
Abstract
We examine the role of dendritic cells subsets in immunity to peripheral infections, with emphasis on the differences in the regulation of primary and secondary T cell responses to viruses. Our major focus is on new developments in the understanding of immunity to infections of the skin and lung, which are crucial entry points for a variety of infectious pathogens. Initially we describe a diverse network of dendritic cell subsets, but then we argue for a more generalized model of reduced complexity.
Similar content being viewed by others


Main
Ralph Steinman described dendritic cells (DCs), as they are now recognized, in the 1970s and showed that they are potent accessory cells involved in the induction (priming) phase of the immune response1,2. However, DCs were first observed in skin sections in the late 1800s by Paul Langerhans, who mistakenly identified them as a cell of neurological function3 (Fig. 1a). Once it was realized that Steinman's DCs were related to Langerhans cells (LCs)4, it was the latter that ultimately became the archetypal DCs. The progression of LCs through skin residence, antigen capture, migration, maturation and antigen presentation (Fig. 1b) was seen as the classic DC life cycle, a view more recently referred to as the “Langerhans cell paradigm”5. The original assessment of the importance of DCs in the initiation of immunity was not immediately accepted, as many immunologists held the view that macrophages or even B cells were the critical antigen-presenting cell. In the intervening years, however, numerous approaches have supported the idea of a key role for DCs in the priming phase of immunity. Interestingly, Hume recently questioned the demarcation between macrophages and DC6, and separately, basophils have been linked to the initiation of T helper type 2 immunity7,8,9, rekindling this dispute. On balance, however, the consensus has it that DCs are most probably a distinct population with unique T cell–stimulatory capacity.

Kim Caesar
(a) Staining of epidermal sheets for langerin (red) to identify LCs, for viral antigens (green) to identify HSV type 1, and cell nuclei (blue) on day 4 of infection just as the virus emerges from the nerve endings after replicating in the dorsal route ganglia113. (b) The Langerhans cell paradigm, in which cells spend the skin phase in antigen-capture mode, but after encountering pathogen, these DCs migrate to the draining lymph node and mature by upregulating costimulatory molecules and MHC class II–antigen complexes so they can activate naive T cells.
One of the best ways to define the role of DCs in the initiation of immunity has been to drive expression of the simian diphtheria toxin receptor (DTR) in mouse DCs under the control of the Cd11c promoter10,11. This allows depletion of DCs by injection of diphtheria toxin and was first used to link DCs to the priming of immunity to Listeria monocytogenes, to liver-stage malaria (Plasmodium yoelii) and to innocuous cross-presented antigen11. Many groups have subsequently extended this approach to their favorite antigen or organism, greatly boosting the case for DCs in the initiation of immunity12,13,14,15,16,17,18 and the generation of secondary responses19,20,21, although not with unanimous agreement22. One major caveat to this method is that a number of different cell types express CD11c, including natural killer cells, activated CD8+ T cells and some macrophages, which has made it difficult to definitively conclude DCs are responsible for immune initiation. In addition, in the case of L. monocytogenes, an alternative explanation may underlie the requirement for DCs, as this organism requires capture by DCs for replication in the spleen23. Similarly, DCs seem to be necessary for the infectivity of mouse mammary tumor virus24.
Another approach supporting the idea of a role for DCs in both immunity and tolerance induction has been the targeting of antigen to DCs via surface receptors such as CD205 (refs. 25,26, 27). When targeting approaches are combined with the CD11c-DTR depletion system12,28, an even stronger case for the essential role of DCs in immune initiation is evident. Once again, however, no receptor targeted so far is truly DC specific, which has left a modicum of doubt.
Many groups have shown DCs to be crucial antigen-presenting cells by isolating them directly from sites of immune induction (spleen or lymph node). Using allogeneic T cells as responders, Steinman originally used this approach to define the role for DCs in priming29. Although it is enticing, such ex vivo detection of antigen-presenting ability reflects the limits of technical capabilities of the time, and so it is possible that yet other cell types, which cannot be isolated, have an important role in priming. As an example, isolation of CD8α+ DCs30 was achieved many years after conclusions about the role of DCs in priming had been drawn with isolation techniques that would have failed to include this important population.
In the study of DC involvement in immune responses associated with the skin and other peripheral tissues, it is evident that in vivo depletion or ex vivo isolation techniques are the mainstay of the approaches used. The above discussion cautions that care be taken in interpreting data from these approaches, especially when techniques are used that further separate DCs into subpopulations.
DC subsets
The division of DCs into subsets was indicated in the 1970s when LCs were found to be different from splenic DCs, at least in their expression of Birbeck granules (made of langerin). But in those earlier times, this distinction was perhaps viewed more in terms of a precursor-product relationship, with those in lymphoid organs being simply a later stage of the LCs of the skin. In the mouse, decisive evidence for subset organization was provided by the subdivison of splenic DCs into CD8α− DCs and CD8α+ DCs30. This divide had been made earlier with CD205, DCIR2 and CD24 expression31 but was not clearly distinguished from a temporal developmental change. With the discovery of this splenic DC subdivision, Shortman's group began in earnest to assess precursor-product relationships, and several subsets were identified as distinct end stages32,33. The intricate description of DC subsets in the mouse paralleled the subdivision of human DCs into myeloid DCs and plasmacytoid DCs (pDCs)34.
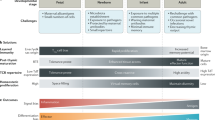
Stepping forward in time, quite a number of DC subsets that do not seem to be precursor-product related are now known (Fig. 2). The subdivision of DCs into myeloid DCs and pDCs seen in human is also seen in mice35,36,37 and seems to represent a major divide, with gene-expression analysis placing pDCs apart from other DCs38, which are now more often referred to as conventional DCs (cDCs). The role of pDCs in immunity is unclear and will not be discussed further here, but has been reviewed elsewhere39. Our view is that their key role is in innate immunity for the production of immune effector molecules such as interferon-α, although evidence for an antigen-presentation function is compelling39.

Kim Caesar
Key surface phenotype markers of DC subsets, categorized first on the basis of whether they are present in the steady state or only after inflammation (for example, infection). DN, CD4−CD8− (double-negative) DCs. The gut-associated DC subset that expresses CD103 and CD11b is not included separately, as this subset may simply be a member of the CD11b+ group. Also, monocytes have been reported to generate LCs, CD103+ DCs and CD11b+ DCs109,110,111,112, but this scheme draws attention to monocyte-derived DCs generated from monocytes rapidly recruited to inflammatory sites. The relationship between these inflammatory DCs and those in the steady state remains an open issue.
