Cross-Sectional Analysis of the Utility of Pulmonary Function Tests in Predicting Emphysema in Ever-Smokers

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
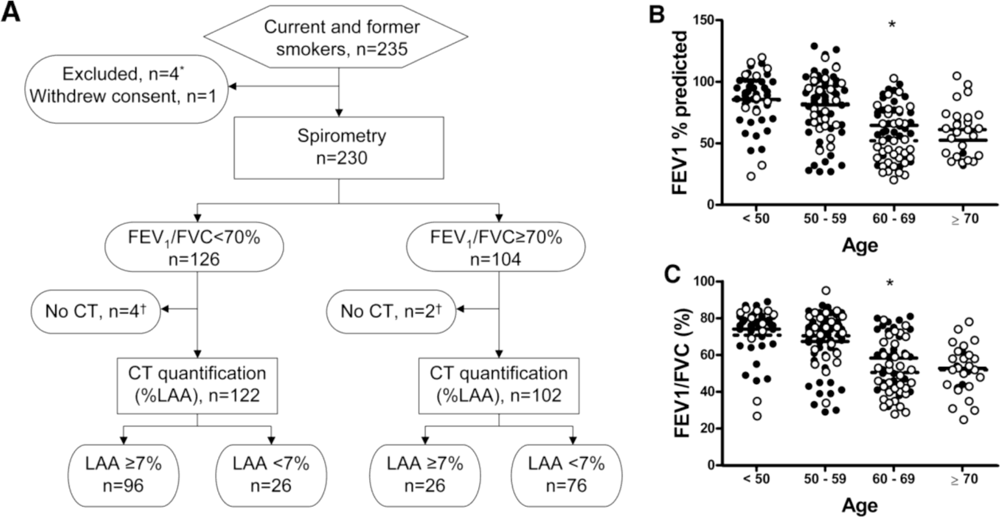
2.1. Clinical and Demographic Characteristic of the Study Participants
2.2. Phenotypic Characterization of Former and Current Smokers
2.3. Quantitative CT Morphometry Assessment of Emphysema
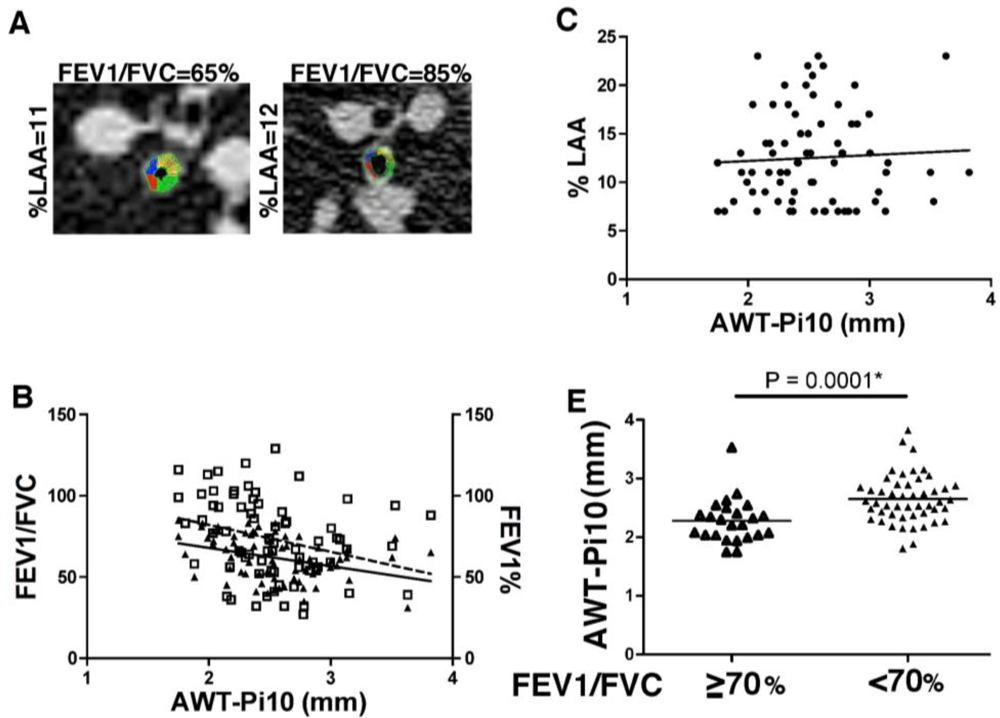
2.4. Measurement of Airway Wall Thickness
2.5. Statistical Analysis
3. Results
3.1. Demographics Distributed by GOLD Classification and CT Evidence of Emphysema
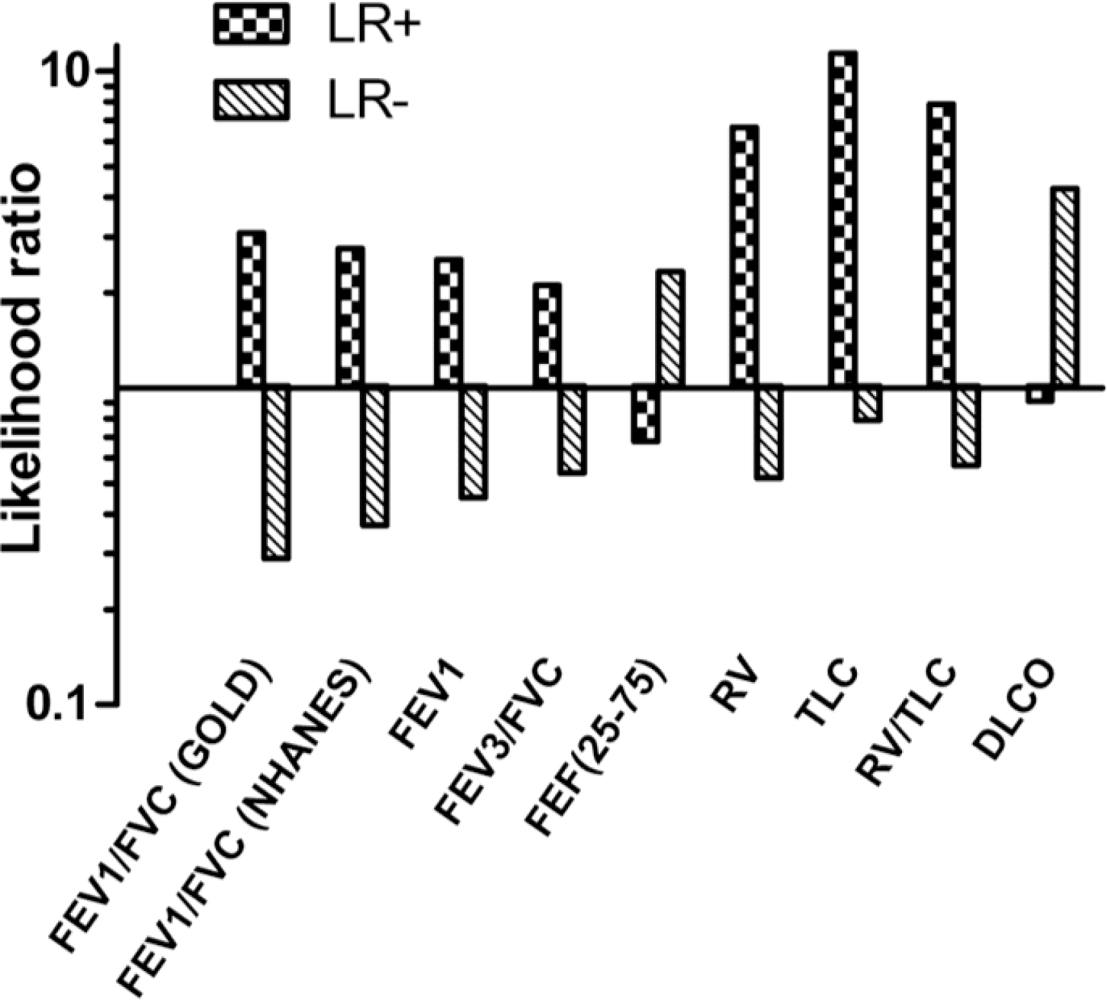
3.2. Diagnostic Value of Pulmonary Function Tests in Emphysema
3.3. Correlation between CT Emphysema and Pulmonary Function Tests
3.4. Airway Wall Thickness Is Associated with Airway Obstruction but Not Emphysema
4. Discussion and Conclusions
Acknowledgments
References
- Centers for Disease Control and Prevention (CDC). State-specific prevalence and trends in adult cigarette smoking—United States, 1998–2007. MMWR 2009, 58, 221–226. [Google Scholar]
- Shafey, O; Eriksen, M; Ross, H; Mackay, J. The Tobacco Atlas, 3rd ed; American Cancer Society: Atlanta, GA, USA, 2009. [Google Scholar]
- Schubert, C. Anti-tobacco efforts going up in smoke. Nature Med 2006, 12, 866. [Google Scholar]
