



Chest x-ray or CT for COVID-19 pneumonia? Comparative study in a simulated triage setting
- Nicola Sverzellati1⇑,
- Christopher J Ryerson2,
- Gianluca Milanese1,
- Elisabetta A Renzoni3,
- Annalisa Volpi4,
- Paolo Spagnolo5,
- Francesco Bonella6,
- Ivan Comelli7,
- Paola Affanni8,
- Licia Veronesi8,
- Carmelinda Manna1,
- Andrea Ciuni1,
- Carlotta Sartorio1,
- Giulia Tringali1,
- Mario Silva1,
- Emanuele Michieletti9,
- Davide Colombi9 and
- U Athol Wells3
- 1Scienze Radiologiche, Dipartimento di Medicina e Chirurgia, University-Hospital of Parma, Parma, Italy
- 2Department of Medicine, University of British Columbia and Centre for Heart Lung Innovation, St. Paul's Hospital, Vancouver, Canada
- 3Interstitial Lung Disease Unit, Royal Brompton Hospital, Imperial College, London, UK
- 41st Anesthesia and Intensive Care Unit, University Hospital of Parma, Parma, Italy
- 5Respiratory Disease Unit, Department of Cardiac, Thoracic, Vascular Sciences and Public Health, University of Padova, Padua, Italy
- 6Center for Interstitial and rare Lung Diseases, Pneumology Department, Ruhrandklinik University Hospital, University of Duiburg-Essen, Essen, Germany
- 7Unità Operativa Pronto Soccorso e Medicina d' Urgenza, Azienda Ospedaliero-Universitaria di Parma, Parma, Italy
- 8Department of Medicine and Surgery, University of Parma, Parma, Italy
- 9Department of Radiological Functions, Radiology Unit, “Guglielmo da Saliceto” Hospital, Piacenza, Italy
- Nicola Sverzellati, Scienze Radiologiche, Dipartimento di Medicina e Chirurgia, Università di Parma, Padiglione Barbieri, Scienze Radiologiche, Azienda Ospedaliero-Universitaria di Parma, Parma, 43126, Italy. E-mail: nicola.sverzellati{at}unipr.it
Abstract
Introduction: for the management of patients referred to respiratory triage during the early stages of the SARS-CoV-2 pandemic, either chest radiograph (CXR) or computed tomography (CT) were used as first-line diagnostic tools. The aim of this study was to compare the impact on triage, diagnosis and prognosis of patients with suspected COVID-19 when clinical decisions are derived from reconstructed CXR or from CT.
Methods: we reconstructed CXR (r-CXR) from high-resolution CT (HRCT) scan. Five clinical observers independently reviewed clinical charts of 300 subjects with suspected COVID-19 pneumonia, integrated with either r-CXR or HRCT report in two consecutive blinded and randomised sessions: clinical decisions were recorded for each session. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and prognostic value were compared between r-CXR and HRCT. The best radiological integration was also examined to develop an optimised respiratory triage algorithm.
Results: interobserver agreement was fair (Kendall's W=0.365; p<0.001) by r-CXR-based protocol and good (Kendall's W=0.654; p<0.001) by CT-based protocol. NPV assisted by r-CXR (31.4%) was lower than that of HRCT (77.9%). In case of indeterminate or typical radiological appearence for COVID-19 pneumonia, extent of disease on r-CXR or HRCT were the only two imaging variables that were similarly linked to mortality by adjusted multivariable models
Conclusions: the present findings suggest that clinical triage is safely assisted by CXR. An integrated algorithm using first-line CXR and contingent use of HRCT can help optimise management and prognostication of COVID-19.
Introduction
Despite worldwide efforts to halt its transmission, severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) has affected more than 30 million individuals and caused nearly 1 million deaths as of late September 2020 [1, 2]. After the initial outbreak, most countries have prepared their healthcare systems to face the pandemic. Although highly desirable, global and shared preparedness planning has faced political, institutional, social, environmental, and technological challenges [3, 4]. A recent International survey reported substantial heterogeneity in the diagnostic approach to coronavirus disease 2019 (COVID-19) pneumonia within and among countries and continents [4].
To date, molecular testing is used in both symptomatic or asymptomatic subjects with risk of contamination. However, the use of imaging, particularly the choice of imaging technique, is still a matter of debate [5–8]. Molecular and imaging testing are helpful in different aspects of the disease and their integration should be driven by dynamic protocols to be adapted as knowledge of the disease improves. The use of real-time reverse transcription-polymerase chain reaction (RT-PCR) was adapted to the massive needs by shortening of reaction time (and thus reporting time), yet it is still challenged by a substantial proportion of false negatives [9]. Conversely, imaging can show signs of pneumonia in patients with negative RT-PCR but clinically suspected COVID-19, thus offering a potential role in supporting rapid decision making [9, 10]. The use of imaging was thus recommended for patients who present at triage with moderate to severe features of COVID-19 pneumonia regardless of RT-PCR results [7].