Leaving pDCs aside, cDCs can be categorized into three subsets in the spleen on the basis of their expression of CD4 and CD8α40 (Fig. 2). It is uncertain whether the bulk of the CD4−CD8− subset is distinct from the CD4+ subset, but several reports have found differences41,42, and studies of the uptake of 5-bromodeoxyuridine have found no major precursor-product relationship32. Unfortunately, a few precursors of CD8α+ DCs are contained in the CD4−CD8− subset43, which has muddied the waters of most studies in which splenic cDCs are simply categorized as CD8α+ cDCs and CD8α− cDCs.
The vast majority of splenic cDCs are derived from precursors that develop into DCs in the spleen44,45. These DCs reside in an immature state46 and probably perform the task of screening the blood for pathogens42,47,48. This review will not further address the function of DCs of the spleen but focuses on those DCs found in peripheral tissues and their draining lymph nodes. It is important to note, however, that DC subtypes found in the spleen also reside in lymph nodes, although CD4+ DCs are much rarer and the CD4−CD8− population is more prominent (Fig. 2). These lymph node–resident DCs may capture antigen from migratory DCs49,50,51 or from material draining directly through the lymphatic conduits52.
The true complexity of DC subsets becomes evident when we leave the spleen and enter secondary lymphoid tissues. The relatively simplistic view we held for some years was that only a single subset of DCs, which express CD11b and CD205, migrate from most organs, with the skin additionally containing LCs53. That view was clearly an oversimplification because numerous reports had described multiple DC subsets in organs such as the lung54,55 and gut56,57,58. However, it was difficult to separate developmental stages from distinct end stages, and without good reason to incorporate additional subsets into a global view of DCs, the simple model was preferred. The advent of the DTR system and the desire to better define the role of LCs in immunity and tolerance provided the impetus needed to raise the specter of additional tissue-associated DC subsets.
For many years, LCs were seen to fulfill the classic DC paradigm (Fig. 1b), but in 2003, evidence emerged that LCs are unable to generate CD8+ T cell immunity to herpes simplex virus type 1 (HSV-1) after infection of the skin epidermis59,60, precisely where LCs reside (Fig. 1a). Because LCs are radioresistant, unlike other DCs61, bone marrow chimeras can be generated in which LCs are the only DC type expressing the correct major histocompatibility complex (MHC) class I molecules to present viral antigen. The failure to detect primary HSV-specific cytotoxic T lymphocyte (CTL) responses in these conditions59 indicates that LCs are incapable of priming. In related studies examining the antigen-presenting cells that stimulate helper T cells after HSV-2 infection of the vaginal mucosa, questions were also raised about the role of LCs in viral immunity at epithelial sites62. Concurrent with doubts raised about the immunogenicity of LCs, cloning of the mouse langerin gene63 and description of the CD11c-DTR system11 left the ground fertile for the generation of a new series of tools to examine the now perplexing issue of LC function.
To study LC function, three groups developed mice that inducibly64,65 or constitutively66 lack langerin-expressing cells. In experiments using langerin-DTR mice, LCs were shown to be largely dispensable for hapten-mediated skin sensitization64. As a consequence, these animals provided further proof that LCs are unlikely to be the ubiquitous T cell primers that had long been accepted in the literature3, although hints of the priming capacity of LCs did emerge from these studies67,68. This evidence has been summarized elsewhere68. Notably, experiments with these animals also revealed an unappreciated complexity in the skin DC subpopulations, identifying a novel subset distinct from known LC and dermal DC populations.
When constructing their original langerin-DTR mice, Malissen and colleagues also used the gene knock-in approach to produce mice expressing enhanced green fluorescent protein (eGFP) under control of the endogenous langerin promoter64, which thus allowed tracking of langerin-positive cells in vivo by monitoring of eGFP. Although these mice nicely confirmed the existence of vast array of langerin-positive DCs in the skin epidermis, which matched the results of histological studies (Fig. 1a), they also highlighted the existence of a relatively small subset of langerin-positive DCs in the dermis. Like others before them, Malissen and colleagues regarded these langerin-positive DCs in the dermis as LCs en route to the draining lymph node. It was subsequently revealed, however, that these cells were a novel langerin-expressing DC that resides in the dermis69,70,71. These langerin-positive DCs were bone marrow derived and, in contrast to LCs, were radiosensitive69,70,71. They depended on the chemokine receptor CCR2, but not CCR6, to enter the skin, but like LCs used CCR7 to migrate to the draining node70. Painting of the skin with fluorescent agents and then monitoring of fluorescent cells in the draining lymph node directly demonstrated their migratory capacity69,72. The location of langerin-positive dermal DCs may be anatomically restricted, with one report hinting at a possible association with hair follicles and the potential for dendrites to reach through the basement membrane to the epidermis69. Extensive phenotypic characterization of the langerin-positive dermal DCs69 has shown that they are distinct from both LCs and classical dermal DCs, with low expression of CD11b and high expression of the integrin CD103 (αE)β7, the latter of which binds E-cadherin expressed by epithelial cells and by LCs themselves73,74. CD103 is also expressed on a number of other epithelium-associated cell types, including γδ T cells75, intraepithelial lymphocytes75 and tissue-resident memory αβ T cells76,77. Interestingly, earlier studies had reported CD103 expression on DCs in the lung and its draining nodes55, in the gut and draining lymphoid tissue56,57 and in lymph nodes draining nonmucosal sites such as the skin78.
Together the studies described above have established the existence of at least three different subpopulations of migratory DCs in the skin. We will refer to them here as LCs, dermal DCs and CD103+ DCs (Fig. 2). The last might best be called langerin-positive CD11b−CD103+ DCs, as low CD11b expression and high langerin expression are hallmarks of this population and CD103 is expressed by one other subset of DCs (discussed below). Unfortunately, it is probably best not to refer to CD103+ DCs as dermal DCs (as named by those who found them in the skin), as counterparts also reside in other sites. The lung contains at least two populations of DCs, including a CD103+ subset55,69 and a CD11b+ subset, the latter of which is probably a counterpart of the classical CD11b+ dermal DCs. In this review, for simplicity we will refer to cells as being CD11b+ or CD11b−, although it would be more accurate to define them as having high or low expression, as DCs are never completely negative. Mature progeny of the two lung-associated DCs populations are also found in the lung-draining mediastinal lymph node50,55,79. Like the CD103+ DCs in the dermis, those in the lung express langerin55,69, are CD11b− and can be depleted by treatment of langerin-DTR mice with diphtheria toxin55,79. CD11b− DCs, which probably match the CD103+ DCs found in the skin and lung-draining lymph nodes, are also seen in lymph nodes draining the liver and kidneys50, and langerin-positive DCs expressing CD103 are found in the liver69. Finally, langerin-expressing DCs can be identified in the muscular layer of the small intestine80, and CD11b−CD8α− DCs, which are probably CD103+ DCs, are found in the mesenteric lymph nodes and Peyer's patches81. It is worth noting that in addition to containing a small population of typical CD103+ DCs that lack expression of CD11b, the mesenteric lymph node contains a much larger population of CD11b+ CD103+ DCs (unpublished data). Expression of CD11b by this subset of CD103+ DCs suggests to us that they are not equivalent to the langerin-positive CD103+ population but are more like LCs or classical CD11b+ dermal DCs. Overall, the identification of counterparts of CD103+ DCs in lymph nodes draining the gut, liver, kidney, lungs and skin indicates that these DCs are widely distributed and not just skin associated.
