
Abstract
Post-transplantation bronchiolitis obliterans syndrome (BOS) is a clinicopathological syndrome characterised histologically by obliterative bronchiolitis (OB) and physiologically by airflow limitation. It affects long-term survival with no consistently effective treatment strategy.
An updated review of risk factors for OB/BOS, and approaches to prevention and treatment was performed through a systematic review of relevant studies between January 1990 and February 2005. The initial search identified 853 publications, with 56 articles reviewed after exclusions. Early acute rejection is the most significant risk factor, with late rejection (≥3 months) also significant. Lymphocytic bronchitis/bronchiolitis is relevant, with later onset associated with greater risk. Viral infections are identified as significant risk factors. Human leukocyte antigen matching and OB/BOS development is a weaker association, but is stronger with acute rejection. Recipient and donor characteristics have a minor role. There is limited evidence that altering immunosuppression is effective in reducing the rate of decline in lung function.
BOS reflects an allo-immunological injury, possibly triggered by cytomegalovirus and respiratory viral infections, or noninfectious injury. Immunological susceptibility may be reflected by more frequent acute rejection episodes. Preventative and therapeutic modifications in immunosuppression remain important. Identifying markers of immunological susceptibility and, hence, risk stratification requires further research.
Similar content being viewed by others

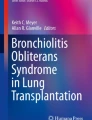
Obliterative bronchiolitis (OB) following lung transplantation is a histological diagnosis. It is defined by the presence of either an eccentric or, more commonly, concentric increase in fibrous tissue between the muscularis mucosa and the epithelium of membranous and proximal respiratory bronchioles, often in the form of fibrous plaques.[1] Figure 1 illustrates the pathological finding of more advanced OB where the bronchiole is occluded by cellular fibrous tissue. The aetiology and pathogenesis of OB appears to be multifactorial and may include repeated injury to the allograft by ischaemic-reperfusion injury, acute rejection, infection and other inflammatory reactions leading to airway epithelial tissue damage and loss. This then appears to be followed by an exaggerated healing response.[2] Risk factors for OB have been previously published by our group.[3] Diagnosis is usually based on a combination of clinical, radiological and functional markers. Bronchoscopy and transbronchial biopsy remain useful to exclude other abnormalities; however, this is an insensitive diagnostic test for this patchy histological process. The physiological surrogate bronchiolitis obliterans syndrome (BOS) has been defined[4] and recently revised[5] for use in clinical management and research, and is typified by progressive airflow obstruction. This staged definition has aided the study of risk factors and mechanisms for OB. However, attempts to modify these mechanisms, usually with augmented immunosuppression, has not significantly reduced the risk of developing of OB. It continues to result in reduced health-related quality of life[6] and a significant increase in the cost of care.[7] It remains the major cause of graft dysfunction with as many as 55% of affected individuals dying from this complication.[8,9] This paper presents an updated systematic review of the risk factors for OB and the current approaches to prevention and treatment.

Typical histological presentation of a bronchiole occluded by cellular fibrous tissue as seen in advanced obliterative bronchiolitis.
1. Literature Search
A systematic review was conducted using MEDLINE, EMBASE and the Cochrane Controlled Trials Register. The defined topic area used the terms obliterative bronchiolitis, bronchiolitis obliterans syndrome, and lung transpl*. Subsequent hand searching of identified journal articles and reviews was performed for the period January 1990 to February 2005. We excluded studies for the following reasons: non-human studies; publications prior to 1990; small (<25 patients) studies that were predominantly concerned with investigating the pathogenesis of OB; studies solely concerned with diagnosis of OB; and centre reports superceded by more recent studies. Onset of BOS, defined according to the unrevised international classification of lung dysfunction,[4] or OB, defined histologically, was the primary outcome of interest.
The initial search identified 853 publications. After exclusions, 56 articles were reviewed in detail.
2. Risk Factors
Almost all information on risk factors was derived from observational studies in single centres. Risk factors can be divided into immunological and non-immunological categories.
2.1 Immunological Risk Factors
2.1.1 Acute Rejection
Acute rejection is defined as a perivascular infiltration of mononuclear cells, including lymphocytes, into the graft, and classified according to internationally accepted criteria.[10] Acute rejection was the single most important risk factor for OB/BOS (table I). In the most recent reports from 15 transplant centres, 13[2,8,9,11–20] reported a significant association with acute rejection using a variety of clinical and histologically based definitions of acute rejection, and irrespective of whether or not both surveillance and symptomatic biopsies were included (table I). For two of these studies[13,14] the effect was only evident for later episodes. In lung transplantation, acute rejection frequently occurs beyond 3 months and a prolonged period of acute rejection post-transplantation may be an important marker for chronic problems.