- Rennard, SI; Vestbo, J. COPD: The dangerous underestimate of 15%. Lancet 2006, 367, 1216–1219. [Google Scholar]
- Rennard, SI; Vestbo, J. Natural histories of chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc 2008, 5, 878–883. [Google Scholar]
- Shan, M; Cheng, HF; Song, LZ; Roberts, L; Green, L; Hacken-Bitar, J; Huh, J; Bakaeen, F; Coxson, HO; Storness-Bliss, C; et al. Lung myeloid dendritic cells coordinately induce Th1 and Th17 responses in human emphysema. Sci. Transl. Med 2009, 4, 132–140. [Google Scholar]
- Freeman, CM; Martinez, FJ; Han, MK; Ames, TM; Chensue, SW; Todt, JC; Arenberg, DA; Meldrum, CA; Getty, C; McCloskey, L; et al. Lung dendritic cell expression of maturation molecules increases with worsening chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med 2009, 180, 1179–1188. [Google Scholar]
- Silverman, EK; Spira, A; Pare, PD. Genetics and genomics of chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc 2009, 6, 539–542. [Google Scholar]
- Stavem, K; Aaser, E; Sandvik, L; Bjornholt, J; Erikssen, G; Thaulow, E; Erikssen, J. Lung function, smoking and mortality in a 26-year follow-up of healthy middle-aged males. Eur. Resp. J 2005, 4, 618–625. [Google Scholar]
- Kim, WJ; Silverman, EK; Hoffman, E; Criner, GJ; Mosenifar, Z; Sciurba, FC; Make, BJ; Carey, V; San Jose Estepar, R; Diaz, A; et al. CT metrics of airway disease and emphysema in severe COPD. Chest 2009, 136, 396–404. [Google Scholar]