The migratory CD103+ DCs and the lymphoid tissue–resident CD8α+ DCs bear many similarities, including expression of langerin, lack of CD11b, some antigen-presentation functions (discussed below), and their absence in mice deficient in the transcription factor Batf3 (ref. 82). It will be worthwhile to determine whether responses by regulatory T cells and CD8+ T cells induced by gut CD103+ DCs56,57,58 depend on Batf3.
Migratory DC subset function during infection
Extensive studies examining responses to lung-associated antigens have provided functional insight into the role of the CD103+ DC population. As mentioned above, DCs that seem to mirror both the skin-associated CD103+ DCs and the classical dermal DCs (CD11b+) have been described in the lung, with CD103+ DCs 'preferentially' located in the lung mucosa and vascular walls55. Examination of the types of DCs involved in antigen presentation after intranasal administration of noninfectious agents such as ovalbumin83 or inactivated virions84 has shown that CD103+ DCs are capable of cross-presentation, whereas migratory CD11b+ DCs are focused mainly on MHC class II–restricted presentation. Similarly, for viral infection of the respiratory tract, most studies have shown that CD103+ DCs are the main migratory subset presenting MHC class I–restricted antigens50,79,84,85, although a few reports have also observed MHC class I–restricted presentation by CD11b+ DCs84,85. Lymph node–resident CD8α+ DCs also contribute to CD8+ T cell activation during lung infection50,79,84,85 by a process that is potentially dependent on antigen handover from migratory DCs50. For viral infection, it is difficult to define whether DCs use cross-presentation or direct MHC I presentation (if infected). However, we speculate that migratory CD11b+ DCs, which do not cross-present innocuous antigens, require direct infection for MHC class I–restricted presentation of virus material. The corollary of this would be that both the migratory CD103+ DCs and the lymph node–resident CD8α+ DCs may rely on cross-presentation, as these subsets are known to cross-present innocuous antigens83,86. On this basis, agents able to infect DCs without causing rapid cell death or immunomodulation could be directly presented by any infected DCs, including the CD11b+ DC subset, but would be additionally cross-presented by DC subsets capable of this function. In contrast, only the CD103+ DCs and lymph node–resident CD8α+ DCs would present those more disabling viruses, and in this case presentation would be solely by cross-presentation (Fig. 3).

Kim Caesar
During viral infection, DCs may be infected (right side of diagram) or may capture virus particles or virus-infected cellular material (left side of diagram). Infected DCs may undergo apoptosis or lysis and become an antigen source for CD8α+ DCs or, if the virus is not highly destructive or immunomodulatory, they may survive and prime CD8+ T cells. DCs carrying viral material (lower left) will stimulate CD8+ T cells only if they are able to cross-present (CD103+ DCs) but may present antigen to CD4 T cells (CD11b+ DCs; not shown) or transfer it to lymph node–resident CD8α+ DCs for cross-presentation. The contribution of direct versus cross-presentation will depend on the dose of virus and its immunomodulatory and destructive capacity. Ag, antigen.
A scenario that parallels that in the lung is beginning to emerge for the presentation of virus and innocuous antigens by skin-associated DC subsets, although for this tissue, LCs add a layer of complexity that makes it more difficult to reach definitive conclusions. The introduction of several different viruses into the skin has elucidated a role for lymph node–resident CD8α+ DCs in CD8+ T cell immunity48,87,88,89. As seen for lung immune responses, for skin immunity, lymph node–resident CD8α+ DCs seem to obtain their viral antigens from migratory DCs51, although direct antigen drainage may contribute to this89. Such DC-to-DC transfer was originally indicated in experiments in which allogeneic DCs were injected directly into the skin and MHC class II–restricted presentation of alloantigen was monitored for recipient DCs in the lymph node49.
Several groups have observed presentation by skin-derived migratory DCs for various antigens, including viral components72,87,88,89, innocuous proteins90,91 and self components92,93. Subcutaneous injection of C57BL/6 mice with noncytopathic lentivirus vectors, in contrast to injection of other viruses such as HSV, vaccinia virus or influenza virus48,87,88,89, yields presentation mainly by migratory DCs87. The precise phenotype of these migratory DCs was not defined, but given that the virus was introduced subcutaneously, they are probably of dermal origin. Efficient presentation of lentiviral antigens by these migratory DCs might rely on the nonapoptotic nature of this vector, and this could underlie its lack of presentation by CD8α+ DCs, which efficiently capture apoptotic cells94. The dose of virus might also affect the contribution of migratory DCs, as even highly aggressive viruses that kill most DCs might allow a few live DCs to reach the lymph node and prime T cells. This could explain the variable antigen-presenting contribution by dermal DCs for subcutaneous infection with influenza virus48,88.
After subcutaneous infection with Leishmania major, a putatively migratory CD11b+ DC subset can present parasite antigens95,96. Subsequent studies have suggested that the CD11b+ DCs were not LCs and may have been nonmigratory lymph node–resident cells97,98,99, although some presentation by migratory DCs was indicated by labeling of the skin of infected mice with fluorescein isothiocyanate99. Recently, langerin+ cells were shown to be not required for the priming of CD4+ T cells, although langerin+ non-LCs did contribute to CD8+ T cell responses100. Whether these latter DCs were CD103+ DCs or CD8α+ DCs, which also express langerin64, was not determined.
