
Abstract
The ability to identify individuals who are susceptible to adverse drug reactions (ADRs) has the potential to reduce the personal and population costs of drug-related morbidity. Some individuals may show an increased susceptibility to certain ADRs through genetic polymorphisms that alter their responses to various drugs.
We wished to establish a methodology that would be acceptable to members of the general population and that would enable estimation of the risks that specific genetic factors confer on susceptibility to specific ADRs. Buccal swabs were selected as a minimally invasive method to obtain cells for DNA extraction. We wished to determine whether DNA of sufficient quantity and quality could be obtained to enable genotyping for two different polymorphic genes that code for enzymes that are widely involved in drug disposition.
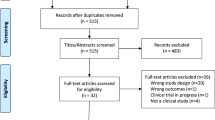
This article describes a small pilot study of methodology developed in the New Zealand Intensive Medicines Monitoring Programme (IMMP) to link prescription event monitoring (PEM) studies with pharmacogenetics. The methodology involves a nested case-control study design to investigate whether patients with genetic variants in P-glycoprotein (P-gp) and cytochrome P450 (CYP) 2C9 are more susceptible to psychiatric or visual disturbances following cyclooxygenase-2 inhibitor use (ADR signals identified in the IMMP database) than matched control patients taking the medication without experiencing any ADRs.
It was concluded that the use of buccal swabs is acceptable to patients and provides DNA of sufficient quantity and quality for genotyping. Although no differences in the distribution of genotypes in the case and control populations were found in this small study, case-control studies investigating genetic risks for ADRs using drug cohorts from PEM studies are possible, and there are several areas where population-based studies of genetic risk factors for ADRs are needed.
Examples are discussed where research in large populations is required urgently. These are: (i) genetic variations affecting P-gp function; (ii) variations affecting drugs metabolised by CYP2C9 and other polymorphic CYP enzymes; (iii) genetic variation in β-adrenergic receptors and adverse outcomes from β-adrenoceptor agonist therapy; and (iv) genetic variation in cardiac cell membrane potassium channels and their association with long QT syndromes and serious cardiac dysrhythmias.
Such studies will help to identify factors that increase the risk of unwanted outcomes from drug therapy. They will also help to establish in what circumstances genotyping should be performed prior to commencing drug treatment and in tailoring drug treatment for individual patients.



Similar content being viewed by others

References
McQueen EG. Intensified adverse drug reaction reporting scheme. N Z Med J 1977; 85(589): 477
Coulter DM. Signal generation in the New Zealand Intensive Medicines Monitoring Programme: a combined clinical and statistical approach. Drug Saf 2002; 25(6): 433–9
Inman WH. Postmarketing surveillance of adverse drug reactions in general practice. II: prescription-event monitoring at the University of Southampton. BMJ (Clin Res Ed) 1981; 282 (6271): 1216–7
Coulter DM. The New Zealand Intensive Medicines Monitoring Programme in pro-active safety surveillance. Pharmacoepidemiol Drug Saf 2000; 9: 273–80
Brazell C, Freeman A, Mosteller M. Maximizing the value of medicines by including pharmacogenetic research in drug development and surveillance. Br J Clin Pharmacol 2002; 53(3): 224–31
Aithal GP, Day CP, Kesteven PJ, et al. Association of polymorphisms in the cytochrome P450 CYP2C9 with warfarin dose requirement and risk of bleeding complications. Lancet 1999; 353(9154): 717–9
Drysdale CM, McGraw DW, Stack CB, et al. Complex promoter and coding region beta 2-adrenergic receptor haplotypes alter receptor expression and predict in vivo responsiveness. Proc Natl Acad Sci U S A 2000; 97(19): 10483–8
