
Abstract
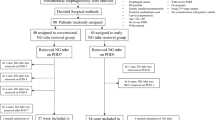
The aim of this study is to determine if the endoscopic presence of esophagitis predicts aspiration pneumonia after the initiation of enteral feedings in a newly placed PEG tube. A retrospective analysis of 278 patients who received a PEG tube from November 1999 to June 2002 was performed. All PEG procedures performed by a single endoscopist were reviewed from the GI Trac database at the Medical University of South Carolina. Eleven of the procedures were aborted due to technical difficulties. Nine patients received the PEG for gastric decompression only. Seven patients died within 14 days of PEG placement from non-PEG-related complications and were excluded. The resulting 251 patients included for our analysis successfully had PEG tube placement and had at least 14 days of enteral feeding. Esophagitis was defined macroscopically by the endoscopic presence of mucosal edema, friability, or obscurity of the normal vascular pattern in the distal esophagus. Aspiration was defined as the witnessed regurgitation of or tracheal suctioning of PEG feedings. Pneumonia as a consequence of aspiration was defined by development of fever and new infiltrate on chest radiograph within 14 days of PEG placement. Two hundred fifty-one patients had PEG placement (M, 127; F, 124; average age, 62.4 year; age range, 18–95 years) performed by a single endoscopist over a 32-month period. Fourteen (5.6%) of these patients had clinically evident pulmonary aspiration, with seven of them developing pneumonia. Thirteen (93%) of these patients had normal esophageal mucosa. One of the 24 patients (4%) with esophagitis or esophageal ulceration present endoscopically had an aspiration event with subsequent pneumonia. None of the 20 patients found to have some other form of esophageal pathology had an aspiration event. The overall incidence of aspiration pneumonia after the initiation of PEG feedings was 2.7% (7/251). The odds ratio that the presence of esophagitis would predict the development of aspiration pneumonia was 1.60, with a 95% confidence interval of 0.18 to 13.89. This study argues that the presence of esophagitis alone does not increase the risk of aspiration pneumonia from PEG feedings. Other factors apart from esophagitis play an important role in the incidence of aspiration pneumonia with PEG feeding.
Similar content being viewed by others


References
Gauderer MW, Ponsky JL, Iznant RJ: Gastrostomy without laparoscopy: A percutaneous endoscopic technique. J Pediatr Surg 15:872–875, 1980
Grant JP: Comparison of percutaneous endoscopic gastrostomy with Stamm gastrostomy. Ann Surg 207:598–603, 1988
Patel PH, Thomas E: Risk factors for pneumonia after percutaneous endoscopic gastrostomy. J Clin Gastroenterol 12:389–392, 1990
Cole MJ, Smith JT, Molnar C, et al.: Aspiration after percutaneous gastrostomy. J Clin Gastroenterol 9:90–95, 1987
Cogen R, Weinryb J: Aspiration pneumonia in nursing home patients fed via gastrostomy tubes. Am J Gastroenterol 84:1509–1512, 1989
Kadakia SC, Sullivan HO, Starnes E: Percutaneous endoscopic gastrostomy or jejunostomy and the incidence of aspiration in 79 patients. Am J Surg 164:114–118, 1992
Lien HC, Chang CS, Chen GH: Can percutaneous endoscopic jejunostomy prevent gastroesophageal reflux in patients with pre-existing esophagitis? Am J Gastroenterol 95:3439–3443, 2000
Larson DE, Burton D, Schroeder KW, et al.: Percutaneous endoscopic gastrostomy: Indications, success, complications, and mortality in 314 consecutive patients. Gastroenterology 93:48–52, 1987
Kaplan DS, Murthy UK, Linscher WG: Percutaneous endoscopic jejunostomy: Long-term follow up of 23 patients. Gastrointest Endosc 35:403–406, 1989
DiSario JA, Foutch PG, Sanowski RA: Poor results with percutaneous endoscopic jejunostomy. Gastrointest Endosc 36:257–260, 1990
Wolfsen HC, Kozarek RA, Ball TJ, et al.: Tube dysfunction following percutaneous gastrostomy and jejunostomy. Gastrointest Endosc 36:261–263, 1990
Henderson JM, Strodel WE, Gilinsky NH: Limitations of percutaneous endoscopic jejunostomy. JPEN 17:546, 1993
Huxley EJ, Viroslav J, Gray WR, et al.: Pharyngeal aspiration in normal adults and patients with depressed consciousness. Am J Med 64:564–568, 1978
DeLegge MH, Duckworth PF, McHenry L, et al.: Percutaneous endoscopic gastrojejunostomy: A dual center safety and efficacy trial. JPEN 19:239–243, 1995
McClave S, Chang WK: Complications of enteral access. Gastrointest Endosc 58:739–751, 2001
Finucane TE, Christmas C, Travis K: Tube feeding in patients with advanced dementia: a review of the evidence. JAMA 282:1365–1370, 1999
Kobayashi K, Cooper C, Clark A, et al.: A prospective evaluation of outcomes in patients referred for PEG placement. Gastrointest Endosc 55:500–506, 2001
Jarnagin WR, Duh Q-Y, Mulvihill SJ, et al.: The efficacy and limitations of percutaneous endoscopic gastrostomy. Arch Surg 127:261–264, 1992
Grant JP: Percutaneous endoscopic gastrostomy. Initial placement by single endoscopic technique and long term follow-up. Ann Surg 217:167–174, 1993
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Carnes, M.L., Sabol, D.A. & DeLegge, M. Does the Presence of Esophagitis Prior to PEG Placement Increase the Risk for Aspiration Pneumonia?. Dig Dis Sci 49, 1798–1802 (2004). https://doi.org/10.1007/s10620-004-9573-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-004-9573-4