- Han, MK; Bartholmai, B; Liu, LX; Murray, S; Curtis, JL; Sciurba, FC; Kazerooni, EA; Thompson, B; Frederick, M; Li, D; et al. Clinical significance of radiologic characterizations in COPD. COPD 2009, 6, 459–467. [Google Scholar]
- Pescarolo, M; Sverzellati, N; Verduri, A; Chetta, A; Marangio, E; De Filippo, M; Olivieri, D; Zompatori, M. How much do GOLD stages reflect CT abnormalities in COPD patients? Radiol. Med 2008, 113, 817–829. [Google Scholar]
- Anthonisen, NR; Connett, JE; Murray, RP. Smoking and lung function of Lung Health Study participants after 11 years. Am. J. Respir. Crit. Care Med 2002, 166, 675–679. [Google Scholar]
- Pellegrino, R; Viegi, G; Brusasco, V; Crapo, RO; Burgos, F; Casaburi, R; Coates, A; van der Grinten, CPM; Gustafsson, P; Hankinson, J; et al. Interpretative strategies for lung function tests. Eur. Respir. J 2005, 26, 948–968. [Google Scholar]
- Stocks, J; Quanjer, PH. Reference values for residual volume, functional residual capacity and total lung capacity—ATS workshop on lung volume measurements. Official statement of the european respiratory society. Eur. Respir. J 1995, 8, 492–506. [Google Scholar]
- GOLD Executive Committee. Global Strategy for the Diagnosis, Management, and Prevention of COPD. Available online: http://www.goldcopd.com/GuidelinesResources.asp?l1=2&l2=0.2008 (accessed on 21 May 2009).
