





To the Editors:
In a recent article published in the European Respiratory Journal, Bont et al. 1 presented data on systemic cytokine responses in hospitalized ventilated and nonventilated infants with respiratory syncytial virus (RSV) bronchiolitis. Their main findings were a lower production of interferon-γ (IFN-γ) and elevated plasma levels of interleukin (IL)-8 in ventilated patients. They concluded from their data that a depressed lymphocyte function and elevated IL-8 plasma levels are markers of severe RSV bronchiolitis in infants requiring ventilation.
However, the median age in ventilated patients was significantly lower than in nonventilated patients (1 versus 4 months). Furthermore, eight out of 14 ventilated patients were prematurely born. From that point of view it is difficult to compare these different groups because IFN-γ response is age-related and increases after 2 months of age 2. Performing a recently developed technique we were able to investigate IFN-γ production in neonatal and adult lymphocytes directly at the single cell level by flow cytometry 3. The number of IFN-γ producing lymphocytes was strikingly lower in newborn and especially preterm infants, followed by a substantial increase in the first months of life (fig. 1⇓). Considering these data, the lower IFN-γ response in the group of ventilated infants was more age-dependent than disease-related. Additionally, it seems questionable whether a local RSV infection ofthe lung is able to suppress IFN-γ production in blood lymphocytes supraphysiologically stimulated with phytohaemagglutinin.

Flow cytomertic detection of intracytoplasmic interferon (IFN)-γ, synthesis among CD3 positive lymphocytes stimulated with phorbol 12-myristate 13-acetate and ionomycin after cell permeabilization with saponin. Representative cases illustrate the age dependent IFN-γ synthesis in lymphocytes. Only small amounts of IFN-γ producing lymphocytes were detectable in a) healthy preterm and b) term infants at birth. In an c) infant 4 months of age the number of IFN-γ producing lymphocytes increased and reached 40% of an d) adult. The right upper quadrant represents the per cent IFN-γ producing lymphocytes of the totla CD3 positive lymphocytes population: preterm infant: 2%; term infant: 6%; infant, 4 months: 14%; adult: 34%. Percentages in the right lower quadrant represent the cytokine negative lymphocytes.
The elevated IL-8 plasma levels described in ventilated infants as a marker of severe RSV bronchiolitis also needs further comment 1. Although the difference in IL-8 plasma levels between ventilated and nonventilated infants was reported to be significant it seems questionable whether this difference is clinically important. Indeed, ten out of 14 cytokine levels from ventilated infants fell in the range of nonventilated infants 1. In addition, in an experimental rat model it has been demonstrated that mechanical ventilation can stimulate local and systemic inflammatory reactions 4. Furthermore, IL-8 levels were found to be elevated in ventilated preterm infants who develop chronic lung disease 5, 6. These studies support the view that mechanical ventilation induces inflammation in newborn infants and could be responsible for elevated IL-8 plasma levels in the group of ventilated infants with RSV bronchiolitis, also 1. Bont et al. 1 argued that a period of 2–6 h between initiation of mechanical ventilation and blood sampling was too short for induction of inflammation. However, we could demonstrate a fast IL-8 synthesis in monocytes ex vivo after 1 h of stimulation followed by a peak after 3 h (fig. 2⇓). Thus, the influence of mechanical ventilation on IL-8 production in the group of ventilated infants with RSV bronchiolitis 1 cannot be excluded.

