
Carbapenems to Treat Multidrug and Extensively Drug-Resistant Tuberculosis: A Systematic Review

 ,
,  ,
,
Abstract
:
1. Introduction
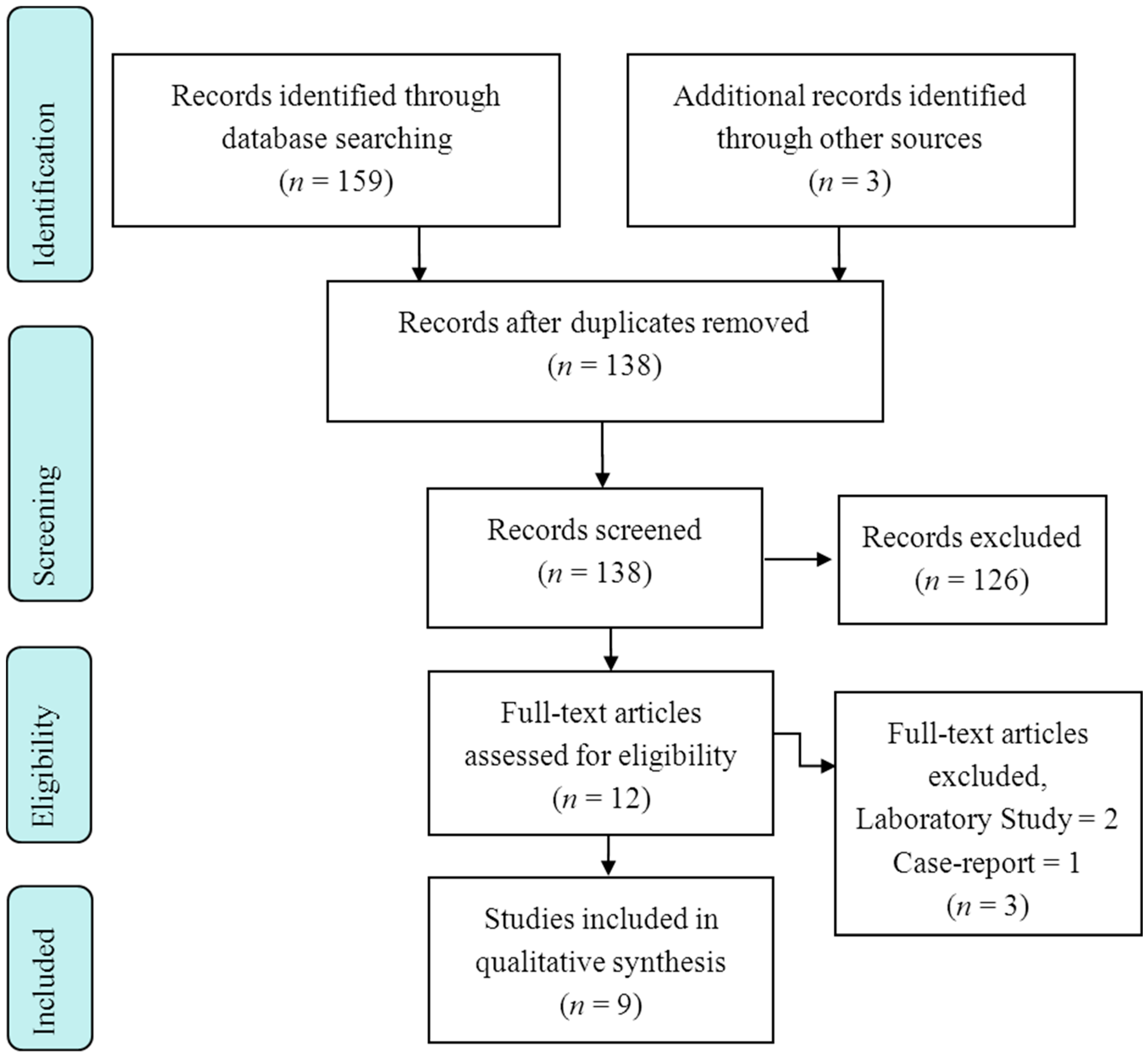
2. Methods
- (1)
- Case-reports describing fewer than 3 M/XDR-TB cases;
- (2)
- Experimental studies on animals with TB;
- (3)
- Reviews and editorials on carbapenems and M/XDR-TB; and
- (4)
- Unclear/unconfirmed M/XDR-TB diagnosis of treated patients.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2015; Document WHO/HTM/TB/2015.22; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Skrahina, A.; Hurevich, H.; Zalutskaya, A.; Sahalchyk, E.; Astrauko, A.; van Gemert, W.; Hoffner, S.; Rusovich, V.; Zignol, M. Alarming levels of drug-resistant tuberculosis in Belarus: Results of a survey in Minsk. Eur. Respir. J. 2012, 39, 1425–1431. [Google Scholar] [CrossRef] [PubMed]
- Migliori, G.B.; Sotgiu, G.; Gandhi, N.R.; Falzon, D.; DeRiemer, K.; Centis, R.; Hollm-Delgado, M.G.; Palmero, D.; Pérez-Guzmán, C.; Vargas, M.H.; et al. The Collaborative Group for Meta-Analysis of Individual Patient Data in MDR-TB. Drug resistance beyond extensively drug resistant tuberculosis: Individual patient data meta-analysis. Eur. Respir. J. 2013, 42, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Falzon, D.; Gandhi, N.; Migliori, G.B.; Sotgiu, G.; Cox, H.; Holtz, T.H.; Hollm-Delgado, M.G.; Keshavjee, S.; DeRiemer, K.; Centis, R.; et al. Collaborative Group for Meta-Analysis of Individual Patient Data in MDR-TB. Resistance to fluoroquinolones and second-line injectable drugs: Impact on multidrug-resistant TB outcomes. Eur. Respir. J. 2013, 42, 156–168. [Google Scholar] [CrossRef] [PubMed]
- Diel, R.; Rutz, S.; Castell, S.; Schaberg, T. Tuberculosis: Cost of illness in Germany. Eur. Respir. J. 2012, 40, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Diel, R.; Vandeputte, J.; de Vries, G.; Stillo, J.; Wanlin, M.; Nienhaus, A. Costs of tuberculosis disease in the European Union: A systematic analysis and cost calculation. Eur. Respir. J. 2014, 43, 554–565. [Google Scholar] [CrossRef] [PubMed]
- Falzon, D.; Jaramillo, E.; Schünemann, H.J.; Arentz, M.; Bauer, M.; Bayona, J.; Blanc, L.; Caminero, J.A.; Daley, C.L.; Duncombe, C.; et al. WHO guidelines for the programmatic management of drug-resistant tuberculosis: 2011 update. Eur. Respir. J. 2011, 38, 516–528. [Google Scholar] [CrossRef] [PubMed]
- Migliori, G.B.; de Iaco, G.; Besozzi, G.; Centis, R.; Cirillo, D.M. First tuberculosis cases in Italy resistant to all tested drugs. Eurosurveillance 2007, 12, E070517.1. [Google Scholar] [PubMed]
