
Abstract
The aims of this study were to determine whether caffeine administration increased respiratory muscle function and if this was associated with lung function improvement in prematurely born infants being weaned from mechanical ventilation. Respiratory muscle function was assessed by measurement of the maximum pressures generated during occlusions at end inspiration (Pemax) and end expiration (Pimax) and lung function by measurement of lung volume (functional residual capacity (FRC)) and respiratory system compliance (CRS) and resistance (RRS) in 18 infants with a median gestational age of 28 (range 24–36) weeks. Measurements were made immediately prior to caffeine administration (baseline) and 6 h later. Six hours after caffeine administration compared to baseline, the median Pemax (p = 0.017), Pimax (p = 0.004), FRC (p < 0.001), CRS (p = 0.002) and RRS (p = 0.004) had significantly improved. Our results suggest that caffeine administration facilitates weaning of prematurely born infants from mechanical ventilation by improving respiratory muscle strength.
Similar content being viewed by others

Introduction
Mechanical ventilation can be lifesaving in prematurely born infants, but prolonged ventilation is associated with complications, including an increased risk of nosocomial infection [24]. Hence, it is important to extubate infants as soon as possible, and a number of strategies and therapies have been used to facilitate weaning and extubation [9]. Meta-analysis of the results of randomised trials has demonstrated that methylxanthine administration facilitates extubation [11]. Both theophylline and caffeine have been used, but caffeine is now more commonly administered as it has a longer half life and is less toxic. In addition, in a randomised comparison [17], caffeine was demonstrated to have an earlier onset of action. Methylxanthines have a number of effects that could facilitate weaning including improving airway resistance [26] and compliance, although the latter has not been consistently reported [2]. Caffeine also has a diuretic effect, which may explain the improved lung compliance [26]. The improvement in compliance might also be explained by enhanced diaphragmatic activity, as in dogs, and caffeine administration was associated with improved contractility in both non-fatigued and fatigued diaphragms [25]. In a randomised study [13], aminophylline resulted in an increase (43%) in diaphragm excursions in infants. There, however, has been no quantitative assessment of the effect of caffeine administration on respiratory muscle strength in neonates. The aims, therefore, of this study were to test the hypothesis that caffeine administration would improve respiratory muscle strength in prematurely born infants being weaned from mechanical ventilation and this would be associated with improvements in lung function.
Materials and methods
Prematurely born, ventilated infants were eligible for entry into this study once their respiratory status had started to improve. Consecutive infants whose parents gave informed written consent were entered into the study, which was approved by the King’s College Hospital Research Ethics Committee. The infants all followed the neonatal unit’s standard weaning policy, that is, infants are weaned from mechanical ventilation by being transferred to patient-triggered ventilation. Within 1 h after switching to patient-triggered ventilation, sedation was stopped. Peak pressure was gradually reduced according to the blood gas monitoring results. Caffeine citrate was given in a loading dose of 20 mg/kg once the infant’s peak pressure had been reduced to below 20 cm H2O and a maintenance dose of caffeine citrate (5 mg/kg/24 h) was then given 24 h later. The inspiratory time and positive end expiratory pressure remained constant throughout the weaning process. All infants were ventilated via shouldered endotracheal tubes as per the neonatal unit’s routine policy [14]. Blood gases were assessed at four to six hourly intervals and reduction in peak pressure was made if the infant did not have a respiratory acidosis (pH < 7.25 with a raised PaCO2). Once a peak pressure of ≤14 cm H2O was reached and the inspired oxygen concentration (FiO2) was less than 0.40, the decision to extubate was made by the clinical team, who were unaware of the results of the respiratory muscle strength and lung function tests. The infant was then transferred on to endotracheal continuous positive airways pressure (CPAP) for a maximum of 1 h. If they did not develop a respiratory acidosis or desaturations, they were then extubated either into a head box containing the appropriate amount of supplementary oxygen or, if of birthweight less than 1,000 g, on to nasal CPAP. Nasal prong CPAP was instituted in infants of birthweight greater than 1.0 kg according to the routine policy, that is, if following extubation a respiratory acidosis or recurrent minor apnoeas developed. Extubation failure was diagnosed if infants of birthweight >1.0 kg required CPAP or any infant required reintubation within 48 h of extubation. Infants were reintubated if they had a major apnoea, developed a severe respiratory acidosis (pH < 7.20) or failed to improve despite instituting CPAP.