Israel E, Drazen JM, Liggett SB, et al. The effect of polymorphisms of the beta (2)-adrenergic receptor on the response to regular use of albuterol in asthma. Am J Respir Crit Care Med 2000; 162(1): 75–80
Higashi MK, Veenstra DL, Kondo LM, et al. Association between CYP2C9 genetic variants and anticoagulation-related outcomes during warfarin therapy. JAMA 2002; 287(13): 1690–8
Evans WE, McLeod HL. Pharmacogenomics: drug disposition, drug targets, and side effects. N Engl J Med 2003; 348(6): 538–49
Weinshilboum R. Inheritance and drug response. N Engl J Med 2003; 348(6): 529–37
Marzolini C, Paus E, Buclin T, et al. Polymorphisms in human MDR1 (P-glycoprotein): recent advances and clinical relevance. Clin Pharmacol Ther 2004; 75(1): 13–33
Clark D, Morgan A, Hananeia L, et al. Drug metabolism genotypes and their association with adverse drug reactions in selected populations: a pilot study of methodology. Drug Saf 2000; 9: 393–400
Coulter DM, Clark DW, Savage RL. Celecoxib, rofecoxib, and acute temporary visual impairment. BMJ 2003; 327(7425): 1214–5
Coulter DM. Acute psychiatric reactions with COX-2 inhibitors. Prescriber Update 2002; 23(2): 21
Schwab M, Eichelbaum M, Fromm MF. Genetic polymorphisms of the human MDR1 drug transporter. Annu Rev Pharmacol Toxicol 2003; 43: 285–307
Haefliger IO, Meyer P, Flammer J, et al. The vascular endothelium as a regulator of the ocular circulation: a new concept in ophthalmology? Surv Ophthalmol 1994; 39(2): 123–32
Clark DWJ, Layton D, Shakir SAW. Do some inhibitors of cyclooxygenase-2 (COX-2) increase the risk of thromboembolic events? Linking pharmacology with pharmacoepidemiology. Drug Saf 2004; 27(7): 427–56
Tang C, Shou M, Rushmore TH, et al. In-vitro metabolism of celecoxib, a cyclooxygenase-2 inhibitor, by allelic variant forms of human liver microsomal cytochrome P450 2C9: correlation with CYP2C9 genotype and in-vivo pharmacokinetics. Pharmacogenetics 2001; 11(3): 223–35
Miners JO, Birkett DJ. Cytochrome P4502C9: an enzyme of major importance in human drug metabolism. Br J Clin Pharmacol 1998; 45(6): 525–38
Brenner SS, Herrlinger C, Dilger K, et al. Influence of age and cytochrome P450 2C9 genotype on the steady-state disposition of diclofenac and celecoxib. Clin Pharmacokinet 2003; 42(3): 283–92
Martin JH, Begg EJ, Kennedy MA, et al. Is cytochrome P450 2C9 genotype associated with NSAID gastric ulceration? Br J Clin Pharmacol 2001; 51(6): 627–30
Roberts RL, Joyce PR, Mulder RT, et al. A common P-glycoprotein polymorphism is associated with nortriptyline-induced postural hypotension in patients treated for major depression. Pharmacogenomics J 2002; 2(3): 191–6
Richards B, Skoletsky J, Shuber AP, et al. Multiplex PCR amplification from the CFTR gene using DNA prepared from buccal brushes/swabs. Hum Mol Genet 1993; 2(2): 159–63
Daly AK, Day CP. Candidate gene case-control association studies: advantages and potential pitfalls. Br J Clin Pharmacol 2001; 52(5): 489–99
Tang K, Ngoi SM, Gwee PC, et al. Distinct haplotype profiles and strong linkage disequilibrium at the MDR1 multidrug transporter gene locus in three ethnic Asian populations. Pharmacogenetics 2002; 12(6): 437–50
Kroetz DL, Pauli-Magnus C, Hodges LM, et al. Sequence diversity and haplotype structure in the human ABCB1 (MDR1, multidrug resistance transporter) gene. Pharmacogenetics 2003; 13 (8): 481–94
Tucker G. Pharmacogenetics: expectations and reality. BMJ 2004; 329(7456): 4–6
Brinkmann U, Roots I, Eichelbaum M. Pharmacogenetics of the human drug-transporter gene MDR1: impact of polymorphisms on pharmacotherapy. Drug Discov Today 2001; 6(16): 835–9
Seelig A. A general pattern for substrate recognition by Pglycoprotein. Eur J Biochem 1998; 251(1-2): 252–61
Benet LZ, Izumi T, Zhang Y, et al. Intestinal MDR transport proteins and P-450 enzymes as barriers to oral drug delivery. J Control Release 1999; 62(1-2): 25–31
Thiebaut F, Tsuruo T, Hamada H, et al. Cellular localization of the multidrug-resistance gene product P-glycoprotein in normal human tissues. Proc Natl Acad Sci U S A 1987; 84(21): 7735–8