{kind=link}
{kind=link}
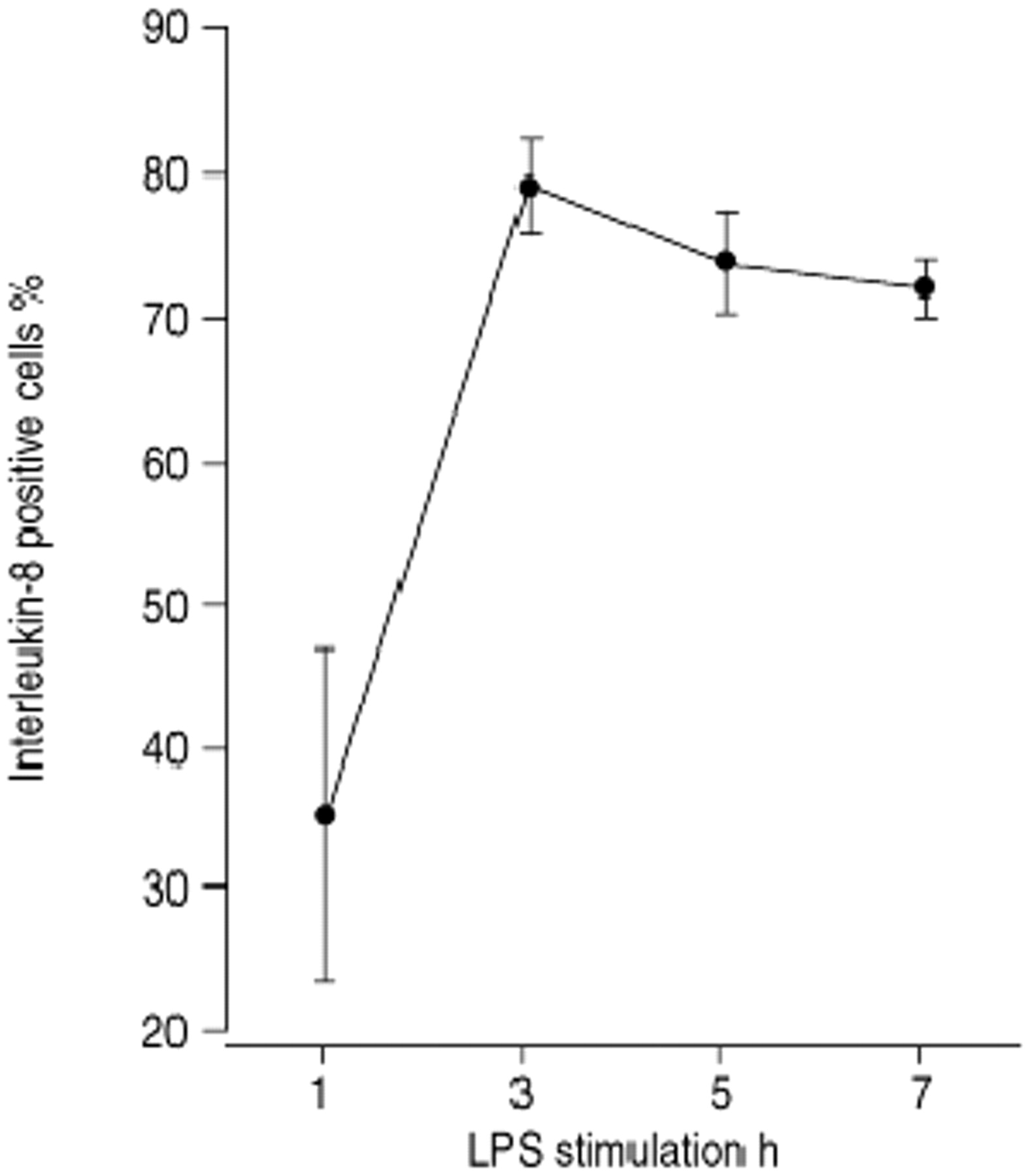
Kinetics of intracytoplasmic interleukin (IL)-8 synthesis in monocytes (n=5). IL-8 producing monocytes were already detectable 1 h after stimulation with lipopolysaccharide (LPS) in whole blood culture followed by a peak after 3 h. The amount of IL-8 producing monocytes is expressed as the percentage of the CD14 positive monocyte population analysed by flow cytometry at the single cell level according to a modified protocol 3. Bars refer to 1 sem.
Considering these data, we think that neither interferon-γ response or interleukin-8 plasma levels can be regarded as a marker of disease severity in respiratory syncytial virus bronchiolitis. It seems more likely that immune response maturation and mechanical ventilation were responsible for the differences between ventilated and nonventilated infants with respiratory syncytial virus bronchiolitis reported in the study by Bont et al. 1.
- © ERS Journals Ltd