Immediately prior to administering the first dose of caffeine (baseline) and 6 h later, respiratory muscle strength, functional residual capacity (FRC), respiratory system compliance (CRS) and resistance (RRS) were measured. Airflow was recorded using a pneumotachograph (Mercury F10L; GM Engineering, Kilwinnning, UK) and differential pressure transducer (range ±2 cm H2O; MP45; Validyne Corporation, Northridge, CA, USA) inserted between the endotracheal tube and ventilator circuit manifold. Airway pressure was measured from a side port on the pneumotachograph using a differential pressure transducer (range ±100 cm H2O, MP45: Validyne Corporation). The signal from the pressure transducers was amplified (CD 280, Validyne) and displayed in real time on a personal computer (Dell Optiplex GX620, Dell Inc, UK) running Labview™ software (version 5.1, National Instruments, Austin, TX, USA), with analogue to digital sampling at 100 Hz (PCI-M10-16XE-50, National Instruments).
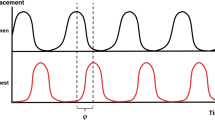
Respiratory muscle strength was assessed by measurements of the maximum inspiratory (Pimax) and expiratory (Pemax) pressures generated following airway occlusion while the infant was briefly disconnected from the ventilator. A two-way non-breathing valve was attached to the distal end of the pneumotachograph, and occlusion of the inspiratory limb of the valve allowed expiration but not inspiration, while occlusion of the expiratory limb allowed inspiration but not expiration. At least three sets of occlusions were performed to assess Pimax and Pemax. Occlusions were performed at least 5 min apart. Each occlusion was maintained until the infant had made at least five respiratory efforts. The timing of the occlusion was determined by observation of the infant’s respiratory movements. From the series of occlusions, the largest negative inspiratory (Pimax) and largest positive expiratory (Pemax) pressures generated were recorded. During the measurements, the infants were observed for episodes of chest wall distortion.
Lung volume was assessed by measurement of FRC using a helium gas dilution technique and a specially designed infant circuit (total volume 95 ml; Equilibrated Biosystems Inc, Series 7700, Melville, NY, USA). The circuit contained a rebreathing bag filled with a mixture of helium and oxygen enclosed in an airtight cylinder. The rebreathing bag was inserted into the ventilator circuit immediately above the endotracheal tube via a three-way valve. Actuation of the valve, at end expiration, connected the patient to the rebreathing bag and diverted the flow from ventilator to the airtight cylinder, thus maintaining mechanical ventilatory support. The change in helium concentration against time was displayed in real time on a flat panel display. During the measurement, if there was no change in the helium concentration over a 15-s period, equilibration was deemed to have occurred. The initial and equilibration helium concentrations were used in the calculation of FRC, which was corrected for oxygen consumption (assumed to be 7 ml/kg/min) [12] and to body temperature, pressure and water vapour-saturated conditions. FRC was measured twice and the results of the paired measurements averaged and related to body weight.
CRS and RRS were assessed using the single breath occlusion technique. The occlusions were performed using a pneumatic sliding valve (dead space 1.6 ml; 4285 series Hans Rudolph Inc, Kansas City, USA) connected to the distal end of the pneumotachograph inserted into the ventilator circuit. The pneumatic valve was arranged such that at end inspiration the infant could expire to room air (zero positive end expiratory pressure). The occlusion provoked the Hering Breuer reflex resulting in a temporary apnoea, as indicated by a plateau in the airway pressure trace. End inspiration was identified from the flow signal. Only occlusions with a pressure plateau of at least 100 ms were used in the calculation of CRS and RRS [10]; the mean CRS and RRS results from at least five such occlusions were calculated. CRS was related to body weight.
The nurses recorded hourly on observation charts, the ventilatory support received by the infant and the results of all blood gas monitoring. From the charts, the infant’s ventilatory requirements 6 h prior to receiving caffeine, at baseline and 6 h after caffeine had been given were determined.