- Han, MK; Agusti, A; Calverley, PM; Celli, BR; Criner, G; Curtis, JL; Fabbri, LM; Goldin, JG; Jones, PW; Macnee, W; et al. Chronic obstructive pulmonary disease phenotypes: The future of COPD. Am. J. Respir. Crit. Care Med 2010, 182, 598–604. [Google Scholar]
- Gu, D; Kelly, TN; Wu, X; Chen, J; Samet, JM; Huang, JF; Zhu, ML; Chen, JC; Chen, CS; Duan, XF; et al. Mortality attributable to smoking in China. N. Engl. J. Med 2009, 360, 150–159. [Google Scholar]
- Spitz, MR; Hong, WK; Amos, CI; Wu, X; Schabath, MB; Dong, Q; Shete, S; Etzel, CJ. A risk model for prediction of lung cancer. J. Nat. Cancer Inst 2007, 99, 715–726. [Google Scholar]
- Wilson, DO; Weissfeld, JL; Balkan, A; Schragin, JG; Fuhrman, CR; Fisher, SN; Wilson, J; Leader, JK; Siegfried, JM; Shapiro, SD. Association of radiographic emphysema and airflow obstruction with lung cancer. Am. J. Respir. Crit. Care Med 2008, 178, 738–744. [Google Scholar]
- Houghton, AM; Mouded, M; Shapiro, SD. Common origins of lung cancer and COPD. Nature Med 2008, 14, 1023–1024. [Google Scholar]
- Punturieri, A; Szabo, E; Croxton, TL; Shapiro, SD; Dubinett, SM. Lung cancer and chronic obstructive pulmonary disease: Needs and opportunities for integrated research. J. Nat. Cancer Inst 2009, 101, 554–559. [Google Scholar]
- van Klaveren, RJ; de Koning, HJ; Mulshine, J; Hirsch, FR. Lung cancer screening by spiral CT. What is the optimal target population for screening trials? Lung Cancer 2002, 38, 243–252. [Google Scholar]
- Haruna, A; Muro, S; Nakano, Y; Ohara, T; Hoshino, Y; Ogawa, E; Hirai, T; Niimi, A; Nishimura, K; Chin, K; et al. CT scan findings of emphysema predict mortality in COPD. Chest 2010, 138, 635–640. [Google Scholar]
- Gevenois, PA; de Maertelaer, V; De Vuyst, P; Zanen, J; Yernault, JC. Comparison of computed density and macroscopic morphometry in pulmonary emphysema. Am. J. Respir. Crit. Care Med 1995, 152, 653–657. [Google Scholar]
- Gevenois, PA; De Vuyst, P; de Maertelaer, V; Zanen, J; Jacobovitz, D; Cosio, MG; Yernault, JC. Comparison of computed density and microscopic morphometry in pulmonary emphysema. Am. J. Respir. Crit. Care Med 1996, 154, 187–192. [Google Scholar]
- Patel, BD; Coxson, HO; Pillai, SG; Agusti, AGN; Calverley, PMA; Donner, CF; Make, BJ; Müller, NL; Rennard, SI; Vestbo, J; et al. Airway wall thickening and emphysema show independent familial aggregation in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med 2008, 178, 500–505. [Google Scholar]
- Grydeland, TB; Dirksen, A; Coxson, HO; Eagan, TML; Thorsen, E; Pillai, SG; Sharma, S; Eide, GE; Gulsvik, A; Bakke, PS. Quantitative computed tomography measures of emphysema and airway wall thickness are related to respiratory symptoms. Am. J. Respir. Crit. Care Med 2010, 181, 353–359. [Google Scholar]