Kerb R, Aynacioglu AS, Brockmoller J, et al. The predictive value of MDR1, CYP2C9, and CYP2C19 polymorphisms for phenytoin plasma levels. Pharmacogenomics J 2001; 1(3): 204–10
Greiner B, Eichelbaum M, Fritz P, et al. The role of intestinal Pglycoprotein in the interaction of digoxin and rifampin. J Clin Invest 1999; 104(2): 147–53
Cordon-Cardo C, O’Brien JP, Casals D, et al. Multidrug-resistance gene (P-glycoprotein) is expressed by endothelial cells at blood-brain barrier sites. Proc Natl Acad Sci U S A 1989; 86(2): 695–8
Schinkel AH, Wagenaar E, Mol CA, et al. P-glycoprotein in the blood-brain barrier of mice influences the brain penetration and pharmacological activity of many drugs. J Clin Invest 1996; 97(11): 2517–24
Sakaeda T, Nakamura T, Horinouchi M, et al. MDR1 genotyperelated pharmacokinetics of digoxin after single oral administration in healthy Japanese subjects. Pharm Res 2001; 18(10): 1400–4
Kim RB, Leake BF, Choo EF, et al. Identification of functionally variant MDR1 alleles among European Americans and African Americans. Clin Pharmacol Ther 2001; 70(2): 189–99
Fellay J, Marzolini C, Meaden ER, et al. Response to antiretroviral treatment in HIV-1-infected individuals with allelic variants of the multidrug resistance transporter 1: a pharmacogenetics study. Lancet 2002; 359(9300): 30–6
Kim RB, Wandel C, Leake B, et al. Interrelationship between substrates and inhibitors of human CYP3A and P-glycoprotein. Pharm Res 1999; 16(3): 408–14
Hoffmeyer S, Burk O, von Richter O, et al. Functional polymorphisms of the human multidrug-resistance gene: multiple sequence variations and correlation of one allele with Pglycoprotein expression and activity in vivo. Proc Natl Acad Sci U S A 2000; 97(7): 3473–8
Johne A, Kopke K, Gerloff T, et al. Modulation of steady-state kinetics of digoxin by haplotypes of the P-glycoprotein MDR1 gene. Clin Pharmacol Ther 2002; 72(5): 584–94
Morita N, Yasumori T, Nakayama K. Human MDR1 polymorphism: G2677T/A and C3435T have no effect on MDR1 transport activities. Biochem Pharmacol 2003; 65(11): 1843–52
Sekino K, Kubota T, Okada Y, et al. Effect of the single CYP2C9*3 allele on pharmacokinetics and pharmacodynamics of losartan in healthy Japanese subjects. Eur J Clin Pharmacol 2003; 59(8-9): 589–92
Soldner A, Benet LZ, Mutschler E, et al. Active transport of the angiotensin-II antagonist losartan and its main metabolite EXP 3174 across MDCK-MDR1 and caco-2 cell monolayers. Br J Pharmacol 2000; 129(6): 1235–43
Cvetkovic M, Leake B, Fromm MF, et al. OATP and P-glycoprotein transporters mediate the cellular uptake and excretion of fexofenadine. Drug Metab Dispos 1999; 27(8): 866–71
Uhr M, Steckler T, Yassouridis A, et al. Penetration of amitriptyline, but not of fluoxetine, into brain is enhanced in mice with blood-brain barrier deficiency due to mdr1a P-glycoprotein gene disruption. Neuropsychopharmacology 2000; 22(4): 380–7
Nebert DW, Gonzalez FJ. P450 genes: structure, evolution, and regulation. Annu Rev Biochem 1987; 56: 945–93
Bertilsson L, Dahl ML, Dalen P, et al. Molecular genetics of CYP2D6: clinical relevance with focus on psychotropic drugs. Br J Clin Pharmacol 2002; 53(2): 111–22
Goldstein JA, de Morais SM. Biochemistry and molecular biology of the human CYP2C subfamily. Pharmacogenetics 1994; 4(6): 285–99
Lasker JM, Wester MR, Aramsombatdee E, et al. Characterization of CYP2C19 and CYP2C9 from human liver: respective roles in microsomal tolbutamide, S-mephenytoin, and omeprazole hydroxylations. Arch Biochem Biophys 1998; 353(1): 16–28
Miners J. CYP2C9 polymorphism: impact on tolbutamide pharmacokinetics and response. Pharmacogenetics 2002; 12(2): 91–2
McCrea JB, Cribb A, Rushmore T, et al. Phenotypic and genotypic investigations of a healthy volunteer deficient in the conversion of losartan to its active metabolite E-3174. Clin Pharmacol Ther 1999; 65(3): 348–52
Goldstein JA. Clinical relevance of genetic polymorphisms in the human CYP2C subfamily. Br J Clin Pharmacol 2001; 52(4): 349–55
Gill HJ, Tjia JF, Kitteringham NR, et al. The effect of genetic polymorphisms in CYP2C9 on sulphamethoxazole N-hydroxylation. Pharmacogenetics 1999; 9(1): 43–53