Sample size
Recruitment of 18 infants allowed us to detect, with at least 80% power at the 5% level, a change in respiratory muscle function from baseline to 6 h after administration of caffeine equivalent to at least one standard deviation in the results of the measurements.
Analysis
The data were demonstrated not to be normally distributed using the Kolmogorov–Smirnov test. Differences, therefore, were assessed for statistical significance using a paired Wilcoxon rank sum test or Friedman test to correct for multiple comparison as appropriate. SPSS for Windows, version15 2007–2008 (SPSS Inc, Chicago IL, USA) was used.
Patients
Eighteen patients with a median gestational age of 28 (range 24–36) weeks and birthweight of 1,110 (range 730–2,975) g were studied at a median postnatal age of 6 (range 1–19) days. Sixteen infants had had respiratory distress syndrome and all but one had been exposed to two doses of corticosteroids antenatally and all had received two doses of a natural surfactant. The other two infants, although born prematurely, had congenital diaphragmatic hernia (CDH) and were studied after operative closure of the diaphragmatic defect. We, therefore, have given the results for the total sample size and also only for the 16 infants with RDS.
Results
Two infants required reintubation within 48 h of extubation, one had a CDH and the other had had RDS and a birthweight of 750 g. In the 18 infants overall, Pimax (p = 0.017), Pemax (p = 0.004), FRC (<0.0001), CRS (p = 0.002) and RRS (p = 0.004) had significantly improved at 6 h post-caffeine administration compared to baseline (Table 1). Exclusion of the two infants with CDH yielded similar results, in that Pimax (p = 0.039), Pemax (p = 0.007), FRC (p < 0.0001), CRS (p = 0.003) and RRS (p = 0.005) were significantly improved at 6 h post-caffeine administration compared to baseline (Table 1). Six hours post-caffeine administration, in the 18 infants overall the peak inspiratory pressure (PIP) tended to be lower both than at baseline and 6 h prior to caffeine administration (p = 0.066); the inspired oxygen concentration (FiO2) remained unchanged. In the 16 infants who had had RDS, the FiO2 remained unchanged, but the median PIP was significantly lower 6 h post-caffeine administration compared to either at baseline or 6 h prior to caffeine administration (p = 0.011; Table 2).
Discussion
We have demonstrated that caffeine administration in prematurely born infants being weaned from mechanical ventilation was associated with improvements in respiratory muscle strength and lung function. This was not a randomised trial as we felt it unethical to withhold caffeine from prematurely born infants following the results of the CAP trial [21] and the associated follow-up study [22] demonstrating caffeine administration was associated with a significant reduction in BPD and cerebral palsy. Each infant acted as their own control. We did not measure respiratory muscle strength and lung function 6 h before caffeine administration, as well as at baseline and 6 h later for logistical reasons, in particular the study period would have been 15 h. In addition, as decisions regarding caffeine administration were made on the consultant ward round, we felt it inappropriate to withhold caffeine for a further 6 h for a research study. We did, however, collect information on the inspired oxygen concentration and peak inflating pressures. There were no significant changes in the inspired oxygen concentrations or peak inflation pressures over the 6 h prior to caffeine administration, but after caffeine administration, there was a reduction in the peak pressure which was statistically significant in the infants who had had RDS. In a previously reported randomised study [7] in prematurely born infants during weaning, the compliance of those who had received theophylline improved from a mean of 0.67 to 0.95 ml/cm H2O 6 h post-theophylline administration, whereas in the controls the mean compliance did not alter significantly being 0.63 ml/cm H2O at baseline and 0.67 ml/cm H2O 6 h later. Thus, we feel that the improvements in respiratory muscle strength and lung function we describe were due to caffeine administration.