Different imaging approaches are available and have been discussed in the recent COVID-19 literature, including chest X-ray (CXR) and computed tomography (CT). There is still no international consensus upon the integrated use of CXR or CT for clinical assessment and management of subjects with suspected COVID-19 pneumonia [4–6, 11–17]. Most concerns are focused on the accuracy of these tests, individual resources, and risk of infection for radiographers and other healthcare employees. However, the scientific debate lacks important evidence on the impact of CXR and CT on triage decisions and patient care.
In this study, we sought to use a post-processing imaging technique to retrospectively reconstruct CXR from CT scan, and compare the impact of these two imaging tools on the initial clinical triage, diagnosis and prognosis of patients with suspected COVID-19.
Methods
Study population
The study population comprised patients who had been evaluated with chest high-resolution computed tomography (HRCT) scan by the COVID-19 respiratory triage of the University Hospital of Parma, which is located in one of the most affected areas in Northern Italy. In brief, patients were screened for symptoms (e.g. fever and dyspnea) and oxygen saturation. Patients with moderate to severe pulmonary involvement (e.g. oxygen saturation ≤95%) underwent HRCT scan. Given the turnaround times for SARS-CoV-2 testing results (e.g. ranging from 2 to >48 h), a presumptive diagnosis based on clinical-radiological findings was considered for swift decision making such as discharge, recommendation for home quarantine, or hospitalisation in different hospital areas including either dedicated COVID-19 pavilions or non-COVID-19 wards. Details on clinical triage were previously reported [8].
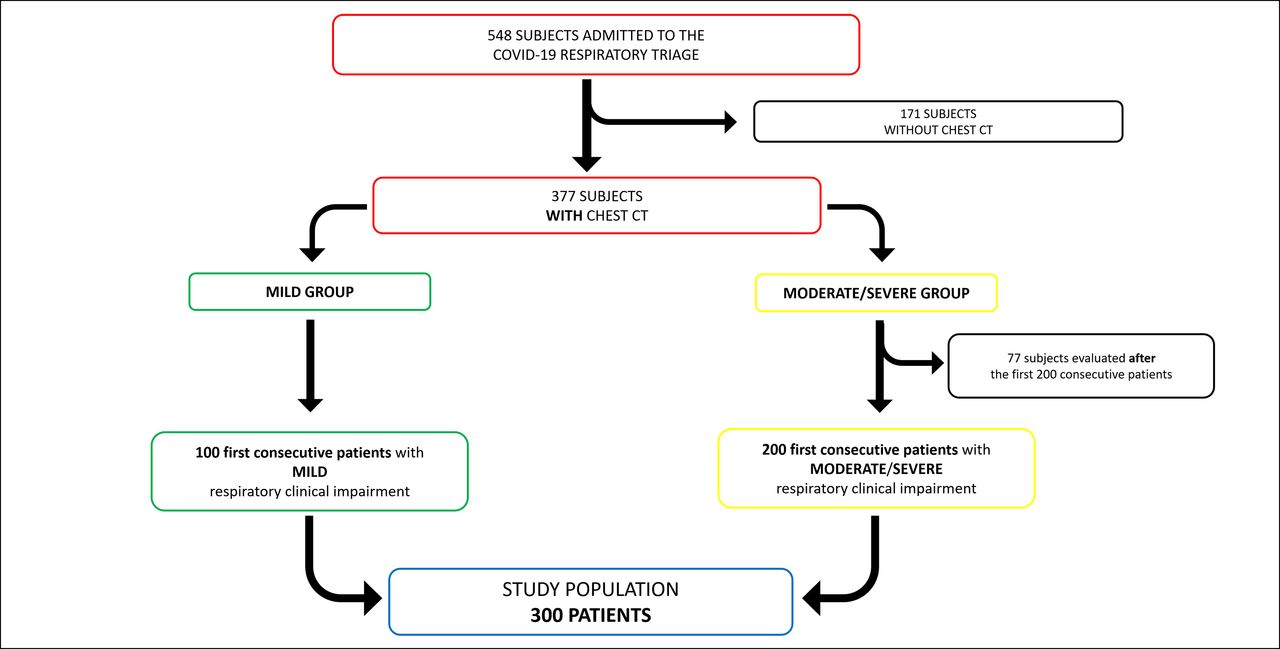
The study derivation cohort was built up by including 300 patients who consecutively underwent HRCT at the Parma triage from 29th February to 7th March 2020, as follows: the first 200 patients consecutively admitted to the triage with moderate-severe respiratory clinical impairment were mixed up with the first 100 patients consecutively admitted with mild respiratory clinical impairment (e.g. oxygen saturation 96–98%, hyperthermia, tachypnea) (fig. 1). The addition of this subgroup ensured that the full spectrum of COVID-19 severity was evaluated.

Diagram illustrating the selection of the derivation study cohort.