Association between acute rejection and obliterative bronchiolitis (OB)
In the two studies that failed to demonstrate a significant association,[21,22] one involved only 22 cases of BOS and did not find a significant association despite a greater mean number of rejection episodes in the BOS group (4.33 vs 2.34[22]) and the other involved surveillance biopsies only, which alone may not be sufficiently sensitive to pick up associations, as the majority of these were low grade rejection.[21]
Further evidence of the role of acute rejection is provided by the association between BOS and decreased immunosuppression.[13] Ciclosporin (cyclosporin) levels were <200 ng/mL on two or more occasions in 21 of 66 BOS patients, compared with three of 68 non-BOS patients (p < 0.001). In the 21 BOS patients, immunosuppression was decreased for clinical reasons in 5 patients and was presumed to result from non-compliance in the remaining 16 patients. Regular reinforcement in the necessity of compliance remains important.[13]
2.1.2 Lymphocytic Bronchitis/Bronchiolitis
Non-fibrosing lymphocytic inflammation of the airways (lymphocytic bronchitis/bronchiolitis) has been seen in bronchial biopsies of lung transplant recipients and is thought to be a manifestation of acute rejection when other causes, particularly infection, have been excluded.[13] It has been associated with onset of OB/BOS,[2,11,13] with the strength of the relationship increasing over time following transplantation.[13] This may account for the lack of association reported by the Papworth group,[9] who only studied risk factors occurring in the first 6 months and did not perform surveillance biopsies beyond this time. In addition, there are difficulties in attributing histological appearances of lymphocytic bronchitis/bronchiolitis to acute rejection due to the frequent coexistence of infection and the variable presence of bronchioles, if any, in transbronchial biopsy samples.[9]
2.1.3 Human Leukocyte Antigen Mismatching
The association with mismatches at specific loci remains unclear. Some studies report no association.[11,13,23] In an analysis of 3549 lung transplants no significant association could be found between human leukocyte antigen (HLA) mismatching and development of OB, but there was a significant association with acute rejection.[23] In studies from single centres OB/BOS has been associated with fewer mismatches,[12] mismatches at the A locus,[2,14,19,24,25] two mismatches at the DR locus[18] and with total mismatches.[9,14,16,26] In general, studies that have demonstrated the detrimental effects of HLA mismatches have been based on large registries.[27] Single-centre studies have limited power due both to the small absolute effect of mismatching and to the lack of prospective tissue matching, resulting in few beneficial transplants.
2.2 Non-Immunological Risk Factors
2.2.1 Cytomegalovirus (CMV)
The impact of cytomegalovirus (CMV) is difficult to evaluate and may have varied with time, reflecting the relatively recent development of newer treatment protocols, including ganciclovir prophylaxis. A wide range of analyses and definitions were employed in the literature, making synthesis of the available evidence problematic. Newer screening technology, including quantitative polymerase chain reaction (PCR) viral analysis is currently evolving. Table II summarises the major relationships.

Association between markers of cytomegalovirus (CMV) and obliterative bronchiolitis
OB/BOS onset has been associated with CMV infection but only in a univariate analysis[9] or when expressed as a severity score.[11] Once BOS has developed there is some evidence that CMV infection confers greater risk of progressive disease.[17] There is more evidence of a link between CMV pneumonitis or disease and chronic lung dysfunction (table II). The CMV serological status of donor and recipients, particularly the implantation of a graft from a CMV positive donor into a negative recipient, has been considered a risk factor for BOS/OB, presumably as a surrogate for damage caused by introduction of the virus. However, serology has not proved a consistent risk factor (table II). The association between serological mismatching may have been attenuated by the increased use of ganciclovir prophylaxis.[29–32]
2.2.2 Non-CMV Infections
A small number of studies have implicated non-CMV pulmonary infections,[9] community respiratory viruses (particularly respiratory syncytial virus [RSV], parainfluenza virus [PIV] 3 and influenza A),[33] bacterial/fungal pneumonias, chlamydial infections[34,35] and Pneumocystis jiroveci (carinii)[11] in the pathogenesis of OB/BOS. A seasonal variation in the onset of OB/BOS has been described in lung transplant recipients, with a peak incidence in late winter correlating with the peak incidence of viral infection in the community.[33] It is possible that a low index of suspicion by clinicians results in infrequent utilisation of viral diagnostic assays to screen for these viruses. In one retrospective review of 122 patients following respiratory tract viral infection (RSV, PIV, influenza, adenovirus) OB/BOS occurred in 50% of patients who survived.[36] A recent review evaluating the effect of parainfluenza virus reported that 32% of the 22 patients with active infection subsequently developed OB during the following 18 months.[37] Treatment options include aerolised and intravenous ribavirin (a synthetic guanosine analogue and broad-spectrum antiviral agent), based on small case series and anecdotal cases.[36,38,39] A small case-control series demonstrated that ribavirin and high-dose corticosteroids in lung transplant recipients with RSV respiratory tract infection was more effective than corticosteroid therapy alone in improving rate of recovery in pulmonary function and reducing the rate of OB/BOS development.[39]
There was evidence that post-BOS onset infections were associated with a more rapid progression through BOS stages and to death.[9]
2.3 Other Risk Factors
Younger recipient age,[8,11,24] transplantation for primary pulmonary hypertension[14] and single lung transplantation[16] have been associated with OB/BOS. However, recipient characteristics have not been found to be risk factors in the over-riding majority of centres.
