
Abstract
Coronary heart disease (CHD) is the leading cause of mortality in the industrialized world. Proper identication of individuals at risk for CHD is challenging. The Framingham Risk Score, the most widely accepted tool for quantifying 10-year risk, fails to identify a great proportion of future CHD. Because of the health and economic consequences of CHD, there is a need to develop better prognostic tools for primary prevention. Coronary artery calcium scoring, C-reactive protein measurement, and heart rate recovery and exercise tolerance during exercise stress test may be useful tools for better risk stratication of intermediate-risk patients.
Similar content being viewed by others

References and Recommended Reading
Thom T, Haase N, Rosamond W, et al.: Heart Disease and Stroke Statistics-2006 Update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2006, 113L:85–151.
•• Gluckman TJ, Baranowski B, Ashen MD, et al.: A practical and evidence-based approach to cardiovascular risk reduction. Arch Intern Med 2004, 164:1490–1500.This article summarizes a comprehensive approach to cardiovascular prevention in an ABC format (comprehensive summary using the alphabet as a mnemonic device helping doctors remember all aspects of cardiovascular risk reduction)
Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106:3143–3421.
Akosah KO, Schaper A, Cogbill C, et al.: Preventing myocardial infarction in the young adult in the first place: how do the National Cholesterol Education Panel III guidelines perform? J Am Coll Cardiol 2003, 41:1475–1479.
•• Nasir K, Michos E, Blumenthal R, et al.: Detection of high-risk young adults and women by coronary calcium and National Cholesterol Education Program Panel III Guidelines. J Am Coll Cardiol 2005, 46:1931–1936.This is one of the first studies to show that many people with advanced subclinical atherosclerosis do not qualify for aspirin or lipid-lowering therapy if one relies on traditional risk assessment
Witteman JC, Kannel WB, Wolf PA, et al.: Aortic calcified plaques and cardiovascular disease (the Framingham Study). Am J Cardiol 1990, 66:1060–1064.
Schoenhagen P, Halliburton SS, Stillman AE, et al.: Noninvasive imaging of coronary arteries: current and future role of multi-detector row CT. Radiology 2004, 232:7–17.
Fuster V, Fayad Z, Moreno P, et al.: Atherothrombosis and high risk plaque. J Am Coll Cardiol 2005, 46:1209–1218.
Arad Y, Spadaro LA, Goodman K, et al.: Predictive value of electron beam computed tomography of the coronary arteries. 19 month follow-up of 1171 asymptomatic subjects. Circulation 1996, 93:1951–1953.
Arad Y, Spadaro LA, Goodman K, et al.: Prediction of coronary events with electron beam computed tomography. J Am Coll Cardiol 2000, 36:1253–1260.
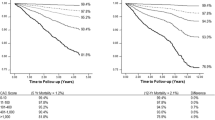
Shaw LJ, Raggi P, Schisterman E, et al.: Prognostic value of cardiac risk factors and coronary artery calcium screening for all-cause mortality. Radiology 2003, 228:826–833.
Kondos GT, Hoff JA, Sevrukov A, et al.: Electron-beam tomography coronary artery calcium and cardiac events. Circulation 2003, 107:2571–2576.
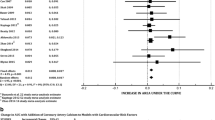
Greenland P, LaBree L, Azen SP, et al.: Coronary artery calcium score combined with framingham score for risk prediction in asymptomatic individuals. JAMA 2004, 291:210–215.
LaMonte MJ, FitzGerald SJ, Church TS, et al.: Coronary artery calcium score and coronary heart disease events in a large cohort of asymptomatic men and women. A J Epidemiol 2005, 162:421–429.
Taylor AJ, Bindeman J, Feuerstein I, et al.: Coronary calcium independently predicts incident premature coronary heart disease over measured cardiovascular risk factors. J Am Coll Cardiol 2005, 46:807–814.
Nasir K, Vasanreddy C, Blumenthal R, et al.: Comprehensive coronary risk determination in primary prevention: an imaging and clinical based definition combining computed tomographic artery calcium score and national cholesterol education program risk score. Int J Cardiol 2006, in press.