The study results were externally validated in a cohort of 104 patients (validation cohort) consecutively evaluated at a neighbouring hospital during the same time frame (Piacenza, Italy), which adopted a similar diagnostic protocol (see also supplementary material).
This retrospective study was approved by the referring local Review Board. Informed consent was obtained from the study patients.
Imaging technique
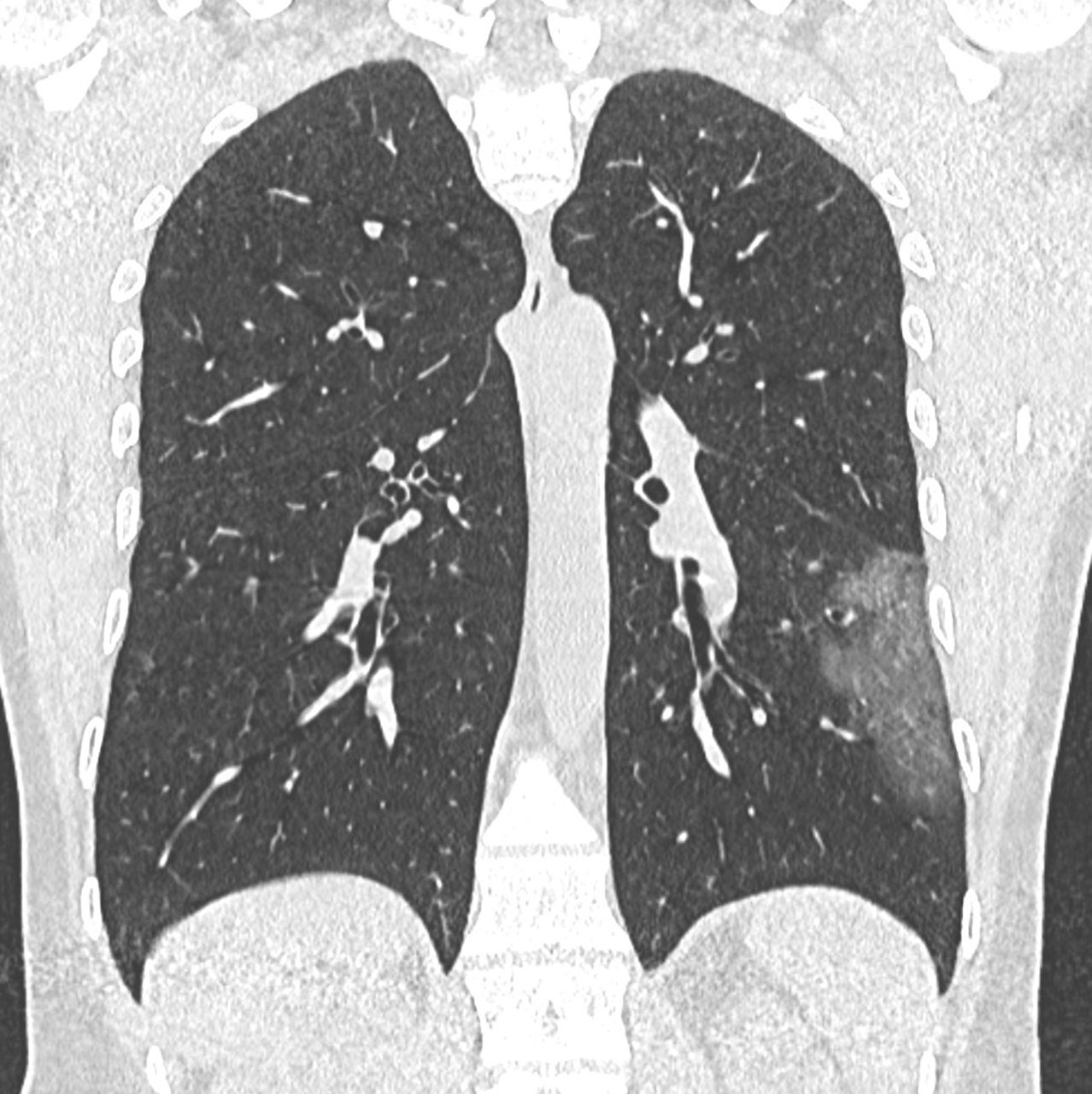
Details on CT scanners and HRCT technique are reported in the supplementary material. HRCT scans allow for various post-processing reconstruction algorithms, including Average Intensity Projection (AIP) [18]. AIP images represent the average of each component attenuation values encountered by the X-ray beam through an object. By manipulating the slab thickness of the coronal AIP mages, it was possible to obtain images analogous to frontal CXR, hereafter called reconstructed (r)-CXR (online videoclip, figures 2–4). Further illustrations, videos and technical details of the conversion from HRCT to r-CXR imaging, as well as evaluation of r-CXR consistency with standard CXR are reported in the supplementary material.