- Caminero, J.A.; Scardigli, A. Classification of antituberculosis drugs: A new proposal based on the most recent evidence. Eur. Respir. J. 2015, 46, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Pontali, E.; Migliori, G.B. Linezolid to treat MDR-/XDR-Tuberculosis: Available evidence and future scenarios. Eur. Respir. J. 2015, 45, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Emanuele, P.; Giovanni, S.; D’Ambrosio, L.; Rosella, C.; Giovanni, B.M. Bedaquiline and MDR-TB: A systematic and critical analysis of the evidence. Eur. Respir. J. 2016, in press. [Google Scholar]
- Esposito, S.; D’Ambrosio, L.; Tadolini, M.; Schaaf, H.S.; Luna, J.C.; Marais, B.; Centis, R.; Dara, M.; Matteelli, A.; Blasi, F.; et al. ERS/WHO Tuberculosis consilium assistance with extensively drug-resistant tuberculosis management in a child: Case study of compassionate delamanid use. Eur. Respir. J. 2014, 44, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Skripconoka, V.; Danilovits, M.; Pehme, L.; Tomson, T.; Skenders, G.; Kummik, T.; Cirule, A.; Leimane, V.; Kurve, A.; Levina, K.; et al. Delamanid improves outcomes and reduces mortality in multidrug-resistant tuberculosis. Eur. Respir. J. 2013, 41, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Gler, M.T.; Skripconoka, V.; Sanchez-Garavito, E.; Xiao, H.; Cabrera-Rivero, J.L.; Vargas-Vasquez, D.E.; Gao, M.; Awad, M.; Park, S.K.; Shim, T.S.; et al. Delamanid for multidrug-resistant pulmonary tuberculosis. N. Engl. J. Med. 2012, 366, 2151–2160. [Google Scholar] [CrossRef] [PubMed]
- Pym, A.S.; Diacon, A.H.; Tang, S.J.; Conradie, F.; Danilovits, M.; Chuchottaworn, C.; Vasilyeva, I.; Andries, K.; Bakare, N.; de Marez, T.; et al. Bedaquiline in the treatment of multi- and extensively drug-resistant tuberculosis. Eur. Respir. J. 2015. [Google Scholar] [CrossRef]
- Diacon, A.H.; Pym, A.; Grobusch, M.; Patientia, R.; Rustomjee, R.; Page-Shipp, L.; Pistorius, C.; Krause, R.; Bogoshi, M.; Churchyard, G.; et al. The diarylquinoline TMC207 for multidrug-resistant tuberculosis. N. Engl. J. Med. 2009, 360, 2397–2405. [Google Scholar] [CrossRef] [PubMed]
- Diacon, A.H.; Pym, A.; Grobusch, M.P.; de los Rios, J.M.; Gotuzzo, E.; Vasilyeva, I.; Leimane, V.; Andries, K.; Bakare, N.; de Marez, T.; et al. Multidrug-resistant tuberculosis and culture conversion with bedaquiline. N. Engl. J. Med. 2014, 371, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Guglielmetti, L.; Le Dû, D.; Jachym, M.; Henry, B.; Martin, D.; Caumes, E.; Veziris, N.; Métivier, N.; Robert, J.; Andrejak, C.; et al. Compassionate use of bedaquiline for the treatment of multidrug-resistant and extensively drug-resistant tuberculosis: Interim analysis of a French cohort. Clin. Infect. Dis. 2015, 60, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Ndjeka, N.; Conradie, F.; Schnippel, K.; Hughes, J.; Bantubani, N.; Ferreira, H.; Maartens, G.; Mametja, D.; Meintjes, G.; Padanilam, X.; et al. Treatment of drug-resistant tuberculosis with bedaquiline in a high HIV prevalence setting: An interim cohort analysis. Int. J. Tuberc. Lung Dis. 2015, 19, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Tiberi, S.; de Lorenzo, S.; Centis, R.; Viggiani, P.; D’Ambrosio, L.; Migliori, G.B. Bedaquiline in MDR/XDR-TB cases: First experience on compassionate use. Eur. Respir. J. 2014, 43, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Tiberi, S.; D’Ambrosio, L.; de Lorenzo, S.; Viggiani, P.; Centis, R.; Migliori, G.B. Tuberculosis elimination, patients’ lives and rational use of new drugs: Revisited. Eur. Respir. J. 2015. [Google Scholar] [CrossRef] [PubMed]
- Migliori, G.B.; Eker, B.; Richardson, M.D.; Sotgiu, G.; Zellweger, J.P.; Skrahina, A.; Ortmann, J.; Girardi, E.; Hoffmann, H.; Besozzi, G.; et al. A retrospective TBNET assessment of linezolid safety, tolerability and efficacy in MDR-TB. Eur. Respir. J. 2009, 34, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Villar, M.; Sotgiu, G.; D’Ambrosio, L.; Raymundo, E.; Fernandes, L.; Barbedo, J.; Diogo, N.; Lange, C.; Centis, R.; Migliori, G.B. Linezolid safety, tolerability and efficacy to treat multidrug- and extensively drug-resistant tuberculosis. Eur. Respir. J. 2011, 38, 730–733. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, S.; Centis, R.; D’Ambrosio, L.; Sotgiu, G.; Migliori, G.B. On linezolid efficacy and tolerability. Eur. Respir. J. 2012, 39, 770–772. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Centis, R.; D’Ambrosio, L.; Alffenaar, J.W.C.; Anger, H.A.; Caminero, J.A.; Castiglia, P.; de Lorenzo, S.; Ferrara, G.; Koh, W.J.; et al. Efficacy, safety and tolerability of linezolid containing regimens in treating MDR-TB and XDR-TB: Systematic review and meta-analysis. Eur. Respir. J. 2012, 40, 1430–1442. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Centis, R.; D’Ambrosio, L.; Spanevello, A.; Migliori, G.B. Linezolid to treat extensively drug-resistant TB: Retrospective data are confirmed by experimental evidence. Eur. Respir. J. 2013, 42, 288–290. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Lee, J.; Carroll, M.W.; Choi, H.; Min, S.; Song, T.; Via, L.E.; Goldfeder, L.C.; Kang, E.; Jin, B.; et al. Linezolid for treatment of chronic extensively drug-resistant tuberculosis. N. Engl. J. Med. 2012, 367, 1508–1518. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Centis, R.; D’Ambrosio, L.; Castiglia, P.; Migliori, G.B. Low minimal inhibitory concentrations of linezolid against multidrug-resistant tuberculosis strains. Eur. Respir. J. 2015, 45, 287–289. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, S.; Alffenaar, J.W.; Sotgiu, G.; Centis, R.; D’Ambrosio, L.; Tiberi, S.; Bolhuis, M.S.; van Altena, R.; Viggiani, P.; Piana, A.; et al. Efficacy and safety of meropenem-clavulanate added to linezolid-containing regimens in the treatment of MDR-/XDR-TB. Eur. Respir. J. 2013, 41, 1386–1392. [Google Scholar] [CrossRef] [PubMed]