Older donor age, prolonged graft ischaemia time and their combination was significantly related to OB/BOS in an International Society for Heart and Lung Transplantation registry report of >5000 transplants,[40] with one study demonstrating increased BOS incidence in recipients where organs were from donors with traumatic brain injury as the cause of death.[15] Otherwise, donor characteristics appear to have little impact on the development of chronic allograft dysfunction or the development of OB.
Although considered an important factor in the development of OB, the definition of, and results from, studies of an ischaemic-reperfusion injury have varied, with some showing weak evidence of an association with OB[11,12,41] and others no association.[19,42] It has also been suggested that gastro-oesohageal reflux may predispose to allograft dysfunction,[43] although this requires further analysis.
Initial reports suggesting that bronchial arterial revascularisation might reduce the incidence[44,45] or postpone the development of OB[22] have not been substantiated.[46]
A positive response to panel reactive antibody (PRA) testing, defined by lymphocytotoxic antibody activity in ≥10% of cell panels, has been associated with BOS in Pittsburgh (PA, USA) [p = 0.007[12]] and St Louis (MO, USA).[24] A small study from Duke University (NC, USA) has demonstrated that new, post-transplant, anti-HLA antibodies detected by flow-PRA are associated with significantly increased BOS onset and progressive disease.[28] Two studies[47,48] demonstrated an association between anti-HLA class 1 antibodies and chronic decline in lung function, and showed that detection of these antibodies preceded BOS development.
A relationship between the presence of organising pneumonia on transbronchial biopsy and OB has been reported.[9,11,49]
3. Clinical Management
3.1 Prevention of Bronchiolitis Obliterans (OB)/Bronchiolitis Obliterans Syndrome (BOS)
Early detection remains critical, with both patient and physician vigilance being required. The diagnosis requires evidence of progressive airflow obstruction on pulmonary testing,[5] and the absence of other causes of airflow obstruction. Bronchoscopy and transbronchial biopsies allow the exclusion of anastomotic stricture, bronchomalacia, infection and acute rejection, which may present a similar clinical picture. The role of surveillance bronchoscopy and transbronchial biopsies remains controversial.
Traditionally, maintenance immunosuppression for lung transplant recipients has included ciclosporin, azathioprine and prednisolone. Tacrolimus has emerged as an effective alternative to ciclosporin and has been used for patients with recurrent acute rejection. However, there is no convincing evidence that it is more effective in preventing BOS. More recently, azathioprine has been replaced by mycophenolate mofetil (MMF) in many transplant centres either for all patients de novo or selectively for patients with recurrent/persistent acute rejection. Despite promising results in renal and cardiac transplant recipients, preliminary results from a randomised controlled trial in lung transplant recipients has failed to demonstrate a reduction of acute rejection episodes with MMF,[50] with the impact on BOS development pending. The Zurich group demonstrated that BOS incidence decreased over time following the introduction of ganciclovir prophylaxis and the replacement of azathioprine with MMF in 93 de novo recipients.[51]
In lung transplantation there are similarities between the pathophysiology of chronic obstructive pulmonary disease and BOS with an infiltration of CD8+ T cells, macrophages and neutrophils.[52] Inflammation of the airways can be a feature of BOS, but it remains apparent that it can be regarded as a steroid-resistant disease at both the clinical and molecular level. De Soyza et al.[53] provided some evidence that inhaled corticosteroids are useful in treating lymphocytic bronchiolitis in a group of 14 patients. However, a small randomised double-blind trial in 30 patients evaluated whether inhaled fluticasone propionate twice daily for 3 months reduced the incidence in BOS development: there was no evidence in this study of any beneficial effect.[52] Despite the well established role of high-dose intravenous and oral corticosteroids with acute allograft rejection there are no randomised trials to evaluate clinical effect, if any, in patients with OB/BOS.
Given that acute rejection appears to be the most important risk factor for OB/BOS, some centres use cytolytic induction therapy. Garrity et al.[54] studied 27 patients treated with daclizumab, a humanised monoclonal antibody, as induction therapy and compared them with 34 historical controls. Therapy with daclizumab resulted in a significant reduction in the incidence of acute rejection of grade A2 or worse. In a randomised controlled trial of anti-rejection induction therapy, Brock et al.[55] compared the monoclonal antibody muromonab-CD3 (OKT3), antithymocyte globulin (ATG) and daclizumab. The muromonab-CD3 group had more infection episodes early (2–12 months) following transplantation, but there were no significant differences between the three groups with acute rejection episodes or BOS onset. Similarly Barlow et al.[56] found ATG and muromonab-CD3 induction therapy to be equally effective in preventing biopsy-proven OB. Snell et al.[57] evaluated ATG with high-dose corticosteroids in ten patients, where nine patients demonstrated significant attenuation of the decline in lung function, with mean follow-up of 310 days.