Shaw L, Raggi P, Berman D, et al.: Coronary artery calcium as a measure of biologic age. Atherosclerosis 2006, in press.
Redberg RF: Coronary artery calcium: should we rely on this surrogate marker? Circulation 2006, 113:336–337.
Raggi P, Davidson M, Callister TQ, et al.: Aggressive versus moderate lipid-lowering therapy in hypercholesterolemic postmenopausal women — beyond endorsed lipid lowering with EBT scanning (BELLES). Circulation 2005, 112:563–571.
Schmermund A, Achenbach S, Budde T, et al.: Effect of intensive versus standard lipid-lowering treatment with atorvastatin on the progression of calcified coronary atherosclerosis over 12 months. Circulation 2006, 113:427–437.
Wilson AM, Ryan AC, Boyle AJ. The novel role of C-reactive protein in cardiovascular disease: isk stratification or pathogen. Int J Cardiol 2006, 106:291–297.
Calabro P, Willerson JT, Yeh ET: Inflammatory cytokines stimulated C-reactive protein production by human coronary artery smooth muscle cells. Circulation 2003, 108:1930–1932.
Jabs WJ, Theissing E, Nitschke M, et al.: Local generation of C-reactive protein in diseased coronary artery venous bypass grafts and normal vascular tissue. Circulation 2003, 108:1428–1431.
Verma S, Wang CH, Li S, et al.: A self-fulfilling prophecy C-reactive protein attenuates nitric oxide production and inhibits angiogenesis. Circulation 2002, 106:913–919.
Bassuk S, Rifai N, Ridker PM: High sensitive C-reactive protein: clinical importance. Curr Probl Cardiol 2004, 29:439–493.
Danesh J, Whincup P, Walker M, et al.: Low grade inflammation and coronary heart disease prospective study and updated meta-analysis. BMJ 2000, 321:199–204.
Wilson P, Nam B, Pencina M, et al.: C-reactive protein and risk of cardiovascular disease in men and women from the Framingham Heart Study. Arch Intern Med 2005, 165:2473–2478.
Mora S, Ridker PM: Justification for the use of statins in primary prevention: an intervention trial evaluating rosuvastatin (JUPITER) — can C-reactive protein be used to target statin therapy in primary prevention? Am J Cardiol 2006, 97:33–41.
• Okin PM, Roman MJ, Best LG, et al.: C-reactive protein and electrocardiographic ST-segment depression additively predict mortality: the Strong Heart Study. J Am Coll Cardiol 2005, 45:1787–1793.This study shows a synergistic relationship between CRP and ST-segment changes
Khera A, De Lemos JA, Peshock RM, et al.: Relationship between C-reactive protein and subclinical atherosclerosis: Dallas Heart Study. Circulation 2006, 113:38–43.
Ridker PM, Cannon C, Morrow D, et al.: C-reactive protein levels and outcomes after statin therapy. N Engl J Med 2005, 352:20–28.
Fowler-Brown A, Pignone M, Pletcher M, et al.: Exercise tolerance testing to screen for coronary heart disease: a systematic review for the technical support for the US Preventive Services Task Force. Ann Intern Med 2004, 140: W9-W24.
Cole C, Blackstone EH, Pashkow F, et al.: Heart rate recovery immediately after exercise as a predictor of mortality. N Engl J Med 1999, 341:1351–1357.
Nishime E, Cole C, Blackstone E, et al.: Herat rate recovery and treadmill exercise store as predictors of mortality in patients referred for exercise ECG. JAMA 2000, 284:1392–1398.
•• Mora S, Redberg R, Sharrett R, et al.: Enhanced risk assessment in asymptomatic individuals with exercise testing and Framingham risk scores. Circulation 2005, 112:1566–1572. This study shows that exercise stress test parameters can be useful in the intermediate-risk population.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Thompson, J.B., Rivera, J.J., Blumenthal, R.S. et al. Primary prevention for patients with intermediate framingham Risk Scores. Curr Cardiol Rep 8, 261–266 (2006). https://doi.org/10.1007/s11886-006-0056-4
Issue Date:
DOI: https://doi.org/10.1007/s11886-006-0056-4