- Payen, M.C.; de Wit, S.; Martin, C.; Sergysels, R.; Muylle, I.; van Laethem, Y.; Clumeck, N. Clinical use of meropenem-clavulanate combination for extensively drug-resistant tuberculosis. Int. J. Tuberc. Lung Dis. 2012, 16, 558–560. [Google Scholar] [CrossRef] [PubMed]
- Tiberi, S.; D’Ambrosio, L.; de Lorenzo, S.; Viggiani, P.; Centis, R.; Sotgiu, G.; Alffenaar, J.W.C.; Migliori, G.B. Ertapenem in the treatment of MDR-TB: First clinical experience. Eur. Respir. J. 2016, 47, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Van Rijn, S.P.; van Altena, R.; Akkerman, O.W.; van Soolingen, D.; van der Laan, T.; de Lange, W.C.M.; Kosterink, J.G.W.; van der Werf, T.S.; Alffenaar, J.W.C. Pharmacokinetics evaluation of ertapenem in patients with treatment of multidrug-resistant tuberculosis. Eur. Respir. J. 2016, in press. [Google Scholar]
- Chambers, H.F.; Turner, J.; Schecter, G.F.; Kawamura, M.; Hopewell, P.C. Hopewell. Imipenem for treatment of tuberculosis in mice and humans. Antimicrob. Agents Chemother. 2005, 49, 2816–2821. [Google Scholar] [CrossRef] [PubMed]
- Arbex, M.A.; Siqueira, H.R.D.; D’Ambrosio, L.; Migliori, G.B. The challenge of managing the extensively drug-resistant tuberculosis at a referral hospital in the state of São Paulo, Brazil: A report of three cases. J. Bras. Pneumol. 2015, 41, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Yew, W.W.; Wong, C.F.; Lee, J.; Wong, P.C.; Chan, C.H. Do β-lactam-β-lactmase inhibitor combinations have a place in the treatment of multidrug-resistant pulmonary tuberculosis? Tuber. Lung Dis. 1995, 78, 90–92. [Google Scholar] [CrossRef]
- Hugonnet, J.E.; Blanchard, J.S. Irreversible inhibition of Mycobacterium tuberculosis β-lactamase by clavulanate. Biochemistry 2007, 46, 11198–12004. [Google Scholar] [CrossRef] [PubMed]
- Hugonnet, J.E.; Tremblay, L.W.; Boshoff, H.I.; Barry, C.E.; Blanchard, J.S. Meropenem-clavulanate is effective against extensively drug-resistant Mycobacterium tuberculosis. Science 2009, 323, 1215–1218. [Google Scholar] [CrossRef] [PubMed]
- Payen, M.; Martin, C.; Antoine-Moussiaux, T.; de Wit, S.; Clumeck, N. Four Cases of XDR-TB Treated with Meropenem-Clavulanate. In Proceedings of the 50th Interscience Conference of Antimicrobial Agents and Chemotherapy (ICAAC), Boston, MA, USA, 12–15 September 2010.
