Article Text

Statistics from Altmetric.com
A 2.5 cm mass abutting the right hilum was found on an employment screening chest radiograph in a 31 year old asymptomatic man (fig 1). Chest CT scans with and without contrast showed a non-enhancing soft tissue mass with no fat or calcification (fig 2). T2 weighted MR images excluded a cystic fluid collection. At 6 month follow up a repeat CT scan showed a 4 mm increase in size and a right middle lobectomy was performed.
Grossly the lung section showed a firm tan well circumscribed mass 2.7 cm in diameter situated in the lung parenchyma without any connection to the pleura (fig 3). Microscopically the lesion was composed of abundant dense hyalinised collagen associated with a scant lymphoplasmacytic infiltrate and lymphoid aggregates, predominantly at the periphery. Foci of psammomatous (rounded, lamellar) and dystrophic calcification were distributed throughout the nodule (fig 4). Immunohistochemistry showed positive factor VIII staining of the fibroblasts, which were also negative for CD34, smooth muscle actin, muscle specific actin and desmin. There was no granulomatous inflammation or necrosis.
Calcifying fibrous pseudotumour (CFPT) is a rare benign lesion composed of hyalinised collagen with psammomatous/dystrophic calcification and a typical pattern of lymphocytic inflammation. This lesion usually occurs within soft tissues1 but has been described in the chest wall, pleura,2 and mediastinum. It has not previously been described in the lung. The pathogenesis is unclear but it has been suggested that these lesions are secondary to a benign inflammatory stimulus.
The differential diagnosis includes localised fibrous tumour of pleura, pulmonary hyalinising granuloma, calcifying granulomas, inflammatory (myofibroblastic) pseudotumour, and amyloidoma. These lesions can be differentiated from CFPT on the basis of conventional histopathology and immunohistochemistry. CFPT has a good prognosis with rare recurrences.2

PA chest radiograph showing a well circumscribed mass abutting the right hilum.

