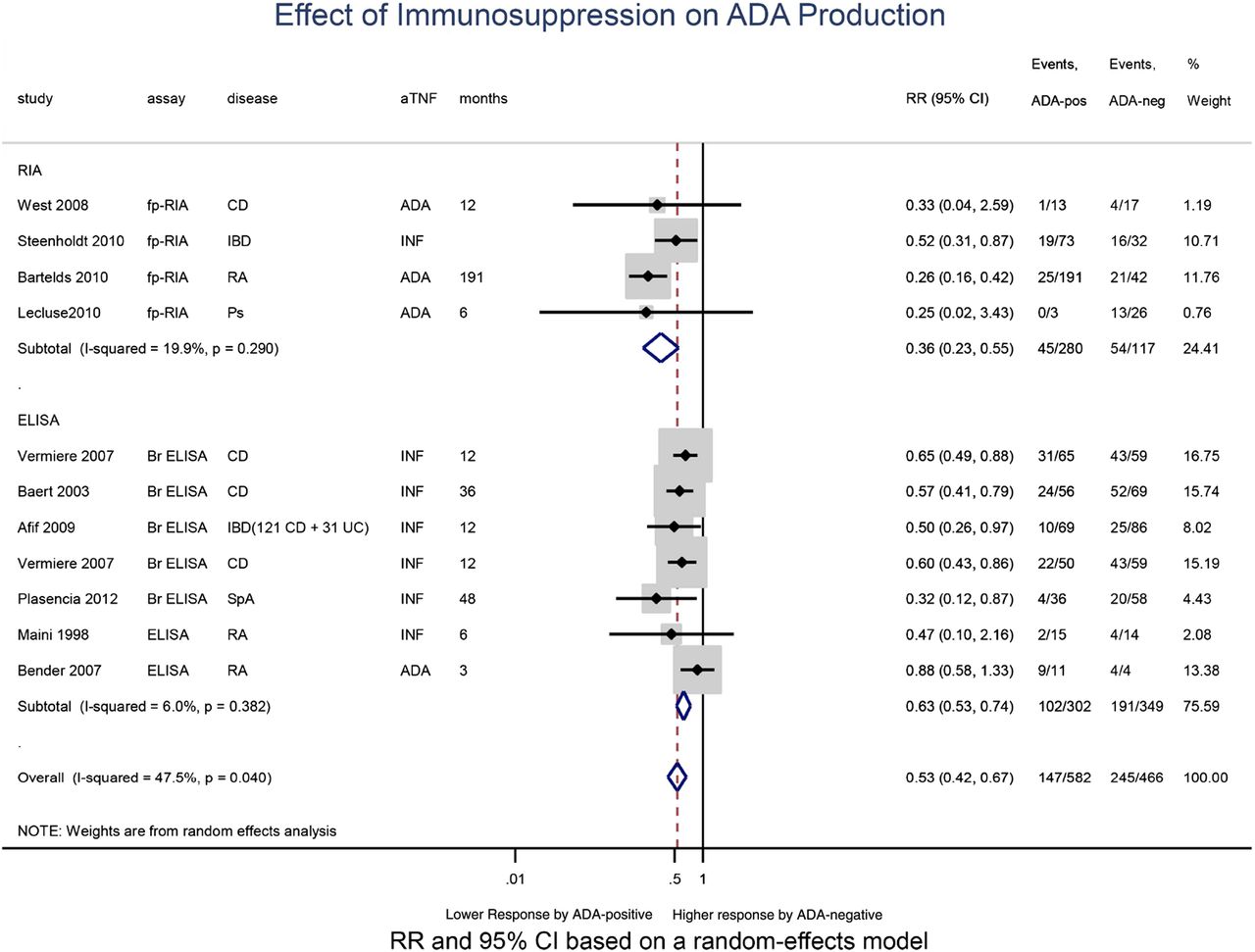
Immunosuppressors reduced the proportion of patients with detectable ADA by about 41% (RR=0.59, 95% CI=0.50 to 0.70) —online supplementary figure S14. Meta-regression confirmed the assay as a significant source of heterogeneity—table 3. Concomitant IS reduced detectable ADA by 64% (RR=0.36; 95% CI=0.23 to 0.55) when RIA was used to detect ADA, while when ELISA methods were used the effect size reduction of detectable ADA was attenuated to 37% (RR=0.63, 95% CI=0.42 to 0.67) —figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of immunosuppression on ADA production (by assay). ADA, anti-drug antibodies; Br ELISA, Bridging enzyme-linked immunosorbent assay; CD, Crohn's Disease; ELISA, Enzyme-linked immunosorbent assay; fp-RIA, Fluid-phase radioimmuno assay; IBD, Inflammatory Bowel Diseases; INF, Infliximab; Ps, Psoriasis; RA, Rheumatoid Arthritis; SpA, Spondyloarthritis; UC, Ulcerative Colitis. Access the article online to view this figure in colour.