Examination of the kinetics of MHC class I– and MHC class II–restricted presentation of HSV-1 antigens after epidermal infection of abraded skin has revealed two phases of presentation: one within 2 days of infection, draining the site of scarification, and a second starting 5 days after infection in the lymph node, draining the recrudescent zosteriform phase of disease72. This second phase occurs because HSV-1 also replicates in the dorsal route ganglia that innervates the scarification site and then, on day 3, egresses to the entire skin dermatome innervated by this ganglia. In this study, although lymph node–resident CD8α+ DCs dominated MHC class I–restricted presentation in the early phase, zosteriform infection resulted in a major contribution by CD103+ DCs to CD8+ T cell activation. For CD4+ T cell responses, classical CD11b+ dermal DCs were the dominant contributors (as previously demonstrated for HSV-2 infection of the vagina62), although strong presentation by CD103+ DCs and, to a lesser extent, CD8α+ DCs was evident. In this study, LCs showed no evidence of MHC class I–restricted presentation and minimal MHC class II–restricted presentation, which underlines their limited role in this infection. Although future studies are needed to define the relative contribution of CD8α+ DCs and CD103+ DCs to the generation of HSV-1-specific CTL immunity, the existing results suggest that for the migratory DC subsets, CD103+ DCs dominate MHC class I–restricted presentation72, whereas CD11b+ dermal DCs control MHC class II–restricted presentation62,72. The ability of CD103+ DCs to present viral antigen to CD8+ T cells probably relates to their ability to cross-present skin-associated antigens, as shown for ovalbumin expressed in the epidermis72. This parallels the cross-presentation ability reported for lung CD103+ DCs83. Thus, antigen presentation for the skin mirrors that in the lung, leaving epidermal LCs still unaccounted for. It is an ongoing and interesting challenge to define the function of this archetypal DC subset.
DC function in secondary T cell responses
Although a great deal of effort has been expended on defining the role of DCs in priming immunity or inducing tolerance, more recently their ability to initiate and maintain secondary responses has been analyzed. Lefrancois and colleagues first showed that DCs are required for secondary responses to viral infection by using the CD11c-DTR system to deplete DCs during the challenge phase20. Similar although less definitive results were provided by the use of bone marrow chimeras101, which also demonstrated that radioresistant LCs do not participate in stimulating memory HSV-1-specific CTL immunity to epidermal challenge. One study examining the presentation of viral antigens to memory CD8+ T cells after lung infection has shown that migratory CD11b− (CD103+) DCs stimulate poor memory CD8+ T cell proliferation relative to their efficient ability to stimulate naive responses102. This property has been reiterated for presentation of skin-derived ovalbumin93, an antigen now known to be cross-presented largely by CD103+ DCs72. These findings show that for tissue-associated antigens, migratory CD103+ DCs control naive CD8+ T cells responses but somewhat poorly reactivate memory. The basis for this difference in roles is unknown, but given the destructive nature of mucosal and epidermal responses mediated by CTLs (for example, contact hypersensitivity), we speculate that this is essential for limiting recurrent CTL responses to noninflammatory environmental antigens.
Unlike naive T cells, memory and effector cells can readily enter nonlymphoid tissues103, especially at sites of local inflammation, which provides possibilities for T cell–DC interactions directly in the periphery itself. Some recent investigations have examined DC stimulation in local sites of inflammation and have linked DCs to this process104,105,106,107. CD11b+ DCs can stimulate cytokine production by both regulatory and helper T cells in inflamed skin104, although the exact origin of these cells was left undefined. In addition, DCs have been linked to local T cell stimulation during influenza infection, in which they seem to promote T cell proliferation or survival directly in the lung105,106. McGill et al. used clodronate-based DC ablation to demonstrate that those DCs involved in local stimulation are a population recruited by the infection, but they were unable to identify the subset involved in this process105. These investigators excluded the possibility of involvement of CD103+ alveolar DCs because they failed to restore T cell proliferation when directly introduced into the lung, in line with the finding described above showing that CD103+ DCs are poor stimulators of secondary responses102. Aldridge et al. have indicated the involvement of a DC subset that produces tumor necrosis factor and inducible nitric oxide synthase (also known as TipDCs), a monocyte-derived population recruited from the blood106, which has generally been associated with the inflammatory process108. Monocyte-derived DCs can also promote secondary T cell population expansion in response to HSV-1 reactivation in sensory ganglia107, which suggests that such monocyte-derived DCs may have a general role in peripheral T cell stimulation. These inflammatory DCs represent a rapidly recruited antigen-presenting capacity that may differ from that of resident skin and mucosal DCs potentially also derived from monocytes109,110,111,112.
A minimalist view of DC subsets
Altogether the literature now supports the idea of the existence of a number of unique DC subsets, with an emerging realization that each is associated with distinct, although potential overlapping, functionalities. Here we would like to suggest the following four major subgroups: the pDCs; the CD11b+ DCs; the CD11b− DCs; and the monocyte-derived inflammatory DCs. Several DCs fall into the CD11b+ DC group, including the CD4+ and CD4−CD8− lymphoid tissue–resident DCs; the dermal CD11b+ DCs and their counterparts in the lung and other tissues; the LCs; and the CD11b+CD103+ DCs of the gut. The CD11b− DC group would include CD8α+ DCs of the lymphoid tissues and the CD103+ langerin-positive DCs of the skin, lungs and other tissues. These four groups could be generalized to have broad specializations, with pDCs promoting innate immunity; the CD11b+ DCs stimulating CD4+ T cell help, potentially focused on humoral immunity or responses to extracellular parasites; the CD11b− DCs being dedicated to priming cytotoxic T cell immunity and responses to cell-associated antigens; and the monocyte-derived inflammatory DCs controlling events directly in inflamed tissues, including antigen presentation at effector sites and the initiation of local secondary responses (Fig. 4). It was tempting to place LCs and the CD103+CD11b+ DCs into a fifth regulatory group, separate from other CD11b+ DCs, but in the interest of simplicity, we refrained.

Kim Caesar
Infection of the skin causes migration of the three skin-resident DCs populations to the draining node72, and associated inflammation at the infection site rapidly recruits monocytes that form DCs in the skin113. Migratory DCs activate T cells in the draining lymph node and provide a source of antigen for lymph node–resident CD8α+ DCs51. DC groups (bottom right) contribute as follows: (i) Adaptive immunity is boosted by innate signals from pDC in the lymph node114 (and potentially the skin). (ii) CD11b+ DCs, such as dermal DCs, and lymph node–resident CD4+ and double-negative DCs contribute to CD4+ T cell responses, whereas (iii) CD11b− DCs (CD103+ DCs and CD8α+ DCs) contribute to CD8+ T cell responses72. (iv) Monocyte-derived DCs act as local stimulators of effector or memory T cells recruited to the infection104,105,106,107. The role of LCs is still largely a mystery, although the possibilities of antigen transport and CD4+ T cell stimulation are not fully excluded.