Reconstructed chest X-ray (r-CXR) (a) and coronal multiplanar reconstruction (MPR) of high-resolution computed tomography (HRCT) (b) of a 41 years old male patient with unilateral COVID-19 pneumonia. Focal, ovoid area of ground glass opacity in the left lower lobe was identified at both r-CXR and HRCT by the study observers. The extent of disease at r-CXR was scored as category 0 (<20%) by both the study observers when using the prognostic scoring system.


Reconstructed chest X-ray (r-CXR) (a) and coronal multiplanar reconstruction (MPR) of high-resolution computed tomography (HRCT) (b) of a 71 years old male patient with bilateral COVID-19 pneumonia. Bilateral, peripheral ground glass opacities were reported at both r-CXR and HCRT. However, disease extent was scored as category 0 (<20%) on r-CXR and category 1 (20–50%) on HRCT.


Reconstructed chest X-ray (r-CXR) (a) and coronal multiplanar reconstruction MPR of high-resolution computed tomography (HRCT) (b) of a 41 years old female patient with severe COVID-19 pneumonia. Bilateral, diffuse ground glass opacities and consolidations occupy most of the lung parenchyma, and the disease extent was scored as category 2 (>50%) both on r-CXR and HRCT.
HRCTs were prospectively scored by a senior chest radiologist (NS, 16-year experience in imaging of interstitial lung disease). He recorded individual HRCT abnormalities and graded the HRCTs into four diagnostic categories, as follows: normal, alternative diagnosis (to be specified), indeterminate, or typical for COVID-19 pneumonia [8]. The total extent of pulmonary disease was scored to the nearest 5%.
In keeping with the visual scoring of the HRCT, two radiologist observers (CM and AC with 11- and 4-year experience in chest imaging, respectively) recorded individual r-CXR abnormalities and graded the r-CXR as follows: normal, alternative diagnosis (to be specified), indeterminate, or typical for COVID-19 pneumonia. The total extent of pulmonary disease on r-CXR was evaluated through an overall visual impression, using a four-point-scale: 0) no parenchymal abnormality; 1) <20%; 2) 20–50%; 3) >50%. Interobserver discrepancies for both diagnostic categories and disease extent were resolved by consensus.
Clinical assessment in a triage-like setting
Clinical data for each patient were jointly reported in data sheets by a consultant anesthesiologist (AV) and a radiologist (GM) table 1. These data were assembled into individual clinical charts that were given for simulation of clinical management to each clinical observer of this study. RT-PCR test results were not included in the clinical charts in order to simulate an environment where turnaround times were long.
Baseline characteristics, presentation vitals and laboratory results of Patients admitted to the respiratory triage for COVID-19 (derivation and validation cohort)
Five clinical observers from three different countries participated in the study. These comprised three physicians (AV, IC, FB) who worked at a HRCT-based triage, and two physicians (PS, EAR) whose hospital protocol proposed a CXR-based triage. Details on the study observer characteristics are given in the supplementary material. Each clinical observer was asked to independently read twice the full set of clinical charts according to two different settings, as follows:
1) The first review was designed to simulate r-CXR-based integrated clinico-radiological protocol: each clinical observer reviewed the data sheet and r-CXR report for each patient. Each clinical observer was asked to provide a clinical decision according to one of the following options:
a. discharge,
b. hospitalisation in non-COVID-19 area,
c. home quarantine,
d. hospitalisation in COVID-19 area,
e. further work-up by chest HRCT.
2) The second review was designed to simulate HRCT-based integrated clinico-radiological protocol: after 2 days from the first review completed, each clinical observer started the second of data sheet including HRCT report for each patient. Each clinical observer was asked to provide a clinical decision according to one of the following options:
a. discharge,
b. hospitalisation in non-COVID-19 area,
c. home quarantine,
d. hospitalisation in COVID-19 area.
The study observers were informed that this triage setting was supposed to simulate a pandemic environment with high influx of subjects with suspected COVID-19 pneumonia, and that the clinical decision could be expressed in the absence of any resource constraints.
Statistical analysis
The study analysis compared the frequency of each clinical decision category and its consistency between “r-CXR-based protocol” and “HRCT-based protocol”, by means of both intra- and inter-observers analysis. Either Chi-squared or McNemar test were used to compare r-CXR and HRCT diagnostic categories and RT-PCR results. Radiological data were compared between r-CXR and HRCT by the weighted-kappa coefficient to evaluate interobserver agreement. Kendall W test was used to evaluate the overall interobserver clinical decision agreement by r-CXR-based or HRCT-based protocol. Further details are provided in the supplementary material.
Spearman's rank correlation coefficient disease was used to evaluate the correlation between r-CXR-extent and HRCT-extent of disease.
Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of both r-CXR and HRCT diagnostic categories were calculated against RT-PCR, by grouping normal to alternative diagnosis and indeterminate to typical for COVID-19 pneumonia diagnostic categories, respectively.