- Orlandi, I; Moroni, C; Camiciottoli, G; Bartolucci, M; Pistolesi, M; Villari, N; Mascalchi, M. Chronic obstructive pulmonary disease: Thin-section CT measurement of airway wall thickness and lung attenuation. Radiology 2005, 234, 604–610. [Google Scholar]
- Coxson, HO; Rogers, RM. Quantitative computed tomography of chronic obstructive pulmonary disease. Acad. Radiol 2005, 12, 1457–1463. [Google Scholar]
- Gelb, AF; McKenna, RJ, Jr; Brenner, M; Fischel, R; Baydur, A; Zamel, N. Contribution of lung and chest wall mechanics following emphysema resection. Chest 1996, 110, 11–17. [Google Scholar]
- Hesselbacher, SE; Perusich, S; Barrow, N; Smithwick, P; Coxson, HO; Krowchuk, N; Corry, D; Ross, R; Kheradmand, F. Physiological impairment in smokers with emphysema. Am. J. Respir. Crit. Care Med 2010, 181, A5952. [Google Scholar]
- Hankinson, JL; Odencrantz, JR; Fedan, KB. Spirometric reference values from a sample of the general U.S. population. Am. J. Respir. Crit. Care Med 1999, 159, 179–187. [Google Scholar]
- Crapo, RO; Morris, AH. Standardized single breath normal values for carbon monoxide diffusing capacity. Amer. Rev. Resp. Dis 1981, 123, 185–189. [Google Scholar]
- Cotes, JE; Chinn, DJ; Reed, JW. Body mass, fat percentage, and fat free mass as reference variables for lung function: Effects on terms for age and sex. Thorax 2001, 56, 839–844. [Google Scholar]
- Miller, A; Thornton, JC; Warshaw, R; Anderson, H; Teirstein, AS; Selikoff, IJ. Single breath diffusing capacity in a representative sample of the population of Michigan, a large industrial state. Predicted values, lower limits of normal, and frequencies of abnormality by smoking history. Amer. Rev. Resp. Dis 1983, 127, 270–277. [Google Scholar]
- Yuan, R; Hogg, JC; Pare, PD; Sin, DD; Wong, JC; Nakano, Y; McWilliams, AM; Lam, S; Coxson, HO. Prediction of the rate of decline in FEV(1) in smokers using quantitative computed tomography. Thorax 2009, 64, 944–999. [Google Scholar]
- Yuan, R; Mayo, JR; Hogg, JC; Pare, PD; McWilliams, AM; Lam, S; Coxson, HO. The effects of radiation dose and CT manufacturer on measurements of lung densitometry. Chest 2007, 132, 617–623. [Google Scholar]
- Bosken, CH; Wiggs, BR; Pare, PD; Hogg, JC. Small airway dimensions in smokers with obstruction to airflow. Am. Rev. Respir. Dis 1990, 142, 563–570. [Google Scholar]
- Nakano, Y; Muro, S; Sakai, H; Hirai, T; Chin, K; Tsukino, M; Nishimura, K; Itoh, H; Paré, PD; Hogg, JC; et al. Computed tomographic measurements of airway dimensions and emphysema in smokers. Correlation with lung function. Am. J. Respir. Crit. Care Med 2000, 162, 1102–1108. [Google Scholar]