We acknowledge that this is probably a gross oversimplification, with new subsets and new functionalities likely to be described over time. However, even this minimalist view is a long way from the 'one size fits all' model encapsulated by the Langerhans cell paradigm, in which all DCs have identical potential and identical function. Given the plethora of pathogens, their varied routes of entry into the body and their diverse characteristics, it is perhaps not that surprising that this network of professional antigen-presenting cells dedicated to controlling T cell immunity has had to diversify to cope with all contenders at all phases of the immune response.
References
Steinman, R.M. & Cohn, Z.A. Identification of a novel cell type in peripheral lymphoid organs of mice. I. Morphology, quantitation, tissue distribution. J. Exp. Med. 137, 1142–1162 (1973). Key paper describing DCs.
Steinman, R.M., Gutchinov, B., Witmer, M.D. & Nussenzweig, M.C. Dendritic cells are the principal stimulators of the primary mixed leukocyte reaction in mice. J. Exp. Med. 157, 613–627 (1983). Key paper shows DCs are the primary stimulatory population.
Romani, N., Holzmann, S., Tripp, C.H., Koch, F. & Stoitzner, P. Langerhans cells—dendritic cells of the epidermis. APMIS 111, 725–740 (2003).
Steinman, R.M. et al. Dendritic cells of the mouse: identification and characterization. J. Invest. Dermatol. 75, 14–16 (1980).
Wilson, N.S. & Villadangos, J.A. Lymphoid organ dendritic cells: beyond the langerhans cells paradigm. Immunol. Cell Biol. 82, 91–98 (2004).
Hume, D.A. Macrophages as APC and the dendritic cell myth. J. Immunol. 181, 5829–5835 (2008).
Sokol, C.L. et al. Basophils function as antigen-presenting cells for an allergen-induced T helper type 2 response. Nat. Immunol. 10, 713–720 (2009).
Yoshimoto, T. et al. Basophils contribute to TH2-IgE responses in vivo via IL-4 production and presentation of peptide–MHC class II complexes to CD4+ T cells. Nat. Immunol. 10, 706–712 (2009).
Perrigoue, J.G. et al. MHC class II–dependent basophil-CD4+ T cell interactions promote TH2 cytokine–dependent immunity. Nat. Immunol. 10, 697–705 (2009).
Saito, M. et al. Diphtheria toxin receptor-mediated conditional and targeted cell ablation in transgenic mice. Nat. Biotechnol. 19, 746–750 (2001).
Jung, S. et al. In vivo depletion of CD11c+ dendritic cells abrogates priming of CD8+ T cells by exogenous cell-associated antigens. Immunity 17, 211–220 (2002). Key paper describing DC ablation method using the DTR system. Showed that DCs are required for several types of immune responses.
Lahoud, M.H. et al. The C-type lectin Clec12A present on mouse and human dendritic cells can serve as a target for antigen delivery and enhancement of antibody responses. J. Immunol. 182, 7587–7594 (2009).
Probst, H.C., McCoy, K., Okazaki, T., Honjo, T. & van den Broek, M. Resting dendritic cells induce peripheral CD8+ T cell tolerance through PD-1 and CTLA-4. Nat. Immunol. 6, 280–286 (2005).
Scumpia, P.O. et al. CD11c+ dendritic cells are required for survival in murine polymicrobial sepsis. J. Immunol. 175, 3282–3286 (2005).
Tian, T., Woodworth, J., Skold, M. & Behar, S.M. In vivo depletion of CD11c+ cells delays the CD4+ T cell response to Mycobacterium tuberculosis and exacerbates the outcome of infection. J. Immunol. 175, 3268–3272 (2005).
Kassim, S.H., Rajasagi, N.K., Zhao, X., Chervenak, R. & Jennings, S.R. In vivo ablation of CD11c-positive dendritic cells increases susceptibility to herpes simplex virus type 1 infection and diminishes NK and T-cell responses. J. Virol. 80, 3985–3993 (2006).
Dai, J., Liu, B., Cua, D.J. & Li, Z. Essential roles of IL-12 and dendritic cells but not IL-23 and macrophages in lupus-like diseases initiated by cell surface HSP gp96. Eur. J. Immunol. 37, 706–715 (2007).
Dewalick, S. et al. Cutting edge: conventional dendritic cells are the critical APC required for the induction of experimental cerebral malaria. J. Immunol. 178, 6033–6037 (2007).
van Rijt, L.S. et al. In vivo depletion of lung CD11c+ dendritic cells during allergen challenge abrogates the characteristic features of asthma. J. Exp. Med. 201, 981–991 (2005).
Zammit, D.J., Cauley, L.S., Pham, Q.M. & Lefrancois, L. Dendritic cells maximize the memory CD8 T cell response to infection. Immunity 22, 561–570 (2005). Key paper showing that DCs are required for secondary responses.
de Jong, J.M. et al. Dendritic cells, but not macrophages or B cells, activate major histocompatibility complex class II-restricted CD4+ T cells upon immune-complex uptake in vivo. Immunology 119, 499–506 (2006).
Scandella, E. et al. Dendritic cell-independent B cell activation during acute virus infection: a role for early CCR7-driven B-T helper cell collaboration. J. Immunol. 178, 1468–1476 (2007).
Neuenhahn, M. et al. CD8α+ dendritic cells are required for efficient entry of Listeria monocytogenes into the spleen. Immunity 25, 619–630 (2006).
Courreges, M.C., Burzyn, D., Nepomnaschy, I., Piazzon, I. & Ross, S.R. Critical role of dendritic cells in mouse mammary tumor virus in vivo infection. J. Virol. 81, 3769–3777 (2007).
Bonifaz, L. et al. Efficient targeting of protein antigen to the dendritic cell receptor DEC-205 in the steady state leads to antigen presentation on major histocompatibility complex class I products and peripheral CD8+ T cell tolerance. J. Exp. Med. 196, 1627–1638 (2002).
Bonifaz, L.C. et al. In vivo targeting of antigens to maturing dendritic cells via the DEC-205 receptor improves T cell vaccination. J. Exp. Med. 199, 815–824 (2004).
Hawiger, D. et al. Dendritic cells induce peripheral T cell unresponsiveness under steady state conditions in vivo. J. Exp. Med. 194, 769–779 (2001).
Nchinda, G. et al. The efficacy of DNA vaccination is enhanced in mice by targeting the encoded protein to dendritic cells. J. Clin. Invest. 118, 1427–1436 (2008).