Unadjusted and multivariable logistic regression analyses were used to identify the contribution of clinical and radiological variables to mortality prediction. Multivariable models included age, sex, duration of symptoms at triage, and a comorbidity score of 0–4, obtained by summing the presence (1 point for each) of individual comorbidities consistently associated with a poor outcome in previous reports (diabetes, hypertension, cardio-vascular disease, obesity). The classification performances of the models were evaluated by the area under the receiver operating characteristic curve (AUC).
Based on these models, we constructed a user-friendly five-point scale for both CT and CXR, integrating age and extent of disease on imaging (the only two variables emerging as strong independent determinants of mortality). These scales were externally tested in the validation cohort.
p values of less than 0.05 were considered to indicate statistically significant differences. Analyses were performed using STATA software (STATA Version 14; Computing Resource Centre, Santa Monica, CA).
Results
Study population
The derivation cohort included 300 patients (188 men and 112 women, 66.8±15.8, age range 23.1–97.6 years). Clinical and laboratory characteristics are summarised in table 1 and in the supplementary material. The mean time interval between the onset of symptoms and the triage assessment (and also HRCT scanning) was 6.3 days (±4.4). A total of 248 patients underwent RT-PCR testing. A total of 162/248 (65.3%) subjects tested positive at initial RT-PCR. Repeat RT-PCR testing was performed if the first RT-PCR was negative, identifying an additional 28 positive cases, thus resulting in an overall 190/248 (76.6%) positive RT-PCR. Vital status was ascertained for 295 out of 300 (98.3%) subjects. All patients were followed until death or a minimum of 30 days (range of follow up 1–153 days).
The characteristics of both derivation and validation cohort are summarised in table 1.
Inter- and intra-observer agreement for the clinical decision
The clinical decision according to either r-CXR-based protocol or HRCT-based protocol is summarised in tables 2 and 3. The overall interobserver agreement by r-CXR-based protocol was fair (Kendall's W=0.365; p<0.001), and it improved to good by HRCT-based protocol (Kendall's W=0.654; p<0.001). This was true even after stratification for categories of oxygen saturation levels (Supplementary Table 1). Of note, opposite trends in the agreement across the range of prespecified oxygen saturation levels were observed: the lower the oxygen saturation the worse the agreement by r-CXR and the better the agreement by HRCT-based protocol (Supplementary Table 1).
Management according to r-CXR-based protocol and HRCT-based protocol
HRCT-based recommendation for subjects for whom HRCT was requested at the r-CXR-based round
Paired interobserver agreement (Supplementary Table 2) by r-CXR ranged from poor (0.17–Obs1/Obs5) to moderate (0.50–Obs2/Obs4), and it ranged from fair (0.23–Obs1/Obs5) to good (0.75–Obs2/Obs4) by HRCT-based protocol.
Intra-observer agreement on the clinical decision by either r-CXR or HRCT ranged from fair (0.37) to good (0.71) (Supplementary Table 3).
In the r-CXR round, further work-up by HRCT scan was requested in 8% to 46% of patients by the study observers. Once the HRCT was provided, the most frequent decision in this group was COVID hospitalisation (41.7% to 73.2%) (table 3). In particular, HRCT scan was requested by at least one observer for a total of 224 (74.7%) patients, while a management decision without request of HRCT (only clinico-r-CXR findings) was expressed by all observers in 76 (25.3%) patients (Supplementary Table 4). In the latter subgroup, the interobserver agreement was similar between r-CXR (Kendall's W=0.763; p<0.001) and HRCT (Kendall's W=0.725; p<0.001). When r-CXR was considered sufficient for the decision making by all the observers, patients had higher oxygen saturation, and reported more frequently a history of social contact with COVID-19 infected individuals, as compared to patients for whom HRCT was requested by any observer (Supplementary Table 4).
Unadjusted associations between mortality and core clinical and imaging variables in patients with chest radiographic findings compatible with COVID infection examined using logistic regression. Relationships are expressed as odds ratios for mortality, with 95% confidence intervals and p values
r-CXR versus HRCT
r-CXR and HRCT data are summarised in table 1.
Interobserver analysis data is given as supplementary data. Eighty-five r-CXR were classified normal, with 49/85 (57.6%) being false negative as compared to HRCT, notably 30/85 (35.3%) showing HRCT abnormalities consistent with COVID-19 pneumonia (ground-glass opacity in 26/30, 86.7%) with a mean disease extent on HRCT 23% (range 5–65%). Conversely, indeterminate r-CXR findings or r-CXR suggestive for a non-COVID-19 disease were each reported in 4/40 (10%) patients with normal HRCT, thus representing false positive r-CXR.