Our results demonstrating improved respiratory muscle function following caffeine administration are supported by certain findings in healthy adults [5, 20], although there are apparently conflicting results [18, 19]. In one study [5], trandiaphragmatic pressure (Pdi) during submaximal voluntary diaphragm contractions performed at similar levels of electromyogram activity was approximately 15% increased after aminophylline infusion. In addition, in another study [20], a 23% increase in Pdi twitch amplitude with supramaximal bilateral phrenic nerve stimulation using needle stimulating electrodes in ten normal subjects was reported following aminophylline infusion. Others [18, 19], however, using the twitch response following supramaximal phrenic nerve stimulation found no improvement in twitch Pdi after aminophylline infusion, but unilateral stimulation was employed by Moxham et al. [19] and this may not be sensitive enough to detect small changes in contractility. The apparently conflicting results may also be explained by the use of different methylxanthines. Both in vitro in the isolated rat diaphragm [4] and in vivo in the intact human [23], caffeine has been demonstrated to have a greater effect on diaphragm contractility than theophylline at the same therapeutic dosage.
To measure inspiratory and expiratory muscle function, a two-way non-breathing valve was used; occlusion of the inspiratory limb allowed expiration but not inspiration, whereas occlusion of the expiratory limb allowed inspiration but not expiration. The unidirectional valve selectively permits unidirectional flow, such that inspiratory efforts occur from progressively lower lung volume and expiratory efforts from progressively higher lung volume resulting in greater pressure generation than when lung volume is at FRC due to improvements in the length–tension relationship of respiratory muscles [6]. As length and geometry can influence the pressure development by the inspiratory and expiratory muscles [5], we also ensured occlusions were always performed at end inspiration for Pemax and end expiration for Pimax. To further reduce variability, occlusions were performed with the patient in the same supine position to eliminate differences in body position and ribcage configuration. The infants were all ventilated via shouldered endotracheal tubes [14]; thus, pressure loss was likely to be minimal or without occurrence.
Caffeine administration was also associated with improvements in compliance and resistance of the respiratory system. These results are consistent with findings from the majority of previous studies [2, 3, 10, 15, 16, 26]. Methylxanthines may increase compliance by stimulation of the surfactant pathway [1] and/or enhancement of the frequency of provoked augmented inspirations [8]. To our knowledge, however, this is the first study demonstrating that caffeine administration is associated with increases in lung volume.
We recruited consecutive infants who were born prematurely and whose parents gave informed written consent. This meant we included two infants who had CDH, nevertheless, despite the wide range of gestational ages and birth weights, we observed significant differences. Exclusion of the two infants with CDH did not influence the results, in that caffeine administration was associated with significant improvements in respiratory muscle strength and lung function in the 18 infants overall and also in the 16 infants who had RDS. As only two of the 18 infants failed extubation, one of whom had a CDH, we did not feel it appropriate to subject that data to statistical analysis. Thus, we cannot comment whether a need for reintubation may be predicted by the magnitude of change in respiratory muscle strength following caffeine administration.
In conclusion, we have demonstrated that caffeine administration improves respiratory muscle strength in prematurely born infants being weaned from mechanical ventilation and this is associated with improvements in lung function. We speculate that the improvement in respiratory muscle strength may explain why caffeine administration facilitates extubation.
References
Cosmi EV, Saitto C, Barbati A et al (1986) Effect of aminophylline on lung maturation in preterm rabbit fetuses. Am J Obstet Gynecol 154:436–439
Davi MJ, Sankaran K, Simons KJ et al (1978) Physiologic changes induced by theophylline in the treatment of apnea in preterm infants. J Pediatr 92:91–95. doi:10.1016/S0022-3476(78)80084-5
Davis JM, Bhutani VK, Stefano JL et al (1989) Changes in pulmonary mechanics following caffeine administration in infants with bronchopulmonary dysplasia. Pediatr Pulmonol 6:49–52. doi:10.1002/ppul.1950060112
Golgeli A, Ozesmi C, Ozesmi M (1995) The effects of theophylline and caffeine on the isolated rat diaphragm. Acta Physiol Pharmacol Ther Latinoam 45:105–113
Grassino A, Goldman MD, Mead J et al (1978) Mechanics of the human diaphragm during voluntary contraction: statics. J Appl Physiol 44:829–839
Green M, Road J, Sieck GC et al (2002) Tests of respiratory muscle strength: ATS/ERS statement on respiratory muscle testing. Am J Respir Crit Care Med 166:528–547
Greenough A, Elias-Jones A, Pool J et al (1985) The therapeutic actions of theophylline in preterm ventilated infants. Early Hum Dev 12:15–22. doi:10.1016/0378-3782(85)90132-X
Greenough A, Morley CJ, Davis JA (1984) Provoked augmented inspirations in ventilated premature babies. Early Hum Dev 9:111–117. doi:10.1016/0378-3782(84)90091-4
Greenough A, Prendergast M (2008) Difficult extubation in low birthweight infants. Arch Dis Child Fetal Neonatal Ed 93:F242–F245. doi:10.1136/adc.2007.121335
Heaf DP, Turner H, Stocks J et al (1987) Comparison of the occlusion and inflation techniques for measuring total respiratory compliance in sick, intubated infants. Pediatr Pulmonol 3:78–82. doi:10.1002/ppul.1950030207
Henderson-Smart DJ, Davis PG (2003) Prophylactic methylxanthines for extubation in preterm infants. Cochrane Database Syst Rev CD000139.