- Nakano, Y; Wong, JC; de Jong, PA; Buzatu, L; Nagao, T; Coxson, HO; Elliott, WM; Hogg, JC; Paré, PD. The prediction of small airway dimensions using computed tomography. Am. J. Respir. Crit. Care Med 2004, 171, 142–146. [Google Scholar]
- Feinstein, AR. Principles of Medical Statistics; Chapman & Hall/CRC: Boca Raton, FL, USA, 2002. [Google Scholar]
- Coxson, HO; Rogers, RM; Whittall, KP; D’Yachkova, Y; Pare, PD; Sciurba, FC; Hogg, JC. A quantification of the lung surface area in emphysema using computed tomography. Am. J. Respir. Crit. Care Med 1999, 159, 851–856. [Google Scholar]
- Coxson, HO; Chan, IH; Mayo, JR; Hlynsky, J; Nakano, Y; Birmingham, CL. Early emphysema in patients with anorexia nervosa. Am. J. Respir. Crit. Care Med 2004, 170, 748–752. [Google Scholar]
- Gillooly, M; Lamb, D. Airspace size in lungs of lifelong non-smokers: Effect of age and sex. Thorax 1993, 48, 39–43. [Google Scholar]
- Sansores, RH; Pare, PD; Abboud, RT. Acute effect of cigarette smoking on the carbon monoxide diffusing capacity of the lung. Am. Rev. Respir. Dis 1992, 146, 951–958. [Google Scholar]
- Remy-Jardin, M; Remy, J; Boulenguez, C; Sobaszek, A; Edme, JL; Furon, D. Morphologic effects of cigarette smoking on airways and pulmonary parenchyma in healthy adult volunteers: CT evaluation and correlation with pulmonary function tests. Radiology 1993, 186, 107–115. [Google Scholar]
- Spaggiari, E; Zompatori, M; Verduri, A; Chetta, A; Ormitti, F; Sverzellati, N; Rabaiotti, E. Early smoking-induced lung lesions in asymptomatic subjects. Correlations between high resolution dynamic CT and pulmonary function testing. Radiol. Med 2005, 109, 27–39. [Google Scholar]
- Sashidhar, K; Gulati, M; Gupta, D; Monga, S; Suri, S. Emphysema in heavy smokers with normal chest radiography. Detection and quantification by HCRT. Acta Radiol 2002, 43, 60–65. [Google Scholar]
- Soejima, K; Yamaguchi, K; Kohda, E; Takeshita, K; Ito, Y; Mastubara, H; Oguma, T; Inoue, T; Okubo, Y; Amakawa, K; et al. Longitudinal follow-up study of smoking-induced lung density changes by high-resolution computed tomography. Am. J. Respir. Crit. Care Med 2000, 161, 1264–1273. [Google Scholar]
- Group NETTR. A randomized trial comparing lung-volume—reduction surgery with medical therapy for severe emphysema. N. Engl. J. Med 2003, 348, 2059–2073. [Google Scholar]
- Wood, DE; McKenna, RJ, Jr; Yusen, RD; Sterman, DH; Ost, DE; Springmeyer, SC; Gonzalez, HX; Mulligan, MS; Gildea, T; Houck, WV; et al. A multicenter trial of an intrabronchial valve for treatment of severe emphysema. J. Thorac. Cardiovasc. Surg 2007, 133, 65–73. [Google Scholar]
- Smith-Bindman, R; Lipson, J; Marcus, R; Kim, KP; Mahesh, M; Gould, R; de González, BA; Miglioretti, DL. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch. Intern. Med 2009, 169, 2078–2086. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | NGC (previously Stage 0) | COPD (GOLD) | |||