There is evidence that CMV incidence has fallen since the introduction of ganciclovir prophylaxis.[30–32] As stated, the Zurich group reported a reduced BOS incidence with the introduction of ganciclovir prophylaxis and MMF.[51] Ganciclovir resistance has been associated with earlier BOS onset in one isolated study.[58] Addition of CMV hyperimmune globulin with prophylactic ganciclovir therapy has coincided with a reduced incidence of OB in a study of matched patients from non-overlapping time periods at Stanford (CA, USA).[59]
Up-regulation of major histocompatibility complex class II loci has been correlated with greater frequency and severity of graft dysfunction. HMG-CoA reductase inhibitors (statins) have been reported to inhibit the facultative expression of these molecules,[60] hence inhibition may alter this component of allogeneic graft injury. A recently published retrospective study from Pittsburgh (PA, USA) compared statin use with non-statin use in 200 lung transplant recipients. Statin use was associated with a significant reduction in the development of OB and high-grade BOS, and also a lower frequency of acute allograft rejection. Additional favourable effects included higher pulmonary function measurements, lower maintenance global immunosuppression, less frequent treatments with intensive immunosuppressives, lowered rate of lethal infections and neoplasms, and improved overall survival (91% vs 58% at 6 years).[61]
3.2 Treatment of OB/BOS
BOS treatment generally consists of either augmenting or adjusting immunosuppressive therapies. Immunosuppressive augmentation may involve azathioprine, corticosteroids, antilymphocyte antibody preparations and aerolised ciclosporin. Once BOS develops it rarely demonstrates full arrest with any of these therapies. However, there are no randomised double-blind trials involving these therapies, including high-dose corticosteroids, which most transplant units will empirically trial.
Aerolised ciclosporin has been used in small numbers of lung recipients with histologically active OB, with one group demonstrating stabilisation in five of seven cases.[62] A subsequent study has demonstrated a survival advantage in patients treated with aerolised ciclosporin.[63]
Immunosuppressive adjustments may include changing ciclosporin to either tacrolimus or sirolimus (rapamycin) and/or changing azathioprine to MMF. In a multicentre study, Klepetko et al.[64] demonstrated that patients who develop BOS while receiving ciclosporin are more likely to have stable lung function after changing to tacrolimus. Revell et al.[65] reported a reduced rate at which lung function declined in 11 patients given tacrolimus as rescue therapy. Roman et al.[66] reported on 12 patients who were switched to tacrolimus alone or tacrolimus and MMF, and the development of BOS. In all patients, lung function stabilised by 12 months after changing therapy. Cairn et al.[67] demonstrated that these improvements can last 12 months after switching. Fieguth et al.[68] reported on seven patients who developed BOS at a median of 165 days after transplantation and were switched to tacrolimus. All but one patient had improved lung function after switching therapy. The remaining patient died from infection-related respiratory failure. Conversely, Sarahrudi et al.[69] reported on 11 patients changed from ciclosporin to tacrolimus with the onset of BOS. There was no significant reduction in functional decline.[69] All of these studies have involved small numbers of patients and have lacked a concurrent control group. Such ‘before and after’ studies are to be treated with caution since they are inherently biased in favour of the ‘after’ therapy; that is, we do not know how many patients would have stabilised spontaneously.
Interestingly, a recent observational pilot study evaluated the macrolide azithromycin following the diagnosis of BOS stage 1.[70] This study was based upon reports demonstrating clinical improvement in patients with cystic fibrosis with maintenance azithromycin,[70] with the authors suggesting an immunomodulatory role. Maintenance azithromycin, with the continuation of each patient’s baseline immunosuppressive therapy, occurred for a mean of 13.7 weeks. Five of the six recipients demonstrated a significant improvement in pulmonary function (mean increase in forced expiratory volume in 1 second of 46%). No significant alteration in ciclosporin or tacrolimus concentrations occurred with the introduction of azithromycin. Verleden and Dupont[71] found similar effects in eight patients treated with azithromycin. Although limited by small sample sizes and lack of a placebo control group, these studies require further investigation. Similarly, a number of other therapies have been evaluated on small groups of patients and early reports of successful halting of functional declined remain to be confirmed in larger, controlled trials. These include cytolytic therapy,[72,73] photophoresis,[74] total lymphoid irradiation,[75] cyclophosphamide[76] and methotrexate.[77] Sirolimus is an additional agent currently being studied, on the basis of promising results in animal models that have demonstrated inhibition in airway obliteration and infiltration of the graft by macrophages.[78] Early experience of 12 patients with newly diagnosed BOS is promising.[79]
Retransplantation has been performed successfully in 145 patients with OB, but with reduced survival compared with first lung transplant.[80] Apart from the retransplant registry,[80] only a few series from single centres have been reported to date, with wide differences in reported survival.[81–84] Retransplantation continues to remain a viable therapeutic option in selected transplant recipients with BOS. However, with the chronic shortage of donor organs and an ever-increasing pool of potential recipients, retransplantation remains controversial and ethically challenging.