It was not possible to evaluate potential differences in detectable ADA among MTX and AZA/MCP, due to limited data.
The Egger's test provided evidence of significant publication bias for the studies evaluating the effect of IS on ADA production—online supplementary figure S15. Positive results may be more likely to be published. However, the presence of small and heterogeneous studies may also underlie that result.
Discussion
Immunogenicity reduces therapeutic response to aTNFs, an effect that is attenuated by immunosuppressors. Detectable ADA decreases aTNF response by as much as 80%. This contrasts with descriptions in most randomized clinical trials (RCTs), considering immunogenicity as a minor problem.36–39 ADAs might reduce drug efficacy by competing with the endogenous ligand (neutralising antibodies) and/or by forming immune complexes, which accelerates the clearance of the drug from the circulation, decreasing its bioavailability. Anti-idiotypic antibodies, which include neutralising antibodies, represent the most significant part of the antibody response against infliximab and adalimumab.40–42 The detection of ADA is technically challenging and the assay may influence the results. The majority of studies in this paper used two independent but similar RIAs, with higher specificity than ELISAs.6 ,10 ,11 ,15 They are both fluid-phase RIAs, which avoid the artifacts induced by solid-phase adsorption of proteins and they both detect ADA against drug-F(ab′)2, not favouring the detection of low-avidity antibodies. RIA is less susceptible than ELISA to drug interference and is able to detect monovalent IgG4 ADA, which may represent a significant proportion of ADA.10 ,43 ELISAs have been the main method used in RCTs, perhaps explaining the contrasting descriptions in RCTs. We believe that the association remains underestimated: four of the included studies used ELISAs; the assays employed cannot detect ADA that is in complex with the drug, not even RIA and we included European League Against Rheumatism moderate response within the responder group.
Despite few published studies reporting anti-etanercept antibodies,44–47 all showed transient low titres, with no impact on drug response; this suggests the presence of ‘binding antibodies’ or false positive results, since ELISAs of low specificity were used. Etanercept is administered more often than other biologicals, possibly creating more drug interference in ADA detection. However, the absence of anti-etanercept antibodies has been confirmed months after therapy withdrawal.27 Etanercept also blocks lymphotoxin-α, which among other functions is important for germinal centre formation.48 The involvement of lymphotoxin-α on drug immunogenicity remains unknown. The absence of clinically significant immunogenicity attributable to etanercept is consistent with the higher drug survival that has been reported for etanercept in comparison with infliximab or adalimumab.49–51
Factors able to modulate the clinical impact of immunogenicity need to be identified. We verified that concomitant IS attenuated the impact of ADA on drug response, particularly MTX. The exact mechanism remains unknown. Concomitant MTX has been shown to be efficient in reducing immunogenicity in a dose-dependent manner, either by reducing the frequency of detectable ADA or by delaying its detection.24 ,52 ,53 The time point of ADA assessment is also important. In our MA the majority of included studies assessed ADA at 12 months, showing a lower ADA frequency in patients receiving concomitant IS. That reduction was more apparent when RIA was used compared with ELISA methods (64% reduction vs 34%), which may be explained by the increased specificity and less drug interference of RIAs over ELISAs.