Steinman, R.M. & Witmer, M.D. Lymphoid dendritic cells are potent stimulators of the primary mixed leukocyte reaction in mice. Proc. Natl. Acad. Sci. USA 75, 5132–5136 (1978).
Vremec, D. et al. The surface phenotype of dendritic cells purified from mouse thymus and spleen: investigation of the CD8 expression by a subpopulation of dendritic cells. J. Exp. Med. 176, 47–58 (1992).
Crowley, M., Inaba, K., Witmer-Pack, M. & Steinman, R.M. The cell surface of mouse dendritic cells: FACS analyses of dendritic cells from different tissues including thymus. Cell. Immunol. 118, 108–125 (1989).
Kamath, A.T. et al. The development, maturation, and turnover rate of mouse spleen dendritic cell populations. J. Immunol. 165, 6762–6770 (2000).
Kamath, A.T., Henri, S., Battye, F., Tough, D.F. & Shortman, K. Developmental kinetics and lifespan of dendritic cells in mouse lymphoid organs. Blood 100, 1734–1741 (2002).
Grouard, G. et al. The enigmatic plasmacytoid T cells develop into dendritic cells with interleukin (IL)-3 and CD40-ligand. J. Exp. Med. 185, 1101–1111 (1997).
Asselin-Paturel, C. et al. Mouse type I IFN-producing cells are immature APCs with plasmacytoid morphology. Nat. Immunol. 2, 1144–1150 (2001).
O'Keeffe, M. et al. Mouse plasmacytoid cells: long-lived cells, heterogeneous in surface phenotype and function, that differentiate into CD8+ dendritic cells only after microbial stimulus. J. Exp. Med. 196, 1307–1319 (2002).
Nakano, H., Yanagita, M. & Gunn, M.D. CD11c+B220+Gr-1+ cells in mouse lymph nodes and spleen display characteristics of plasmacytoid dendritic cells. J. Exp. Med. 194, 1171–1178 (2001).
Robbins, S.H. et al. Novel insights into the relationships between dendritic cell subsets in human and mouse revealed by genome-wide expression profiling. Genome Biol. 9, R17 (2008).
Villadangos, J.A. & Young, L. Antigen-presentation properties of plasmacytoid dendritic cells. Immunity 29, 352–361 (2008).
Vremec, D., Pooley, J., Hochrein, H., Wu, L. & Shortman, K. CD4 and CD8 expression by dendritic cell subtypes in mouse thymus and spleen. J. Immunol. 164, 2978–2986 (2000).
Proietto, A.I. et al. Differential production of inflammatory chemokines by murine dendritic cell subsets. Immunobiology 209, 163–172 (2004).
Lundie, R.J. et al. Blood-stage Plasmodium infection induces CD8+ T lymphocytes to parasite-expressed antigens, largely regulated by CD8α+ dendritic cells. Proc. Natl. Acad. Sci. USA 105, 14509–14514 (2008).
Bedoui, S. et al. Characterization of an immediate splenic precursor of CD8+ dendritic cells capable of inducing antiviral T cell responses. J. Immunol. 182, 4200–4207 (2009).
Naik, S.H. et al. Intrasplenic steady-state dendritic cell precursors that are distinct from monocytes. Nat. Immunol. 7, 663–671 (2006).
Diao, J. et al. In situ replication of immediate dendritic cell (DC) precursors contributes to conventional DC homeostasis in lymphoid tissue. J. Immunol. 176, 7196–7206 (2006).
Wilson, N.S. et al. Most lymphoid organ dendritic cell types are phenotypically and functionally immature. Blood 102, 2187–2194 (2003).
Sponaas, A.M. et al. Malaria infection changes the ability of splenic dendritic cell populations to stimulate antigen-specific T cells. J. Exp. Med. 203, 1427–1433 (2006).
Belz, G.T. et al. Cutting edge: conventional CD8α+ dendritic cells are generally involved in priming CTL immunity to viruses. J. Immunol. 172, 1996–2000 (2004).
Inaba, K. et al. Efficient presentation of phagocytosed cellular fragments on the major histocompatibility complex class II products of dendritic cells. J. Exp. Med. 188, 2163–2173 (1998).
Belz, G.T. et al. Distinct migrating and nonmigrating dendritic cell populations are involved in MHC class I-restricted antigen presentation after lung infection with virus. Proc. Natl. Acad. Sci. USA 101, 8670–8675 (2004).
Allan, R.S. et al. Migratory dendritic cells transfer antigen to a lymph node-resident dendritic cell population for efficient CTL priming. Immunity 25, 153–162 (2006). Provided strong evidence for the handover of antigen from migratory to lymph node–resident DCs.
Sixt, M. et al. The conduit system transports soluble antigens from the afferent lymph to resident dendritic cells in the T cell area of the lymph node. Immunity 22, 19–29 (2005).
Henri, S. et al. The dendritic cell populations of mouse lymph nodes. J. Immunol. 167, 741–748 (2001).
Holt, P.G., Haining, S., Nelson, D.J. & Sedgwick, J.D. Origin and steady-state turnover of class II MHC-bearing dendritic cells in the epithelium of the conducting airways. J. Immunol. 153, 256–261 (1994).
Sung, S.S. et al. A major lung CD103 (αE)-β7 integrin-positive epithelial dendritic cell population expressing Langerin and tight junction proteins. J. Immunol. 176, 2161–2172 (2006). Showed that there are two subsets of lung DCs, one expressing CD103 and with low expression of CD11b and the other negative for CD103 and expressing CD11b.
Annacker, O. et al. Essential role for CD103 in the T cell-mediated regulation of experimental colitis. J. Exp. Med. 202, 1051–1061 (2005).
Johansson-Lindbom, B. et al. Functional specialization of gut CD103+ dendritic cells in the regulation of tissue-selective T cell homing. J. Exp. Med. 202, 1063–1073 (2005).
Jaensson, E. et al. Small intestinal CD103+ dendritic cells display unique functional properties that are conserved between mice and humans. J. Exp. Med. 205, 2139–2149 (2008).
Allan, R.S. et al. Epidermal viral immunity induced by CD8α+ dendritic cells but not by Langerhans cells. Science 301, 1925–1928 (2003). Key paper questioning the long-held view that LCs stimulate immunity to skin infections. Showed CTL immunity to HSV-1 is not induced by LCs.
van Lint, A. et al. Herpes simplex virus-specific CD8+ T cells can clear established lytic infections from skin and nerves and can partially limit the early spread of virus after cutaneous inoculation. J. Immunol. 172, 392–397 (2004).