4. Conclusion
This review allows further insight into the complexity of OB/BOS pathogenesis. Developing an optimal strategy to prevent, detect and manage this condition will continue to require the coordinated approach of multiple centres internationally. Prevention strategies require ongoing focus in the four areas of immunotherapy induction, basic maintenance, adjuvant therapy and corticosteroid therapy. Induction immunotherapy developments require further evaluation in the use of humanised antibodies, specific targets (basiliximab, daclizumab) and lymphocyte depletion (ATG). Detection strategies continue to rely on the combination of clinical, radiological and functional findings, where bronchoscopy and transbronchial biopsy are essential diagnostic procedures to exclude other pathologies, including respiratory tract viruses. Management strategies require further investigation into not just these four areas of immunotherapy but into the anti-proliferative agent sirolimus, the antimetabolite agent MMF and recent derivatives (everolimus, mycophenolate sodium [ERL 080], FK 779 [MNA 279] and FK 778 [MNA 715]). Given the ongoing uncertainty over its role, clinical trials of corticosteroid immunotherapy are required, both from a monotherapeutic approach and as combination therapy.
Finally, most studies that do demonstrate a positive effect in the treatment of OB/BOS show only a limited response, which is to be expected given the typical histological finding of small airway fibrosis and the established damage that has already occurred when lung dysfunction is observed clinically. However, increasing and modifying the immunosuppressive regimen remains the first-line approach to therapy, including within our transplant centre. This immunosuppressive load requires a cautious approach as each recipient is at significantly increased risk of opportunistic infection, which may accelerate loss in lung function and be the cause of death.
References
Burke CM, Theodore J, Dawkins KD, et al. Post-transplant obliterative bronchiolitis and other late lung sequelae in human heart-lung transplantation. Chest 1984; 86: 824–9
El-Gamel A, Sim E, Hasleton P, et al. Transforming growth factor beta (TGF-β) and obliterative bronchiolitis following pulmonary transplantation. J Heart Lung Transplant 1999; 18: 828–37
Sharpies LD, McNeil K, Stewart S, et al. Risk factors for bronchiolitis obliterans: a systematic review of recent publications. J Heart Lung Transplant 2002; 21: 271–81
Cooper JD, Billingham M, Egan T, et al. A working formulation for the standardization of nomenclature and for clinical staging of chronic dysfunction in lung allografts. International Society for Heart and Lung Transplantation. J Heart Lung Transplant 1993; 12: 713–6
Estenne M, Maurer J, Boehler A, et al. Bronchiolitis obliterans syndrome 2001: an update of the diagnostic criteria. J Heart Lung Transplant 2002; 21: 297–310
van den Berg JW, Geertsma A, van der Bij W, et al. Bronchiolitis obliterans syndrome after lung transplantation and health-related quality of life. Am J Respir Crit Care Med 2000; 161: 1937–41
van den Berg JW, van Enckevort PJ, TenVergert EM, et al. Bronchiolitis obliterans syndrome and additional costs of lung transplantation. Chest 2000; 118: 1648–52
Keller C, Cagle P, Brown R, et al. Bronchiolitis obliterans in recipients of single, double and heart-lung transplantation. Chest 1995; 107: 973–80
Heng D, Sharpies L, McNeil K, et al. Bronchiolitis obliterans syndrome: incidence, natural history, prognosis, and risk factors. J Heart Lung Transplant 1998; 17: 1255–63
Yousem SA, Berry GJ, Cagle PT, et al. Revision of the 1990 working formulation for the classification of pulmonary allograft rejection: Lung Rejection Study Group. J Heart Lung Transplant 1996; 15: 1–15
Girgis RE, Tu I, Berry GJ, et al. Risk factors for the development of obliterative bronchiolitis after lung transplantation. J Heart Lung Transplant 1996; 15: 1200–8
Bando K, Paradis IL, Similo S, et al. Obliterative bronchiolitis after lung and heart-lung transplantation: an analysis of risk factors and management. J Thorac Cardiovasc Surg 1995; 110: 4–13
Husain AN, Siddiqui MT, Holmes EW, et al. Analysis of risk factors for the development of bronchiolitis obliterans syndrome. Am J Respir Crit Care Med 1999; 159: 829–33
Kroshus TJ, Kshettry VR, Savik K, et al. Risk factors for the development of bronchiolitis obliterans syndrome after lung transplantation. J Thorac Cardiovasc Surg 1997; 114: 195–202