Of 190 patients with positive RT-PCR results, 156 (82.1%) had positive HRCT scans, and 133 (70%) had positive r-CXRs. Of 58 subjects with negative RT-PCR result, 28 (48.3%) had positive HRCT scans, and 31 (53.4%) had positive r-CXRs. The sensitivity, specificity, PPV, and NPV of HRCT in indicating COVID-19 infection were 95.2% (95%CI: 91.2%–97.8%), 32.8% (95%CI: 21%–46.3%), 82.2% (95%CI: 79.4%–84.7%) and 67.9% (95%CI: 50.3%–81.5%), respectively. The sensitivity, specificity, PPV, and NPV of r-CXR in indicating COVID-19 infection were 81.6% (95%CI 75.3%–86.8%), 27.6% (95%CI 16.7%–40.9%). 78.1% (95%CI 75%–80.9%) and 31.4% (95%CI 21.5%–43.3%), respectively.
Unadjusted associations between mortality and core clinical and imaging variables in patients with r-CXR findings compatible with COVID-19 pneumonia are summarised in table 4. Two models examined mortality against the extent of disease on either r-CXR or HRCT, using the same 4-point categorical grading system (table 4). In the logistic regression model with r-CXR, mortality was associated with extent of disease (OR=2.38; 95%CI 1.61–3.50; p<0.001). In the logistic regression model with HRCT, mortality was associated with extent of disease (OR=2.62; 95%CI 1.67–4.10; p<0.001). Both r-CXR and HRCT associations were robust with inclusion in models of age (also strongly linked to mortality), sex, duration of symptoms, and comorbidity score (Supplementary Table 5).
A further third model was built to explore a two-point grading system for risk stratification: the extent of disease was classified by contingent categories as either limited (r-CXR extent<20%; or r-CXR 20–50%, with HRCT extent 0–50%) or extensive (r-CXR extent >50%; or r-CXR 20–50%, with HRCT extent >50%). The distinction between limited and extensive disease was strongly associated with mortality (OR=5.24; 95%CI 2.69–10.22; p<0.001) and was robust with adjustment for age, sex, and comorbidity score (Supplementary Table 5).
Prognostic scoring systems using r-CXR, and HRCT
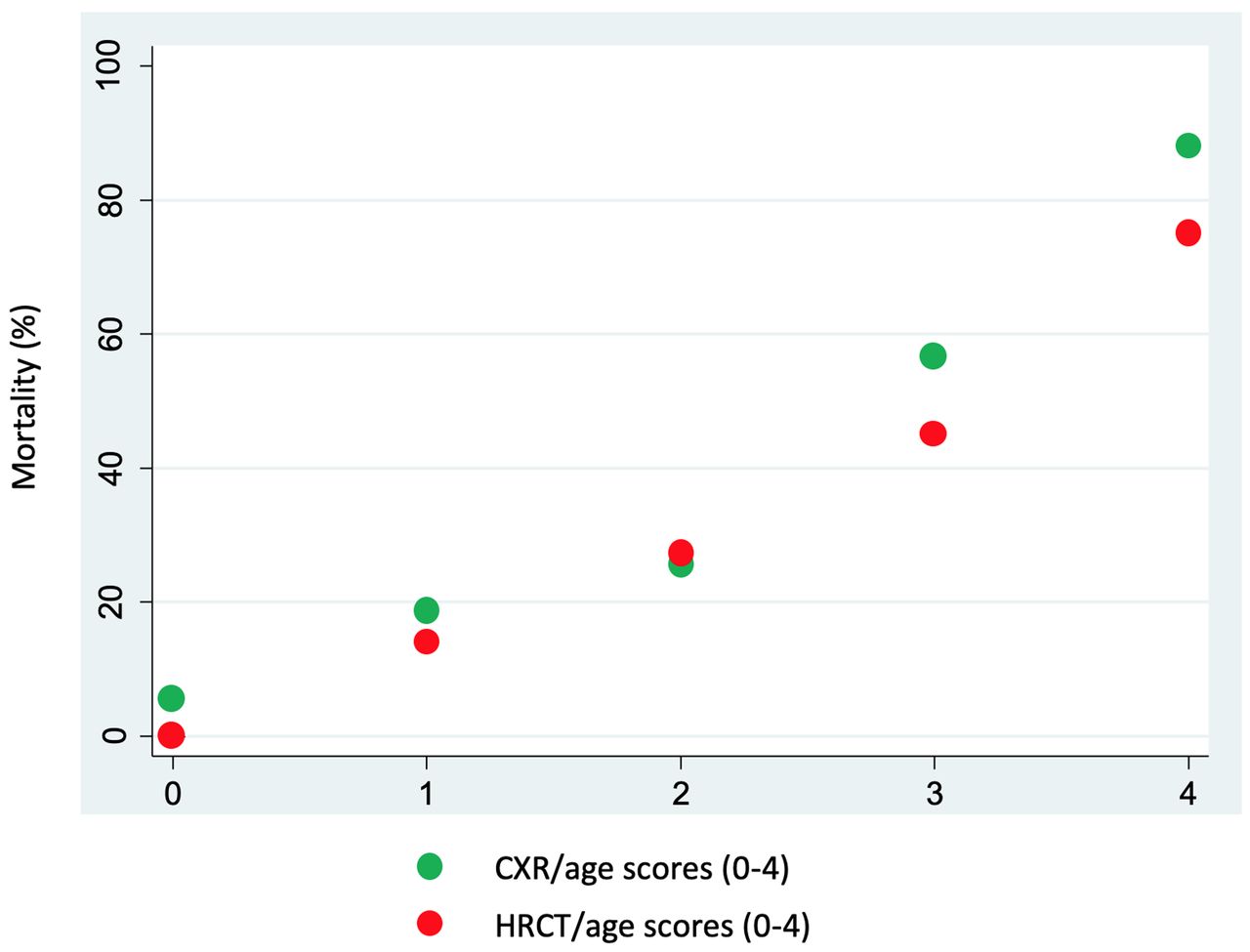
For each of the three abovementioned models, AUC values fell minimally when multivariable analysis was confined to age and extent of disease on imaging (Supplementary Table 5). Therefore, simplified scoring systems for r-CXR and HRCT were constructed based on these two variables. Age was categorised as <60 (score 0), 60–74 (score 1), and >74 (score 2) years, dividing the cohort into approximate thirds (OR=2.79; 95%CI 1.80–4.31; p<0.001). Imaging extent scores were categorised as <20% (score 0); 20–50% (score 1); >50% (score 2) (figs 2–4). Age and imaging scores were summed to provide five point scales (0–4) for age/r-CXR and age/HRCT scoring systems. Mortality in relation to the age/r-CXR and age/HRCT scores are shown in figure 5 and Supplementary Table 6.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mortality in relation to the age/reconstructed chest X-ray (r-CXR) and age/HRCT scores. Age and imaging scores into a five point scales (0–4), both for age/r-CXR and age/HRCT scoring systems.
In a logistic regression model, the age/r-CXR score was associated with mortality (OR=2.85; 95%CI 2.00–4.06; p<0.001), AUC=0.77. This finding was reproduced in the validation cohort (OR=2.48; 95%CI 1.47–4.17; p<0.001), AUC=0.73. In a separate logistic regression model, the age/HRCT score was associated with mortality (OR=2.71; 95%CI 1.92–3.84; p<0.005), AUC=0.76. This finding was reproduced in the validation cohort (OR=4.23; 95%CI 2.11–8.48; p<0.001), AUC=0.80.