|---|---|---|---|---|---|
| (I) | (II) | (III) | (IV) | ||
| Number | 102 | 18 | 55 | 39 | 10 |
| Age, mean (±s.d.) | 53 ± 8 | 55 ± 9 | 64 ± 9 | 64 ± 9 | 59 ± 7 |
| Height, cm (±s.d.) | 170 ± 9 | 174 ± 11 | 174 ± 9 | 175 ± 8 | 173 ± 8 |
| Weight, kg (±s.d.) | 88 ± 21 | 79 ± 12 | 88 ± 18 | 80 ± 19 | 74 ± 16 |
| Male, no. (%) | 42 (41%) | 14 (78%) | 46 (84%) | 35 (90%) | 8 (80%) |
| Ethnicity, no. (%) | |||||
| Black | 60 (59%) | 7 (39%) | 12 (22%) | 13 (33%) | 2 (20%) |
| Hispanic | 4 (4%) | 1 (6%) | 1 (2%) | 1 (3%) | 1 (10%) |
| White | 35 (34%) | 13 (56%) | 42 (76%) | 25 (64%) | 7 (70%) |
| Other | 3 (3%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Smoking status, no. (%) | |||||
| Current | 72 (71%) | 14 (78%) | 29 (53%) | 14 (36%) | 4 (40%) |
| Former | 30 (29%) | 4 (22%) | 26 (47%) | 25 (64%) | 6 (60%) |
| Pack-years, mean (±s.d.) | 33 ± 30 | 40 ± 18 | 69 ± 41 | 66 ± 35 | 62 ± 24 |
| Quitting years, mean (±s.d.) | 14 ± 11 | 21 ± 11 | 12 ± 11 | 9 ± 10 | 9 ± 6 |
| Lung Function | |||||
| % FEV1 (±s.d.) | 92 ± 15 | 90 ± 7 | 64 ± 8 | 39 ± 5 | 25 ± 3 |
| FEV1/FVC ratio (±s.d.) | 78 ± 5 | 66 ± 4 | 56 ± 8 | 42 ± 8 | 34 ± 5 |
| % DLCO (±s.d.) | 78 ± 16 | 63 ± 20 | 59 ± 14 | 42 ± 15 | 35 ± 13 |
| CT Quantification | LAA < 7% No emphysema | LAA ≥ 7% Emphysema |
|---|---|---|
| Number | 102 | 122 |
| Age, mean (±s.d.) | 53 ± 8 | 62 ± 10 |
| Height, cm (±s.d.) | 170 ± 10 | 174 ± 9 |
| Weight, kg (±s.d.) | 85 ± 20 | 86 ± 19 |
| Male, no. (%) | 45 (44%) | 100 (82%) |
| Ethnicity, no. (%) | ||
| Black | 59 (58%) | 35 (29%) |
| Hispanic | 4 (4%) | 4 (3%) |
| White | 37 (36%) | 82 (67%) |
| Other | 2 (2%) | 1 (1%) |
| Smoking status, no. (%) | ||
| Current | 84 (82%) | 49 (40%) |
| Former | 18 (18%) | 73 (60%) |
| Pack-years, mean (±s.d.) | 41 ± 36 | 56 ± 36 |
| Quitting years, mean (±s.d.) | 13 ± 13 | 12 ± 10 |
| Lung function | ||
| %FEV1 (±s.d.) | 87 ± 18 | 62 ± 26 |
| FEV1/FVC (±s.d.) | 74 ± 10 | 55 ± 16 |
| %DLCO (±s.d.) | 74 ± 16 | 57 ± 22 |
| Criteria | Sensitivity % (95% CI) | Specificity % (95% CI) | LR+ | LR− | PPV % | NPV % |
|---|---|---|---|---|---|---|
| FEV1/FVC < 70% | 79 (71–85) | 75 (65–82) | 3.09 | 0.29 | 79 | 75 |
| FEV1/FVC < LLN (NHANES) | 73 (65–80) | 74 (64–81) | 2.76 | 0.37 | 77 | 68 |
| FEV1< LLN | 67 (59–75) | 74 (64–81) | 2.54 | 0.45 | 75 | 65 |
| FEV3/FVC < LLN | 62 (53–70) | 71 (62–79) | 2.11 | 0.54 | 71 | 61 |
| FEF25–75 < LLN | 68 (59–76) | 43 (34–53) | 0.68 | 2.32 | 59 | 54 |
| RV > ULN | 52 (43–61) | 92 (86–96) | 6.64 | 0.52 | 89 | 62 |
| TLC > ULN | 22 (16–30) | 98 (94–100) | 11.38 | 0.79 | 93 | 52 |
| RV/TLC > ULN | 46 (38–55) | 94 (88–98) | 7.87 | 0.57 | 90 | 60 |
| DLCO < LLN | 91 (84–95) | 23 (16–33) | 0.91 | 4.26 | 59 | 68 |