- Veziris, N.; Truffot, C.; Mainardi, J.L.; Jarlier, V. Activity of carbapenems combined with clavulanate against murine tuberculosis. Antimicrob. Agents Chemother. 2011, 55, 2597–2600. [Google Scholar] [CrossRef] [PubMed]
- Palmero, D.; Montaner, P.G.; Cufré, M.; García, A.; Vescovo, M.; Poggi, S. First series of patients with XDR and pre-XDR TB treated with regimens that included meropenen-clavulanate in Argentina. Arch. Bronconeumol. 2015, 51, e49–e52. [Google Scholar] [CrossRef] [PubMed]
- Tiberi, S.; Payen, M.-C.; Sotgiu, G.; D’Ambrosio, L.; Guizado, V.A.; Alffenaar, J.W.; Arbex, M.A.; Caminero, J.A.; Centis, R.; de Lorenzo, S.; et al. Effectiveness and safety of meropenem/clavulanate-containing regimens in the treatment of multidrug and extensively drug-resistant tuberculosis. Eur. Respir. J. 2016, in press. [Google Scholar] [CrossRef]
- Tiberi, S.; Sotgiu, G.; D’Ambrosio, L.; Centis, R.; Arbex, M.A.; Alarcon, A.E.; Alffenaar, J.W.; Caminero, J.A.; Gaga, M.; Gualano, G.; et al. Comparison of effectiveness and safety of imipenem/clavulanate added to an optimised background regimen (OBR) versus OBR controls regimens in the treatment of multidrug and extensively drug-resistant tuberculosis. Clin. Infect. Dis. 2016. [Google Scholar] [CrossRef] [PubMed]
- Tiberi, S.; Sotgiu, G.; D’Ambrosio, L.; Centis, R.; Arbex, M.A.; Alarcon, A.E.; Alffenaar, J.W.; Caminero, J.A.; Gaga, M.; Gualano, G.; et al. Comparison of effectiveness and safety of imipenem/clavulanate-versus meropenem/clavulanate-containing regimens in the treatment of multidrug and extensively drug-resistant tuberculosis. Eur. Respir. J. 2016, in press. [Google Scholar]
- World Health Organization. Definitions and Reporting Framework for Tuberculosis—2013 Revision; 2013 Document WHO/HTM/TB/2013.2; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred reporting items for systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Kempker, R.R.; Kipiani, M.; Mirtskhulava, V.; Tukvadze, N.; Magee, M.J.; Blumberg, H.M. Acquired drug resistance in mycobacterium tuberculosis and poor outcomes among patients with multidrug-resistant tuberculosis. Emerg. Infect. Dis. 2015, 21, 992. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials. Available online: https://clinicaltrials.gov (accessed on 26 February 2016).