Discussion
In this simulated COVID-19 pandemic triage for a high influx of patients with mostly moderate-to-severe clinical features suspicious of COVID-19 pneumonia, the use of r-CXR for morphology and extent of pneumonia allowed fair interobserver agreement for clinical management, however r-CXR with moderate extent displayed limited yield that could be assisted by integration by HRCT. The interobserver agreement considerably increased when using HRCT, which lead to an increase in the number of recommended hospitalisations. This observation is of particular relevance as the observers were from different countries, used various COVID-19 triage strategies in their daily practice, and had different subspecialty interests.
The major source of disagreement for the r-CXR-based protocol was the frequency of the requested HRCT scans, which ranged from 8% to 46% of cases. When HRCT work-up was not recommended by any of the study observers, the agreement was similar to that obtained with the HRCT-based protocol. Although we observed a tendency in considering the r-CXR sufficient in patients with milder pulmonary dysfunction, abnormal r-CXR and high exposure risk, the variety in requesting HRCT scans had still no obvious reasons (e.g. age, disease extent on r-CXR etc.). Such observation emphasises the need to define the clinical indications to CT scanning when the triage workflow relies on CXR as the first imaging modality. In fact, poorly defined criteria may unreasonably increase the number of CT scans after CXR, with potential detrimental effects on the workflow and healthcare worker safety.
In order to evaluate the clinical implications of the two imaging modalities, the sensitivity, the specificity, and the prognostic value of r-CXR and HRCT were compared. The levels of sensitivity for r-CXR were in keeping with previous findings [9, 16, 17, 19]. Sensitivity, specificity, and PPV of r-CXR were marginally lower than HRCT, whereas major discrepancy was found for NPV due to the remarkable proportion of false negative r-CXRs.
Any optimisation process of COVID-19 triage protocols should consider mortality data and resource utilisation predictions [20]. First, the proportion of deaths among patients with normal r-CXR was higher (12%) as compared to normal HRCT (5%). Such a discrepancy was also evident by comparing r-CXR- and HRCT-based prognostic scoring systems (fig. 5). Moreover, the distinction between typical COVID-19 pneumonia and indeterminate findings was not worthwhile for both r-CXR and HRCT as they were associated with similar outcomes. This suggests that, in a pandemic situation, indeterminate CXR or CT findings likely represent signs of COVID-19 pneumonia. Hence, after grouping indeterminate and typical COVID-19 categories, we found that the diagnostic categories had fairly major prognostic significance for both r-CXR and HRCT. This finding is important as the diagnostic categories used in the present study substantially overlap both CO-RADS categories and those proposed by the Radiologic Society of North America [8, 21].