| Criteria | Sensitivity % (95% CI) | Specificity % (95% CI) | LR+ | LR− |
|---|---|---|---|---|
| FEV1/FVC < 70% and FEV1/FVC < LLN (NHANES) | 79 (71–85) | 74 (64–81) | 2.97 | 0.29 |
| FEV1/FVC < 70% and RV/TLC > ULN | 79 (72–87) | 72 (62–80) | 2.79 | 0.29 |
| FEV1/FVC <70% and FEV1 < LLN | 80 (73–87) | 63 (53–72) | 2.16 | 0.31 |
| FEV1/FVC < 70% and FEV3/FVC < LLN | 80 (72–87) | 65 (54–73) | 2.27 | 0.31 |
| FEV1/FVC < 70% and TLC > ULN | 80 (72–87) | 74 (64–81) | 3.03 | 0.27 |
| FEV1/FVC < 70% and RV > ULN | 81 (73–87) | 70 (60–78) | 2.66 | 0.27 |
| FEV1/FVC < 70% and RV > ULN and TLC > ULN | 82 (74–88) | 70 (60–78) | 2.69 | 0.26 |
| FEV1/FVC < 70% and FEF25–75 < LLN | 84 (77–90) | 38 (29–48) | 1.36 | 0.41 |
| FEV1/FVC < 70% and FEV1 < LLN and FEV3/FVC < LLN and FEF25–75 < LLN | 87 (80–92) | 27 (19–37) | 1.20 | 0.48 |
| FEV1/FVC < 70% and FEV3/FVC < LLN and DLCO < LLN | 93 (87–97) | 16 (10–25) | 1.11 | 0.42 |
| FEV1/FVC<70% and DLCO<LLN | 93 (87–97) | 21 (14–30) | 1.19 | 0.32 |
| FEV1/FVC < 70% and DLCO < LLN and RV/TLC > ULN | 93 (87–97) | 21 (14–30) | 1.19 | 0.32 |
| FEV1/FVC < 70% and DLCO < LLN and RV > ULN | 94 (89–97) | 21 (14–30) | 1.20 | 0.28 |
| FEV1/FVC < 70% and FEF25–75 < LLN and DLCO < LLN | 95 (90–98) | 13 (8–21) | 1.09 | 0.39 |
| FEV1/FVC < 70% and DLCO < LLN and TLC > ULN | 95 (90–98) | 21 (14–30) | 1.21 | 0.24 |
| FEV1/FVC < 70% and DLCO < LLN and RV > ULN and TLC > ULN | 95 (90–98) | 21 (14–30) | 1.21 | 0.24 |
| FEV1/FVC < 70% and FEF25–75 < LLN and DLCO < LLN and RV > ULN and TLC > ULN | 97 (92–99) | 13 (8–21) | 1.11 | 0.26 |
© 2011 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Hesselbacher, S.E.; Ross, R.; Schabath, M.B.; Smith, E.O.; Perusich, S.; Barrow, N.; Smithwick, P.; Mammen, M.J.; Coxson, H.; Krowchuk, N.; et al. Cross-Sectional Analysis of the Utility of Pulmonary Function Tests in Predicting Emphysema in Ever-Smokers. Int. J. Environ. Res. Public Health 2011, 8, 1324-1340. https://doi.org/10.3390/ijerph8051324
Hesselbacher SE, Ross R, Schabath MB, Smith EO, Perusich S, Barrow N, Smithwick P, Mammen MJ, Coxson H, Krowchuk N, et al. Cross-Sectional Analysis of the Utility of Pulmonary Function Tests in Predicting Emphysema in Ever-Smokers. International Journal of Environmental Research and Public Health. 2011; 8(5):1324-1340. https://doi.org/10.3390/ijerph8051324
Chicago/Turabian StyleHesselbacher, Sean E., Robert Ross, Matthew B. Schabath, E. O’Brian Smith, Sarah Perusich, Nadia Barrow, Pamela Smithwick, Manoj J. Mammen, Harvey Coxson, Natasha Krowchuk, and et al. 2011. "Cross-Sectional Analysis of the Utility of Pulmonary Function Tests in Predicting Emphysema in Ever-Smokers" International Journal of Environmental Research and Public Health 8, no. 5: 1324-1340. https://doi.org/10.3390/ijerph8051324