These results are of high clinical interest, since they reveal a putative beneficial role of concomitant IS in diseases such as SpA, by modulating immunogenicity, increasing drug survival and treatment effectiveness. A recent study in AS patients failed to demonstrate the influence of MTX on infliximab pharmacokinetics.54 Infliximab is administered more frequently and at higher doses in AS, compared with RA, which may create drug interference and false-negative results if highly drug-sensitive assays are used to detect ADA. That study was conducted up to 18 weeks of infliximab treatment, which for some patients may be too early for full development of immunogenicity. RCTs, with larger follow-up times should be conducted to show the beneficial effect of IS/MTX in these patients.
We could not assess differences between MTX and AZA/MCP regarding their impact on ADA detection, due to the low number of studies using AZA/MCP and the fact that some studies in IBD also enrolled patients receiving MTX, who cannot be separated from the group receiving IS. However, univariate meta-regression detected %MTX as a significant source of heterogeneity, but not %IS (MTX+AZA/MCP). Subgroups based on %MTX resulted in homogeneous groups, whereas, the same did not happen for %IS subgroups. Further studies are warranted to verify whether this effect modifier is extended to other immunosuppressive agents and whether dose and scheduled regimens influence response by detectable ADA.
In some trials, initial higher doses of infliximab or adalimumab have revealed to be less immunogenic.35 ,55 It is not clear if that is a true effect or just an assay limitation of detecting ADA in the presence of high drug concentration. We could not draw any conclusions in our MA because the studies that used higher biological doses enrolled only patients with SpA, Ps and IBD, who also had lower proportion of patients co-treated with IS, confounding the results. Moreover, the limited number of studies and the clinical heterogeneity among them also prevent robust conclusions. Despite the high costs of biological therapies, it would be of great clinical interest to know if higher induction doses of biologicals would reduce immunogenicity, which could result in an improvement of its cost-effectiveness over the long-term.
Some reports show that dose escalation decreased ADA detection, improving drug response12 ,20 but others3 show that the procedure can indeed boost the immune response with serious consequences, such as infusion-related adverse events14 or severe thromboembolic phenomena.56 The absence of ADA might be explained by drug interference, but it is striking why some ADA-positive patients do not boost the ADA production. In our analysis, the proportion of patients who underwent dose escalation did not interfere with the impact of ADA on drug response. Very limited data are available and more studies are warranted to specifically address this question, since dose escalation is often adopted in clinical practice in case of inadequate response. We believe that increasing the dose may be risky since, so far, there is no way to identify which patients are at risk of boosting an anti-biological response after dose escalation.
Scheduled regimens have been revealed to be less immunogenic, by poorly defined mechanisms.4 ,57 ,58 The limited number of studies prevented us from drawing such conclusions in our analysis.
A limitation to our study is that patient population, assessment of antibodies and therapeutic response definitions are not standardised across studies, although we addressed those sources of heterogeneity in the pooled analysis. The power of meta-regression analysis has limitations by the relatively small number of studies and the imprecision of the measurement techniques. The results obtained are driven largely by findings in patients with RA. Although we excluded significant effect size modification by the disease itself, generalisations should be done cautiously.
This is the first SR and MA on aTNF immunogenicity. Our study strongly supports the notion that drug immunogenicity should be considered in clinical practice, during long-term use of therapeutic proteins. It is also an exploratory study, trying to identify factors able to influence the clinical impact of drug immunogenicity. It adds some evidence that unwanted immunogenicity may be modulated. Increasing evidence shows that monitoring immunogenicity will help us to better understand the clinical heterogeneity among patients, representing a very promising tool for an optimised and more personalised usage of biological therapies.
Acknowledgments
We are grateful to Lucien Aarden, PhD, Sanquin Research Institute, Netherlands and to Ricardo Fernandes, MD, Hospital de Santa Maria/Instituto de Medicina Molecular, Portugal, for the critical review of the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figure 1
- Data supplement 3 - Online figure 2
Lay summary
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Handling editor Tore K Kvien
-
Contributors All authors fulfil the authorship criteria.
-
Funding The Gulbenkian Programme for Advanced Medical Education is sponsored by Fundação Calouste Gulbenkian, Fundação Champalimaud, Ministério da Saúde and Fundação para a Ciência e Tecnologia, Portugal.
-
Competing interests None.
-
Ethics approval The study is a systematic review of the literature with a meta-analysis.
-
Provenance and peer review Not commissioned; externally peer reviewed.