Merad, M. et al. Langerhans cells renew in the skin throughout life under steady-state conditions. Nat. Immunol. 3, 1135–1141 (2002).
Zhao, X. et al. Vaginal submucosal dendritic cells, but not Langerhans cells, induce protective Th1 responses to herpes simplex virus-2. J. Exp. Med. 197, 153–162 (2003).
Valladeau, J. et al. Identification of mouse langerin/CD207 in Langerhans cells and some dendritic cells of lymphoid tissues. J. Immunol. 168, 782–792 (2002).
Kissenpfennig, A. et al. Dynamics and function of Langerhans cells in vivo dermal dendritic cells colonize lymph node areas distinct from slower migrating Langerhans cells. Immunity 22, 643–654 (2005). One of three key papers setting up models for LC ablation. Provided the first hint of a langerin-positive dermal DC and suggested that LCs are not required for contact hypersensitivity.
Bennett, C.L. et al. Inducible ablation of mouse Langerhans cells diminishes but fails to abrogate contact hypersensitivity. J. Cell Biol. 169, 569–576 (2005).
Kaplan, D.H., Jenison, M.C., Saeland, S., Shlomchik, W.D. & Shlomchik, M.J. Epidermal langerhans cell-deficient mice develop enhanced contact hypersensitivity. Immunity 23, 611–620 (2005).
Bennett, C.L., Noordegraaf, M., Martina, C.A. & Clausen, B.E. Langerhans cells are required for efficient presentation of topically applied hapten to T cells. J. Immunol. 179, 6830–6835 (2007).
Kaplan, D.H., Kissenpfennig, A. & Clausen, B.E. Insights into Langerhans cell function from Langerhans cell ablation models. Eur. J. Immunol. 38, 2369–2376 (2008).
Bursch, L.S. et al. Identification of a novel population of Langerin+ dendritic cells. J. Exp. Med. 204, 3147–3156 (2007). One of three key papers identifying langerin-positive CD103+CD11b− dermal DCs in the skin.
Poulin, L.F. et al. The dermis contains langerin+ dendritic cells that develop and function independently of epidermal Langerhans cells. J. Exp. Med. 204, 3119–3131 (2007). One of three key papers identifying langerin-positive CD103+CD11b− dermal DCs in the skin.
Ginhoux, F. et al. Blood-derived dermal langerin+ dendritic cells survey the skin in the steady state. J. Exp. Med. 204, 3133–3146 (2007). One of three key papers identifying langerin-positive CD103+CD11b− dermal DCs in the skin.
Bedoui, S. et al. Cross-presentation of viral and self antigens by skin-derived CD103+ dendritic cells. Nat. Immunol. 10, 488–495 (2009).Key paper showing that CD103+ DCs of the skin present viral antigens to CD8+ T cells and cross-present skin antigens. Also provided evidence that dermal CD11b+ DCs present mainly to CD4+ T cells.
Jakob, T., Brown, M.J. & Udey, M.C. Characterization of E-cadherin-containing junctions involving skin-derived dendritic cells. J. Invest. Dermatol. 112, 102–108 (1999).
Tang, A., Amagai, M., Granger, L.G., Stanley, J.R. & Udey, M.C. Adhesion of epidermal Langerhans cells to keratinocytes mediated by E-cadherin. Nature 361, 82–85 (1993).
Brenan, M. & Rees, D.J. Sequence analysis of rat integrin αE1 and αE2 subunits: tissue expression reveals phenotypic similarities between intraepithelial lymphocytes and dendritic cells in lymph. Eur. J. Immunol. 27, 3070–3079 (1997).
Gebhardt, T. et al. Memory T cells in nonlymphoid tissue that provide enhanced local immunity during infection with herpes simplex virus. Nat. Immunol. 10, 524–530 (2009). Key paper illustrating the existence of tissue-resident memory T cells.
Boyman, O., Conrad, C., Tonel, G., Gilliet, M. & Nestle, F.O. The pathogenic role of tissue-resident immune cells in psoriasis. Trends Immunol. 28, 51–57 (2007).
Kilshaw, P.J. Expression of the mucosal T cell integrin αM290β7 by a major subpopulation of dendritic cells in mice. Eur. J. Immunol. 23, 3365–3368 (1993).
GeurtsvanKessel, C.H. et al. Clearance of influenza virus from the lung depends on migratory langerin+CD11b− but not plasmacytoid dendritic cells. J. Exp. Med. 205, 1621–1634 (2008).
Flores-Langarica, A. et al. Network of dendritic cells within the muscular layer of the mouse intestine. Proc. Natl. Acad. Sci. USA 102, 19039–19044 (2005).
Iwasaki, A. & Kelsall, B.L. Unique functions of CD11b+, CD8α+, and double-negative Peyer's patch dendritic cells. J. Immunol. 166, 4884–4890 (2001).
Hildner, K. et al. Batf3 deficiency reveals a critical role for CD8α+ dendritic cells in cytotoxic T cell immunity. Science 322, 1097–1100 (2008).
del Rio, M.L., Rodriguez-Barbosa, J.I., Kremmer, E. & Forster, R. CD103− and CD103+ bronchial lymph node dendritic cells are specialized in presenting and cross-presenting innocuous antigen to CD4+ and CD8+ T cells. J. Immunol. 178, 6861–6866 (2007).
Kim, T.S. & Braciale, T.J. Respiratory dendritic cell subsets differ in their capacity to support the induction of virus-specific cytotoxic CD8+ T cell responses. PLoS One 4, e4204 (2009).
Lukens, M.V., Kruijsen, D., Coenjaerts, F.E., Kimpen, J.L. & van Bleek, G.M. Respiratory syncytial virus-induced activation and migration of respiratory dendritic cells and subsequent antigen presentation in the lung-draining lymph node. J. Virol. 83, 7235–7243 (2009).
den Haan, J.M., Lehar, S.M. & Bevan, M.J. CD8+ but not CD8− dendritic cells cross-prime cytotoxic T cells in vivo. J. Exp. Med. 192, 1685–1696 (2000).
He, Y., Zhang, J., Donahue, C. & Falo, L.D. Jr. Skin-derived dendritic cells induce potent CD8+ T cell immunity in recombinant lentivector-mediated genetic immunization. Immunity 24, 643–656 (2006).
Mount, A.M. et al. Multiple dendritic cell populations activate CD4+ T cells after viral stimulation. PLoS One 3, e1691 (2008).
Lee, H.K. et al. Differential roles of migratory and resident DCs in T cell priming after mucosal or skin HSV-1 infection. J. Exp. Med. 206, 359–370 (2009).