Our findings do not suggest that HRCT extent scoring adds greatly to prognostic evaluation, over and above CXR scoring, and this is concordant with the need to first level approach by CXR to optimise use of radiology resources and maximise patient and healthcare employee safety. However, an alternative strategy–HRCT complement when CXR extent findings are intermediate–allowed categorisation into limited and extensive disease with a major prognostic separation. The proposed contingent staging algorithm–where r-CXR grades 1 (<20%) and 3 (>50%) are accepted and HRCT is used to adjudicate on r-CXR 2 (21–50%)–showed the highest prognostic value. Separation into a higher risk/lower risk dichotomy may have major clinical value but we suggest that this observation requires further exploration if CT is to be integrated into routine prognostic evaluation in selected cases, when CXR findings are not definitive.
The higher number of deaths in subjects with normal r-CXR still represents the main limitation of this staging system. In patients dying despite a r-CXR grade of 1, the HRCT extent grade was either intermediate or extensive in two thirds of cases. These data suggest that a first level approach by CXR will require some improvement in terms of sensitivity. Otherwise, first level approach by HRCT would provide major confidence in clinical decision and prognostication, therefore it might considered in the context of local logistics that minimise risk of contamination (e.g. dedicated scanner in proximity of the triage rooms).
This study has some limitations. It is worth emphasising that our observations were derived from a pre-peak endemic environment (e.g. when RT-PCR demand was beyond capacity), while the triage process is being adjusted as the endemic changes. Nevertheless, the study findings may still be helpful in epidemic scenarios, the increased availability of the lab test results within a few hours could further mitigate the CXR limitations (e.g. lower diagnostic accuracy as compared to CT), encouraging its use. Moreover, the reported heterogeneity in the request of HRCT scans among the study observers when first interpreting a CXR might be overrated as a simulated triage setting does not likely reflect the routine clinical context, where multidisciplinary discussion (e.g. between radiologists and triagers) could support other clinical decisions with better integration of available data. The CXR was derived from HRCT data given the impossibility of running a two arm-randomised-controlled trial between CXR and CT in the COVID-19 setting, yet we tested this approach against original CXR (supplementary materials).
In conclusion, this study showed that r-CXR findings were often regarded as not sufficiently informative by clinicians in a COVID-19 pandemic triage setting. This observation suggests that chest CT should be considered after CXR in a substantial percentage of patients with suspected COVID-19 pneumonia, thus potentially causing detrimental effects in the absence of pre-defined diagnostic work-up criteria. Nevertheless, the present study findings suggest that clinicians could rely on positive CXR showing low or high extent of pneumonia, whereas intermediate extent by CXR should be complemented by CT for optimal classification into high and low risk group.
Data collected for the study will not be made available to others.
Support statement: The study was not funded.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Conflict of interests: Dr. Sverzellati has nothing to disclose.
Conflict of interests: Dr. Ryerson has nothing to disclose.
Conflict of interests: Dr. Milanese has nothing to disclose.
Conflict of interests: Dr. Renzoni has nothing to disclose.
Conflict of interests: Dr. Volpi has nothing to disclose.
Conflict of interests: Dr. Spagnolo reports grants, personal fees and non-financial support from Roche, grants, personal fees and non-financial support from PPM Services, personal fees from Red X Pharma, personal fees from Galapagos, personal fees from Chiesi, grants, personal fees and non-financial support from Boehringer-Ingelheim, outside the submitted work and Wife employee of Novartis. .Dr. Spagnolo reports grants, personal fees and non-financial support from Roche, grants, personal fees and non-financial support from PPM Services, personal fees from Red X Pharma, personal fees from Galapagos, personal fees from Chiesi, grants, personal fees and non-financial support from Boehringer-Ingelheim, outside the submitted work; and Wife employee of Novartis.
Conflict of interests: Dr. Bonella reports personal fees and non-financial support from Boehringer Ingelheim, personal fees and non-financial support from Roche, personal fees and non-financial support from Galapagos, personal fees and non-financial support from Savara Pharma, personal fees and non-financial support from BMS, outside the submitted work.
Conflict of interests: Dr. Comelli has nothing to disclose.
Conflict of interests: Dr. Affanni has nothing to disclose.
Conflict of interests: Dr. Veronesi has nothing to disclose.
Conflict of interests: Dr. Manna has nothing to disclose.
Conflict of interests: Dr. Ciuni has nothing to disclose.
Conflict of interests: Dr. Sartorio has nothing to disclose.
Conflict of interests: Dr. Tringali has nothing to disclose.
Conflict of interests: Dr. Silva has nothing to disclose.
Conflict of interests: Dr. Michieletti has nothing to disclose.
Conflict of interests: Dr. Colombi has nothing to disclose.
Conflict of interests: Dr. Wells U reports personal fees and other from ROCHE, personal fees and other from BI, personal fees and other from Bayer, from null, outside the submitted work.
- Received November 13, 2020.
- Accepted January 27, 2021.
- ©The authors 2021. For reproduction rights and permissions contact permissions{at}ersnet.org