- Sotgiu, G.; Mauch, V.; Migliori, G.B.; Benedetti, A. Evidence-based, agreed-upon health priorities to remedy the tuberculosis patient’s economic disaster. Eur. Respir. J. 2014, 43, 1563–1566. [Google Scholar] [CrossRef] [PubMed]
- Winters, N.; Butler-Laporte, G.; Menzies, D. Efficacy and safety of World Health Organization group 5 drugs for multidrug-resistant tuberculosis treatment. Eur. Respir. J. 2015, 46, 1461–1470. [Google Scholar] [CrossRef] [PubMed]
- Alsaad, N.; Wilffert, B.; van Altena, R.; de Lange, W.C.; van der Werf, T.S.; Kosterink, J.G.; Alffenaar, J.W.C. Potential antimicrobial agents for the treatment of multidrug-resistant tuberculosis. Eur. Respir. J. 2014, 43, 884–897. [Google Scholar] [CrossRef] [PubMed]
- Alsaad, N.; van Altena, R.; Pranger, A.D.; van Soolingen, D.; de Lange, W.C.; van der Werf, T.S.; Kosterink, J.G.; Alffenaar, J.W.C. Evaluation of co-trimoxazole in the treatment of multidrug-resistant tuberculosis. Eur. Respir. J. 2013, 42, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Krieger, D.; Vesenbeckh, S.; Schönfeld, N.; Bettermann, G.; Bauer, T.T.; Rüssmann, H.; Mauch, H. Mefloquine as a potential drug against multidrug-resistant tuberculosis. Eur. Respir. J. 2015, 46, 1503–1505. [Google Scholar] [CrossRef] [PubMed]
- Matteelli, A.; D’Ambrosio, L.; Centis, R.; Tadolini, M.; Migliori, G.B. Compassionate and optimum use of new tuberculosis drugs. Lancet Infect. Dis. 2015, 15, 1131–1132. [Google Scholar] [CrossRef]
- Lönnroth, K.; Migliori, G.B.; Abubakar, I.; D’Ambrosio, L.; de Vries, G.; Diel, R.; Douglas, P.; Falzon, D.; Gaudreau, M.A.; Goletti, D.; et al. Towards tuberculosis elimination: An action framework for low-incidence countries. Eur. Respir. J. 2015, 45, 928–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| First Author | Publication Year | Country | Study Design | Clinical Setting | Study Duration |
|---|---|---|---|---|---|
| Chambers H.F. [33] | 2005 | USA | Prospective | Monocenter, university clinical research center in collaboration with a general hospital | ND |
| Palmero D. [40] | 2015 | Argentina | Retrospective | Monocenter, university medical centre | 2012–2013 |
| De Lorenzo S. [29] | 2013 | Italy, The Netherlands | Retrospective, case-control | Multicenter, university medical center and general hospital | 2001–2012 |
| van Rijn S.P. [32] | 2016 | The Netherlands | Retrospective | Monocenter, university medical center | 2010–2013 |
| Tiberi S. [31] | 2016 | Italy, The Netherlands | Retrospective | Multicenter, university medical center and general hospital | 2008–2015 |
| Tiberi S. [41] | 2016 | Italy, The Netherlands, Belgium, United Kingdom, Greece, Peru, Brazil, Spain, France, Ecuador, Belarus, Slovakia | Retrospective, cohort | Multicenter, university medical centers and general hospitals | 2003–2015 |
| Payen M.C. [30] | 2012 | Belgium | Retrospective | Monocenter, university medical centre | 2009–ND |
| Tiberi S. [42] | 2016 | Italy, The Netherlands, Belgium, United Kingdom, Greece, Peru, Brazil, Spain, France, Ecuador, Belarus, Slovakia | Retrospective, cohort | Multicenter, university medical centers and general hospitals | 2003–2015 |