Ciccone AM, Stewart KC, Meyers BF, et al. Does donor cause of death affect the outcome of lung transplantation? J Thorac Cardiovasc Surg 2002; 123: 429–434; discussion 434-6
Hadjiliadis D, Davis RD, Palmer SM. Is transplant operation important in determining posttransplant risk of bronchiolitis obliterans syndrome in lung transplant recipients? Chest 2002; 122: 1168–75
Fiser SM, Tribble CG, Long SM, et al. Ischemia-reperfusion injury after lung transplantation increases risk of late bronchiolitis obliterans syndrome. Ann Thorac Surg 2002; 73: 1041–1047; discussion 1047-8
van den Berg JW, Hepkema BG, Geertsma A, et al. Long-term outcome of lung transplantation is predicted by the number of HLA-DR mismatches. Transplantation 2001; 71: 368–73
Schulman LL, Weinberg AD, McGregor CC, et al. Influence of donor and recipient HLA locus mismatching on development of obliterative bronchiolitis after lung transplantation. Am J Respir Crit Care Med 2001; 163: 437–42
Hopkins PM, Aboyoun CL, Chhajed PN, et al. Association of minimal rejection in lung transplant recipients with obliterative bronchiolitis. Am J Respir Crit Care Med 2004; 170: 1022–6
Swanson SJ, Mentzer SJ, Reilly JJ, et al. Surveillance transbronchial lung biopsies: implication for survival after lung transplantation. J Thorac and Cardiovasc Surg 2000; 119: 27–38
Norgaard MA, Andersen CB, Pettersson G. Does bronchial artery revascularisation influence results concerning bronchiolitis obliterans syndrome and/or obliterative bronchiolitis after lung transplantation? Eur J Cardiothorac Surg 1998; 14: 311–8
Quantz MA, Bennett LE, Meyer DM, et al. Does human leukocyte antigen matching influence the outcome of lung transplantation? An analysis of 3,459 lung transplantations. J Heart Lung Transplant 2000; 19: 473–9
Sundaresan S, Mohanakumar T, Smith MA, et al. HLA-A locus mismatches and development of antibodies to HLA after lung transplantation correlate with the development of bronchiolitis obliterans syndrome. Transplantation 1998; 65(5): 648–53
Chalermskulrat W, Neuringer IP, Schmitz JL, et al. Human leukocyte antigen mismatches predispose to the severity of bronchiolitis obliterans syndrome after lung transplantation. Chest 2003; 123: 1825–31
Girnita AL, Duquesnoy R, Yousem SA, et al. HLA-specific antibodies are risk factors for lymphocytic bronchiolitis and chronic lung allograft dysfunction. Am J Transplant 2005; 5: 131–8
Opelz G, Wujciak T. The influence of HLA compatibility on graft survival after heart transplantation: the Collaborative Transplant Study [see comments]. N Engl J Med 1994; 330: 816–9
Palmer SM, Davis RD, Hadjiliadis D, et al. Development of an antibody specific to major histocompatibility antigens detectable by flow cytometry after lung transplant is associated with bronchiolitis obliterans syndrome. Transplantation 2002; 74: 799–804
Tamm M, Aboyoun CL, Chhajed PN, et al. Treated cytomegalovirus pneumonia is not associated with bronchiolitis obliterans syndrome. Am J Respir Crit Care Med 2004; 170: 1120–3
Duncan SR, Paradis IL, Yousem SA, et al. Sequelae of cytomegalovirus pulmonary infections in lung allograft recipients. Am Rev Resp Dis 1992; 146: 1419–25
Soghikian MV, Valentine VG, Berry GJ, et al. Impact of ganciclovir prophylaxis on heart-lung and lung transplant recipients. J Heart Lung Transplant 1996; 15: 881–7
Speich R, Thurnheer R, Gaspert A, et al. Efficacy and cost effectiveness of oral ganciclovir in the prevention of cytomegalovirus disease after lung transplantation. Transplantation 1999; 67: 315–20
Hohlfeld J, Neidermeyer J, Hamm H. Seasonal onset of bronchiolitis obliterans syndrome in lung transplant recipients. J Heart Lung Transplant 1996; 15: 888–94
Glanville AR, Gencay M, Tamm M, et al. Chlamydia pneumoniae infection after lung transplantation. J Heart Lung Transplant 2005; 24: 131–6
Kotsimbos TC, Snell GI, Levvey B, et al. Chlamydia pneumoniae serology in donors and recipients and the risk of bronchiolitis obliterans syndrome after lung transplantation. Transplantation 2005; 79: 269–75
Palmer SM, Henshaw NG, Howell DN, et al. Community respiratory viral infection in adult transplant recipients. Chest 1998; 113: 944–50
Vilchez RA, Dauber J, McCurry K, et al. Parainfluenza virus infection in adult lung transplant recipients: an emergent clinical syndrome with implications on allograft function. Am J Transplant 2003; 3: 116–20
Billings JL, Hertz MI, Savik K, et al. Respiratory viruses and chronic rejection in lung transplant recipients. J Heart Lung Transplant 2002; 21: 559–66