Hey EN (1969) The relation between environmental temperature and oxygen consumption in the new-born baby. J Physiol 200:589–603
Heyman E, Ohlsson A, Heyman Z et al (1991) The effect of aminophylline on the excursions of the diaphragm in preterm neonates. A randomized double-blind controlled study. Acta Paediatr Scand 80:308–315. doi:10.1111/j.1651-2227.1991.tb11854.x
Hird M, Greenough A, Gamsu H (1990) Gas trapping during high frequency positive pressure ventilation using conventional ventilators. Early Hum Dev 22:51–56. doi:10.1016/0378-3782(90)90025-E
Kao LC, Durand DJ, Nickerson BG (1988) Improving pulmonary function does not decrease oxygen consumption in infants with bronchopulmonary dysplasia. J Pediatr 112:616–621. doi:10.1016/S0022-3476(88)80184-7
Kao LC, Durand DJ, Phillips BL et al (1987) Oral theophylline and diuretics improve pulmonary mechanics in infants with bronchopulmonary dysplasia. J Pediatr 111:439–444. doi:10.1016/S0022-3476(87)80476-6
Laubscher B, Greenough A, Dimitriou G (1998) Comparative effects of theophylline and caffeine on respiratory function of prematurely born infants. Early Hum Dev 50:185–192. doi:10.1016/S0378-3732(97)00038-6
Levy RD, Nava S, Gibbons L et al (1990) Aminophylline and human diaphragm strength in vivo. J Appl Physiol 68:2591–2596
Moxham J (1988) Aminophylline and the respiratory muscles: an alternative view. Clin Chest Med 9:325–336
Murciano D, Aubier M, Viires N et al (1987) Effects of theophylline and enprofylline on diaphragmatic contractility. J Appl Physiol 63:51–57
Schmidt B, Roberts RS, Davis P et al (2006) Caffeine therapy for apnea of prematurity. N Engl J Med 354:2112–2121. doi:10.1056/NEJMoa054065
Schmidt B, Roberts RS, Davis P et al (2007) Long-term effects of caffeine therapy for apnea of prematurity. N Engl J Med 357:1893–1902. doi:10.1056/NEJMoa073679
Supinski GS, Deal EC Jr, Kelsen SG (1984) The effects of caffeine and theophylline on diaphragm contractility. Am Rev Respir Dis 130:429–433
Thompson PJ, Greenough A, Hird MF et al (1992) Nosocomial bacterial infections in very low birth weight infants. Eur J Pediatr 151:451–454. doi:10.1007/BF01959362
Tong MR, Kang XM, Suetsugu S et al (1993) Effects of caffeine on diaphragmatic contractility and fatigue. Chin Med J (Engl) 106:751–756
Yoder B, Thomson M, Coalson J (2005) Lung function in immature baboons with respiratory distress syndrome receiving early caffeine therapy: a pilot study. Acta Paediatr 94:92–98. doi:10.1080/08035250410023160
Acknowledgement
Dr. Kassim was supported by King’s College Hospital Foundation Trust.
Conflict of interest statement
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kassim, Z., Greenough, A. & Rafferty, G.F. Effect of caffeine on respiratory muscle strength and lung function in prematurely born, ventilated infants. Eur J Pediatr 168, 1491–1495 (2009). https://doi.org/10.1007/s00431-009-0961-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-009-0961-9