CT scan of the chest showing a sharply circumscribed homogenous soft tissue attenuation mass within the right middle lobe.
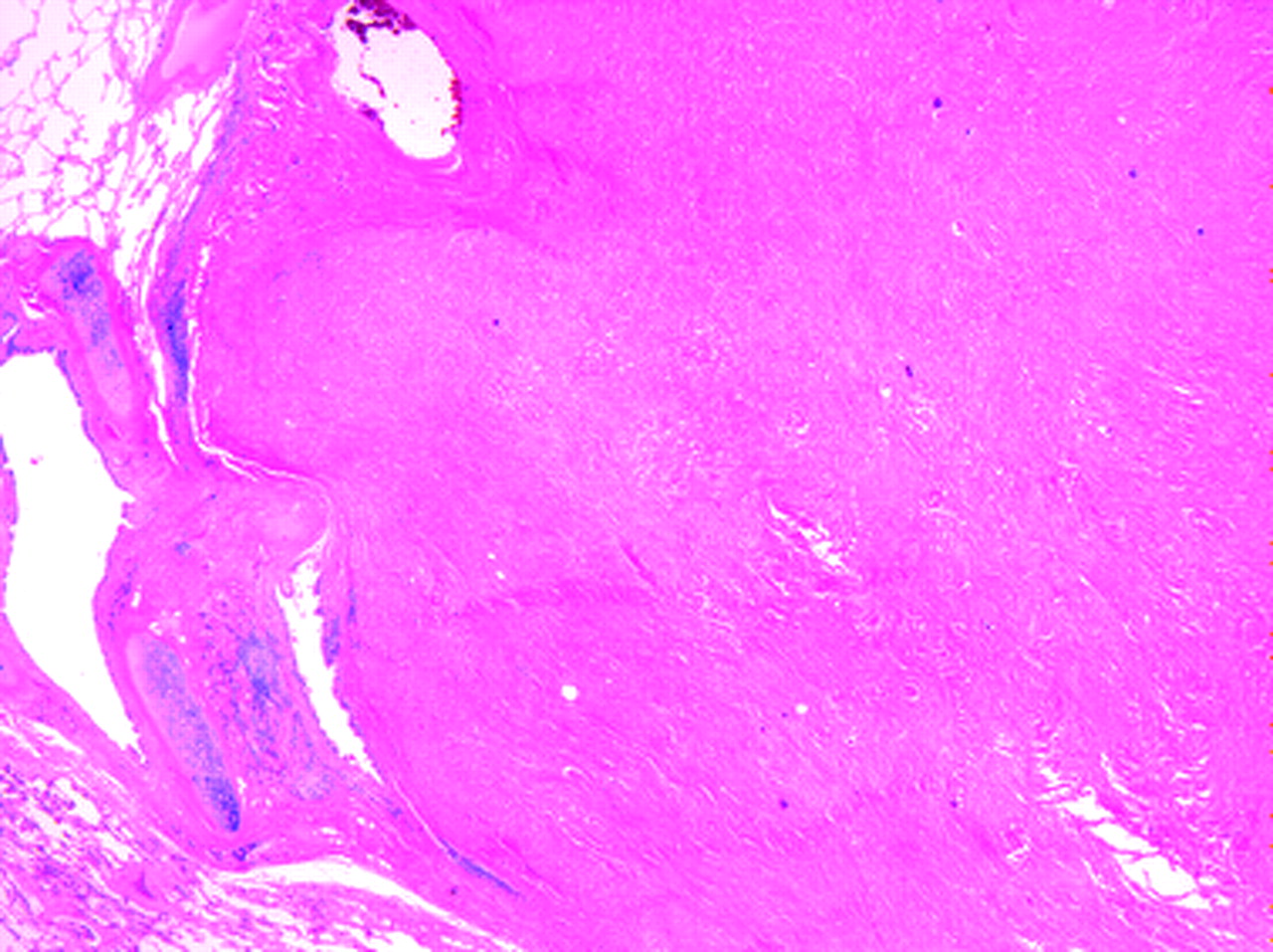
Low power photomicrograph showing a well circumscribed fibrous nodule within the lung parenchyma. It is juxtaposed to a bronchovascular structure but does not appear to originate directly from it (25× original magnification).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
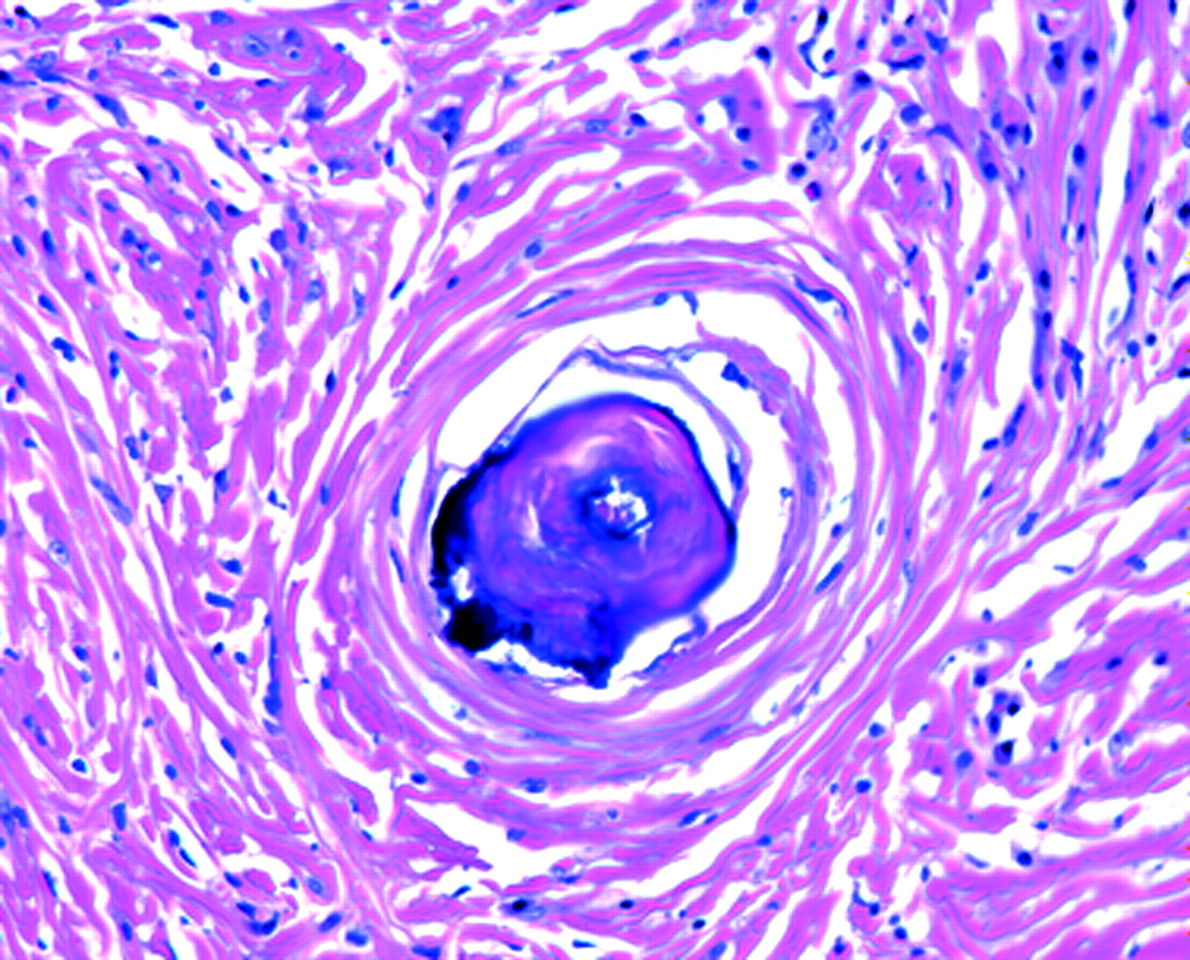
High power photomicrograph showing hyalinised dense collagen bundles, low cellularity, scattered lymphocytes, and psammomatous calcification (200× original magnification).