Scott AR, Morton JM, Plit M, et al. Intravenous ribavirin: effective therapy for respiratory syncytial virus (RSV) infection after lung transplantation [Abstract]. J Heart Lung Transplant 2003; 22: S192
Hosenpud JD, Bennett LE, Keck BM, et al. The Registry of the International Society for Heart and Lung Transplantation: seventeenth official report-2000. J Heart Lung Transplant 2000; 19: 909–31
Fiser SM, Kron IL, Long SM, et al. Influence of graft ischemic time on outcomes following lung transplantation. J Heart Lung Transplant 2001; 20: 1291–6
Fisher AJ, Wardle J, Dark JH, et al. Non-immune acute graft injury after lung transplantation and the risk of subsequent bronchiolitis obliterans syndrome (BOS). J Heart Lung Transplant 2002; 21: 1206–12
Palmer SM, Miralles AP, Howell DN, et al. Gastroesophageal reflux as a reversible cause of allograft dysfunction after lung transplantation. Chest 2000; 118: 1214–7
Baudet EM, Dromer C, Dubrez J, et al. Intermediate-term results after en-bloc double-lung transplantation with bronchial arterial revascularisation. J Thorac Cardiovasc Surg 1996; 112: 1292–9
Yacoub M, Al-Kttan KM, Tadjkarimi S, et al. Medium term results of direct bronchial arterial revascularisation using IMA for single lung transplantation (SLT) with direct revascularisation. Eur J Cardiothorac Surg 1997; 11: 1030–6
Daly RC, McGregor CGA, McDougall JC, et al. Bronchial artery revascularisation does not prevent bronchiolitis obliterans syndrome after lung transplantation [abstract]. Third International Congress on Lung Transplantation; 1998 Sep 10–11; Paris, 22
Smith MA, Sundaresan S, Mohanakuma T, et al. Effect of development of antibodies to HLA and cytomegalovirus mismatch on lung transplantation survival and development of bronchiolitis obliterans syndrome. J Thorac Cardiovasc Surg 1998; 116: 812–20
Jaramillo A, Smith MA, Phelan D, et al. Development of elisadetected anti-HLA antibodies precedes the development of bronchiolitis obliterans syndrome and correlates with progressive decline in pulmonary function after lung transplantation. Transplantation 1999; 67(8): 1155–61
Milne DS, Gascoigne AD, Ashcroft T, et al. Organizing pneumonia following pulmonary transplantation and the development of obliterative bronchiolitis. Transplantation 1994; 57: 1757–62
Corris P, Glanville A, McNeil K, et al. One year analysis of an ongoing international randomized study of mycophenolate mofetil (MMF) vs azathioprine (AZA) in lung transplantation. J Heart Lung Transplant 2001; 20: 149–50
Speich R, Boehler A, Zalunardo MP, et al. Improved results after lung transplantation: analysis of factors. Swiss Med Wkly 2001; 131: 238–45
Whitford H, Walters EH, Levvey B, et al. Addition of inhaled corticosteroids to systemic immunosuppression after lung transplantation: a double-blind, placebo-controlled trial. Transplantation 2002; 11: 1793–9
De Soyza A, Fisher AJ, Small T, et al. Inhaled corticosteroids and the treatment of lymphocytic bronchiolitis following lung transplantation. Am J Respir Crit Care Med 2001; 164: 1209–12
Garrity Jr ER, Villanueva J, Bhorade SM, et al. Low rate of acute lung allograft rejection after the use of daclizumab, an interleukin 2 receptor antibody. Transplantation 2001; 71: 773–7
Brock MV, Borja MC, Ferber L, et al. Induction therapy in lung transplantation: a prospective, controlled clinical trial comparing OKT3, anti-thymocyte globulin, and daclizumab. J Heart Lung Transplant 2001; 20: 1282–90
Barlow CW, Moon MR, Green GR, et al. Rabbit antithymocyte globulin versus OKT3 induction therapy after heart-lung and lung transplantation: effect on survival, rejection, infection, and obliterative bronchiolitis. Transpl Int 2001; 14: 234–9
Snell GI, Esmore DS, Williams TJ. Cytolytic therapy for the bronchiolitis obliterans syndrome complicating lung transplantation. Chest 1996; 109: 874–8
Kruger RM, Shannon WD, Arens MQ, et al. The impact of ganciclovir-resistant cytomegalovirus infection after lung transplantation. Transplantation 1999; 68: 1272–9
Valantine HA, Luikart H, Doyle R, et al. Impact of cytomegalovirus hyperimmune globulin on outcome after cardiothoracic transplantation: a comparative study of combined prophylaxis with CMV hyperimmune globulin plus ganciclovir versus ganciclovir alone. Transplantation 2001; 72: 1647–52
Kwak B, Mulhaupt F, Myit S, et al. Statins as a newly recognized type of immunomodulator. Nat Med 2000; 6: 1399–402
Johnson BA, Iacono AT, Zeevi A, et al. Statin use is associated with improved function and survival of lung allografts. Am J Respir Crit Care Med 2003; 167: 1271–8