Itano, A.A. et al. Distinct dendritic cell populations sequentially present antigen to CD4 T cells and stimulate different aspects of cell-mediated immunity. Immunity 19, 47–57 (2003).
Allenspach, E.J., Lemos, M.P., Porrett, P.M., Turka, L.A. & Laufer, T.M. Migratory and lymphoid-resident dendritic cells cooperate to efficiently prime naive CD4 T cells. Immunity 29, 795–806 (2008).
Mayerova, D., Parke, E.A., Bursch, L.S., Odumade, O.A. & Hogquist, K.A. Langerhans cells activate naive self-antigen-specific CD8 T cells in the steady state. Immunity 21, 391–400 (2004).
Waithman, J. et al. Skin-derived dendritic cells can mediate deletional tolerance of class I-restricted self-reactive T cells. J. Immunol. 179, 4535–4541 (2007).
Iyoda, T. et al. The CD8+ dendritic cell subset selectively endocytoses dying cells in culture and in vivo. J. Exp. Med. 195, 1289–1302 (2002).
Filippi, C. et al. CD4+ T cell polarization in mice is modulated by strain-specific major histocompatibility complex-independent differences within dendritic cells. J. Exp. Med. 198, 201–209 (2003).
Iwasaki, A. The importance of CD11b+ dendritic cells in CD4+ T cell activation in vivo: with help from interleukin 1. J. Exp. Med. 198, 185–190 (2003).
Lemos, M.P., Esquivel, F., Scott, P. & Laufer, T.M. MHC class II expression restricted to CD8α+ and CD11b+ dendritic cells is sufficient for control of Leishmania major. J. Exp. Med. 199, 725–730 (2004).
Ritter, U., Meissner, A., Scheidig, C. & Korner, H. CD8α− and Langerin-negative dendritic cells, but not Langerhans cells, act as principal antigen-presenting cells in leishmaniasis. Eur. J. Immunol. 34, 1542–1550 (2004).
Iezzi, G. et al. Lymph node resident rather than skin-derived dendritic cells initiate specific T cell responses after Leishmania major infection. J. Immunol. 177, 1250–1256 (2006).
Brewig, N. et al. Priming of CD8+ and CD4+ T cells in experimental leishmaniasis is initiated by different dendritic cell subtypes. J. Immunol. 182, 774–783 (2009).
Belz, G.T. et al. Bone marrow-derived cells expand memory CD8+ T cells in response to viral infections of the lung and skin. Eur. J. Immunol. 36, 327–335 (2006).
Belz, G.T., Bedoui, S., Kupresanin, F., Carbone, F.R. & Heath, W.R. Minimal activation of memory CD8+ T cell by tissue-derived dendritic cells favors the stimulation of naive CD8+ T cells. Nat. Immunol. 8, 1060–1066 (2007).
von Andrian, U.H. & Mackay, C.R. T-cell function and migration. Two sides of the same coin. N. Engl. J. Med. 343, 1020–1034 (2000).
McLachlan, J.B., Catron, D.M., Moon, J.J. & Jenkins, M.K. Dendritic cell antigen presentation drives simultaneous cytokine production by effector and regulatory T cells in inflamed skin. Immunity 30, 277–288 (2009).
McGill, J., Van Rooijen, N. & Legge, K.L. Protective influenza-specific CD8 T cell responses require interactions with dendritic cells in the lungs. J. Exp. Med. 205, 1635–1646 (2008).
Aldridge, J.R. Jr. et al. TNF/iNOS-producing dendritic cells are the necessary evil of lethal influenza virus infection. Proc. Natl. Acad. Sci. USA 106, 5306–5311 (2009).
Wakim, L.M., Waithman, J., van Rooijen, N., Heath, W.R. & Carbone, F.R. Dendritic cell-induced memory T cell activation in nonlymphoid tissues. Science 319, 198–202 (2008). Showed that T cells can be activated in peripheral tissues and that monocyte-derived DCs are critical for secondary T cell activation.
Serbina, N.V., Salazar-Mather, T.P., Biron, C.A., Kuziel, W.A. & Pamer, E.G. TNF/iNOS-producing dendritic cells mediate innate immune defense against bacterial infection. Immunity 19, 59–70 (2003).
Tacke, F. & Randolph, G.J. Migratory fate and differentiation of blood monocyte subsets. Immunobiology 211, 609–618 (2006).
Ginhoux, F. et al. Langerhans cells arise from monocytes in vivo. Nat. Immunol. 7, 265–273 (2006).
Varol, C. et al. Monocytes give rise to mucosal, but not splenic, conventional dendritic cells. J. Exp. Med. 204, 171–180 (2007).
Jakubzick, C. et al. Blood monocyte subsets differentially give rise to CD103+ and CD103− pulmonary dendritic cell populations. J. Immunol. 180, 3019–3027 (2008).
Eidsmo, L. et al. Differential migration of epidermal and dermal dendritic cells during skin infection. J. Immunol. 182, 3165–3172 (2009).
Yoneyama, H. et al. Plasmacytoid DCs help lymph node DCs to induce anti-HSV CTLs. J. Exp. Med. 202, 425–435 (2005).
Acknowledgements
We thank K. Shortman, S. Bedoui and P. Stumbles for advice, and L. Eidsmo for the immunohistology in Figure 1a. Supported by the Australian Research Council (W.R.H.), the Howard Hughes Medical Institute (W.R.H.) and the National Health and Medical Research Council of Australia (W.R.H. and F.R.C.).
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Heath, W., Carbone, F. Dendritic cell subsets in primary and secondary T cell responses at body surfaces. Nat Immunol 10, 1237–1244 (2009). https://doi.org/10.1038/ni.1822
Published:
Issue Date:
DOI: https://doi.org/10.1038/ni.1822
This article is cited by
-
ADP-ribosylating adjuvant reveals plasticity in cDC1 cells that drive mucosal Th17 cell development and protection against influenza virus infection
Mucosal Immunology (2022)
-
Kidney dendritic cells: fundamental biology and functional roles in health and disease
Nature Reviews Nephrology (2020)
-
CD205-positive, Sepharose-induced peritoneal exudate cells: a new resource for DC research in the chicken
Veterinary Research Communications (2019)
-
Immunomodulatory capacity of the serotonin receptor 5-HT2B in a subset of human dendritic cells
Scientific Reports (2018)
-
Pandemic 2009 H1N1 Influenza Venus reporter virus reveals broad diversity of MHC class II-positive antigen-bearing cells following infection in vivo
Scientific Reports (2017)