Stubbins MJ, Harries LW, Smith G, et al. Genetic analysis of the human cytochrome P450 CYP2C9 locus. Pharmacogenetics 1996; 6(5): 429–39
Furuya H, Fernandez-Salguero P, Gregory W, et al. Genetic polymorphism of CYP2C9 and its effect on warfarin maintenance dose requirement in patients undergoing anticoagulation therapy. Pharmacogenetics 1995; 5(6): 389–92
Taylor DR, Drazen JM, Herbison GP, et al. Asthma exacerbations during long term beta agonist use: influence of beta (2) adrenoceptor polymorphism. Thorax 2000; 55(9): 762–7
Green SA, Rathz DA, Schuster AJ, et al. The Ile164 beta (2)-adrenoceptor polymorphism alters salmeterol exosite binding and conventional agonist coupling to G (s). Eur J Pharmacol 2001; 421(3): 141–7
Mann M, Chowdhury B, Sullivan E, et al. Serious asthma exacerbations in asthmatics treated with high-dose formoterol. Chest 2003; 124(1): 70–4
Lipworth BJ, Aziz I. Bronchodilator response to albuterol after regular formoterol and effects of acute corticosteroid administration. Chest 2000; 117(1): 156–62
Lipworth BJ. Airway subsensitivity with long-acting beta 2-agonists: is there cause for concern? Drug Saf 1997; 16(5): 295–308
Green SA, Turki J, Bejarano P, et al. Influence of beta 2-adrenergic receptor genotypes on signal transduction in human airway smooth muscle cells. Am J Respir Cell Mol Biol 1995; 13(1): 25–33
Liggett SB. Polymorphisms of the beta2-adrenergic receptor and asthma. Am J Respir Crit Care Med 1997; 156(4 Pt 2): S156–62
Liggett SB. Genetics of beta 2-adrenergic receptor variants in asthma. Clin Exp Allergy 1995; 25Suppl. 2: 89–94
Lima JJ, Thomason DB, Mohamed MH, et al. Impact of genetic polymorphisms of the beta2-adrenergic receptor on albuterol bronchodilator pharmacodynamics. Clin Pharmacol Ther 1999; 65(5): 519–25
Littlejohn MD, Taylor DR, Miller AL, et al. Determination of beta2-adrenergic receptor (ADRB2) haplotypes by a multiplexed polymerase chain reaction assay [abstract]. Hum Mutat 2002; 20(6): 479
Taylor DR, Kennedy MA. Genetic variation of the beta (2)-adrenoceptor: its functional and clinical importance in bronchial asthma. Am J Pharmacogenomics 2001; 1(3): 165–74
Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med 2004; 350(10): 1013–22
Escande D. Pharmacogenetics of cardiac K (+) channels. Eur J Pharmacol 2000; 410(2-3): 281–7
Guzey C, Spigset O. Genotyping of drug targets: a method to predict adverse drug reactions? Drug Saf 2002; 25(8): 553–60
Haddad PM, Anderson IM. Antipsychotic-related QTc prolongation, torsade de pointes and sudden death. Drugs 2002; 62(11): 1649–71
Hu S, Wang S, Gibson J, et al. Inhibition of delayed rectifier K+ channels by dexfenfluramine (Redux). J Pharmacol Exp Ther 1998; 287(2): 480–6
Davies M, Behr E, Carter N, et al. Methodology of the Drug-Induced Arrythmia Risk Evaluation (DARE) study [abstract]. Pharmacoepidemiol Drug Saf 2003; 12: S115
Acknowledgements
A generous grant from the New Zealand Pharmacy Education and Research Foundation has enabled us to undertake the experimental work described in this article. We are also grateful to Janelle Ashton for invaluable assistance with this study and to Deborah Layton and Andrew Boshier for further information on pharmacogenetic studies initiated in the Drug Safety Research Unit. Dr Kennedy is a Senior Research Fellow of the Health Research Council of New Zealand. Dr Roberts is the recipient of a Health Sciences Career Development Award of the University of Otago. The New Zealand Intensive Medicines Monitoring Programme (IMMP) has been supported financially by Medsafe of the NZ Ministry of Health and some pharmaceutical companies, in particular, Merck Research Laboratories, USA.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Clark, D.W.J., Donnelly, E., Coulter, D.M. et al. Linking Pharmacovigilance with Pharmacogenetics. Drug-Safety 27, 1171–1184 (2004). https://doi.org/10.2165/00002018-200427150-00002
Published:
Issue Date:
DOI: https://doi.org/10.2165/00002018-200427150-00002