Iacono AT, Keenan RJ, Duncan SR, et al. Aerosolized cyclosporine in lung recipients with refractory chronic rejection. Am J Respir Crit Care Med 1996; 153: 1451–5
Iacono AT, Corcoran TE, Griffith BP, et al. Aerosol cyclosporin therapy in lung transplant recipients with bronchiolitis obliterans. Eur Respir J 2004; 23: 384–90
Klepetko W, Estenne M, Glanville A, et al. A multicentre study to assess outcome following a switch in the primary immunosuppressant from cyclosporin (CYA) to tacrolimus (TAC) in lung recipients. J Heart Lung Transplant 2001; 20: 208
Revell MP, Lewis ME, Llewellyn-Jones CG, et al. Conservation of small-airway function by tacrolimus/cyclosporine conversion in the management of bronchiolitis obliterans following lung transplantation. J Heart Lung Transplant 2000; 19: 1219–23
Roman A, Bravo C, Monforte V, et al. Preliminary results of rescue therapy with tacrolimus and mycophenolate mofetil in lung transplanted patients with bronchiolitis obliterans. Transplant Proc 2002; 34: 146–7
Cairn J, Yek T, Banner NR, et al. Time-related changes in pulmonary function after conversion to tacrolimus in bronchiolitis obliterans syndrome. J Heart Lung Transplant 2003; 22: 50–7
Fieguth H, Krueger S, Wiedenmann D, et al. Tacrolimus for treatment of bronchiolitis obliterans syndrome after unilateral and bilateral lung transplantation. Transplant Proc 2002; 34(5): 1884
Sarahrudi K, Carretta A, Wisser W, et al. The value of switching from cyclosporine to tacrolimus in the treatment of refractory acute rejection and obliterative bronchiolitis after lung transplantation. Transplant Int 2002; 15: 24–8
Gerhardt SG, McDyer JF, Girgis RE, et al. Maintenance azithromycin therapy for bronchiolitis obliterans syndrome: results of a pilot study. Am J Respir Crit Care Med 2003; 168: 121–5
Verleden GM, Dupont LJ. Azithromycin therapy for patients with bronchiolitis obliterans syndrome after lung transplantation. Transplantation 2004; 77: 1465–7
Date H, Lynch JP, Sundaresan S, et al. The impact of cytolytic therapy on bronchiolitis obliterans syndrome. J Heart Lung Transplant 1998; 17: 869–75
Kesten S, Rajagopalan N, Maurer J. Cytolytic therapy for bronchiolitis obliterans syndrome following lung transplantation. Transplantation 1996; 61: 427–30
O’Hagan AR, Stillwell PC, Arroliga A, et al. Photophoresis in the treatment of refractory bronchiolitis obliterans complicating lung transplantation. Chest 1999; 115: 1459–62
Diamond DA, Michalski JM, Lynch JP, et al. Efficacy of total lymphoid irradiation for chronic allograft rejection following bilateral lung transplantation. Int J Radiat Oncol Biol Phys 1998; 41: 795–800
Verleden GM, Buyse B, Delcroix M, et al. Cyclophosphamide rescue therapy for chronic rejection after lung transplantation. J Heart Lung Transplant 1999; 18: 1139–42
Dusmet M, Maurer J, Winton T, et al. Methotrexate can halt the progression of bronchiolitis obliterans syndrome in lung transplant recipients. J Heart Lung Transplant 1996; 15: 948–54
Fahrni JA, Berry GJ, Morris RE, et al. Rapamycin inhibits development of obliterative airway disease in a murine heterotopic airway transplant model. Transplantation 1997; 63: 533–7
Chaill BC, Somerville KT, Crompton JA, et al. Early experience with sirolimus in lung transplant recipients with chronic allograft rejection. J Heart Lung Transplant 2003; 22: 169–76
Novick RJ, Stitt LW, Al-Kattan K, et al. Pulmonary retransplantation: predictors of graft function and survival in 230 patients: Pulmonary Retransplant Registry. Ann Thorac Surg 1998; 65: 227–34
Miller JD, Patterson GA. Retransplantation following isolated lung transplantation. Semin Thorac Cardiovasc Surg 1992; 4: 122–5
Schäfers H-J, Hausen B, Wahlers T, et al. Retransplantation of the lung: a single center experience. Eur J Cardiothorac Surg 1995; 9: 291–6
Wekerle T, Klepetko W, Wisser W, et al. Lung retransplantation: institutional report on a series of twenty patients. J Heart Lung Transplant 1996; 15: 182–9
Brugiére O, Thabut G, Castier Y, et al. Lung retransplantation for bronchiolitis obliterans syndrome: long-term followup in a series of 15 recipients. Chest 2003; 123: 1832–7
Acknowledgements
No grant, gift, equipment and/or drug support was received for the preparation of this review. The authors have no conflicts of interest that are directly relevant to the content of this review.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Scott, A.I.R., Sharples, L.D. & Stewart, S. Bronchiolitis Obliterans Syndrome. Drugs 65, 761–771 (2005). https://doi.org/10.2165/00003495-200565060-00004
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003495-200565060-00004