| Tiberi S. [43] * | 2016 | Italy, The Netherlands, Belgium, United Kingdom, Greece, Peru, Brazil, Spain, France, Ecuador, Belarus, Slovakia | Retrospective, cohort | Multicenter, university medical centers and general hospitals | 2005–2015 |
| First Author | Individuals Exposed to Carbapenems | Paediatric Patients | Control Group | XDR-TB Cases (%) | Carbapenem Administered | Carbapenem Dosage |
|---|---|---|---|---|---|---|
| Chambers H.F. [33] | 10 | No | No | 2/10 (20.0) | Imipenem | 1 g bid |
| Palmero D. [40] | 10 | No | No | 4/10 (40.0) | Meropenem | 2 g tid, then 2 g tid |
| De Lorenzo S. [29] | 37 | No | Yes | 9/37 (24.3) | Meropenem | 1 g tid |
| Van Rijn S.P. [32] | 18 | Yes; ND | No | ND | Ertapenem | 1 g qd |
| Tiberi S. [31] | 5 | No | No | 2/5 (40.0) | Ertapenem | 1 g qd |
| Tiberi S. [41] | 96 | No | Yes | 47/96 (49.0) | Meropenem | 1 g tid (2 g tid in Belgium) |
| Payen M.C. [30] | 6 | 1/6 | No | 6/6 (100.0) | Meropenem | 2 g tid, then 2 g bid |
| Tiberi S. [42] | 84 | No | Yes | 57/84 (67.9) | Imipenem | 500 mg qid |
| Tiberi S. [43] * | 84 Imipenem 96 Meropenem | No | No | 57/84 (67.9) Imipenem 47/96 (49.0) Meropenem | Imipenem Meropenem | Imipenem: 500 mg qid Meropenem: 1 g tid (2 g tid in Belgium) |
| First Author | Sputum Smear Conversion (%) | Sputum Culture Conversion (%) | Treatment Success (%) ** | Adverse events Attributed to Carbapenems (%) | Interruption of Carbapenems Due to Adverse Events (%) |
|---|---|---|---|---|---|
| Chambers H.F. [33] | ND | 7/9 (77.8) | 7/10 (70.0) | ND | ND |
| Palmero D. [40] | ND | 8/10 (80.0) | 3/6 (50.0) | 0/10 (0.0) | ND |
| De Lorenzo S. [29] | 28/32 (87.5) | 31/37 (83.8) | ND | 5/37 (13.5) | 2/5 (40.0) |
| van Rijn S.P. [32] | ND | 15/18 (83.3) | 15/18 (83.3) | 2/18 (11.1) | 3/18 (16.7) |
| Tiberi S. [31] | 3/5 (60.0) | 3/5 (60.0) | 4/5 (80.0) | 0/5 (0.0) | 2/5 (40.0) |
| Tiberi S. [41] | 55/58 (94.8) | 55/58 (94.8) | 55/96 (57.3) | 6/93 (6.5) | 8/94 (8.5) |
| Payen M.C. [30] | 5/6 (83.3) | 5/6 (83.3) | ND | 0/6 (0.0) | 0/6 (0.0) |
| Tiberi S. [42] | 51/64 (79.7) | 46/64 (71.9) | 34/57 (59.7) | 3/56 (5.4) | 4/55 (7.3) |
| Tiberi S. [43] * | Imipenem 51/64 (79.7) Meropenem 55/58 (94.8) | Imipenem 46/64 (71.9) Meropenem 55/58 (94.8) | Imipenem 34/57 (59.7) Meropenem 55/71 (77.5) | Imipenem 3/56 (5.4) Meropenem 6/93 (6.5) | Imipenem 4/55 (7.3) Meropenem 8/94 (8.5) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sotgiu, G.; D’Ambrosio, L.; Centis, R.; Tiberi, S.; Esposito, S.; Dore, S.; Spanevello, A.; Migliori, G.B. Carbapenems to Treat Multidrug and Extensively Drug-Resistant Tuberculosis: A Systematic Review. Int. J. Mol. Sci. 2016, 17, 373. https://doi.org/10.3390/ijms17030373
Sotgiu G, D’Ambrosio L, Centis R, Tiberi S, Esposito S, Dore S, Spanevello A, Migliori GB. Carbapenems to Treat Multidrug and Extensively Drug-Resistant Tuberculosis: A Systematic Review. International Journal of Molecular Sciences. 2016; 17(3):373. https://doi.org/10.3390/ijms17030373
Chicago/Turabian StyleSotgiu, Giovanni, Lia D’Ambrosio, Rosella Centis, Simon Tiberi, Susanna Esposito, Simone Dore, Antonio Spanevello, and Giovanni Battista Migliori. 2016. "Carbapenems to Treat Multidrug and Extensively Drug-Resistant Tuberculosis: A Systematic Review" International Journal of Molecular Sciences 17, no. 3: 373. https://doi.org/10.3390/ijms17030373