



Early COVID-19 Lockdown in Greece and IPF: A beneficial “impact” beyond any expectation
- Spyros A. Papiris1,
- Demosthenes Bouros2,3,
- Katerina Markopoulou4,
- Lykourgos Kolilekas5,
- Andriana I. Papaioannou1,
- Vasilios Tzilas3,
- Argyrios Tzouvelekis6,
- Eva Fouka7,
- Despoina Papakosta7,
- Zoe Daniil8,
- Paschalis Steiropoulos9,
- Athina Gogali10,
- Ilias C. Papanikolaou11,
- Areti Xyfteri12,
- Aggeliki Haritou13,
- Ioanna Korbila1,
- Ioannis P. Tomos1,
- Stylianos Loukides1,
- Rita Bellelli1,
- Georgia Kounti4,
- Christina Rampiadou4,
- Theodoros Karampitsakos6,
- Ilias Dimeas8,
- Paraskevi Kirgou8,
- Andromachi Bompoki14,
- Eirini Vasarmidi14,
- Konstantinos Loverdos5,
- Elvira-Markela Antonogiannaki1,
- Myrto Blizou1,
- Evangelos Bouros3,
- Konstantinos Kagouridis1,
- Maria Maniati1,
- Anna Karakatsani1,
- Katerina M. Antoniou14,15 and
- Effrosyni D. Manali1,15
- 12nd Pulmonary Medicine Department, General University Hospital “Attikon”, Medical School, National and Kapodistrian University of Athens, Athens, Greece
- 2First Academic Department of Pneumonology, Hospital for Diseases of the Chest “Sotiria”, Medical School, National and Kapodistrian University of Athens, Athens, Greece
- 3Iatriko Medical Center, Athens, Greece
- 4Pulmonary Department, “G Papanikolaou” General Hospital, Thessaloniki, Greece
- 57th Pulmonary Department, Athens Chest Hospital “Sotiria”, Athens Greece
- 6Department of Respiratory Medicine, General Hospital of Patras, University of Patras, Patra, Greece
- 7A Department of Pulmonary Medicine, Aristotle University of Thessaloniki, “G. Papanikolaou” Hospital, Exochi, Thessaloniki, Greece
- 8Department of Respiratory Medicine, Medical School, University of Thessaly, Larissa, Greece
- 9Department of Pneumonology, University Hospital of Alexandroupolis, Democritus University of Thrace, Komotini, Greece
- 10Department of Pneumonology, Medical School, University of Ioannina, Ioannina, Greece
- 11Pulmonary Department, Corfu General Hospital, Corfu, Greece
- 12Messini, Messinias, Greece
- 13Ioannina, Greece
- 14Department of Thoracic Medicine and Laboratory of Molecular and Cellular Pneumonology, Medical School, University of Crete, Heraklion, Crete, Greece
- 15these authors contributed equally to this work
- Dr Effrosyni D. Manali, Assistant Professor, General University Hospital “Attikon”, Medical School, National and Kapodistrian University of Athens, Greece. E-mail: fmanali{at}otenet.gr
Abstract
During the lockdown, IPF patients experienced lower than expected COVID-19 suggesting that simple measures for the winter months, such as face masking, clean hands, physical distancing could be adopted as promising advances in non-pharmacological therapy.
To the Editor
Idiopathic pulmonary fibrosis (IPF) is an irreversibly progressive diffuse lung disease characterised by a usual interstitial pneumonia pattern (UIP). IPF presents with an ominous prognosis with a median survival of around 5 years [1]. The development of an acute exacerbation (AE), histologically diffuse alveolar damage (DAD) upon UIP, represents the most devastating of its complications and leads to death the majority of patients admitted to intensive care unit (ICU) [2–4]. Viral infections in the setting of an altered host lung microbiome are likely important triggers of IPF-AE's and subsequent ARDS [4, 5].
In December 2019, a novel coronavirus was detected as an etiologic agent of Severe Acute Respiratory Syndrome named SARS-coronavirus 2 (SARS-CoV-2) with the potential of multiorgan involvement, disease named Corona Virus Disease-2019 (COVID-19), easily transmissible through respiratory routes [6]. Around 5% of patients develop critical manifestations necessitating ICU support with a mortality rate of 40% to 60% [7]. The mechanisms through which SARS-CoV-2 causes lung damage are partly known. It is postulated that the inhaled virus initially binds to nasal epithelial cells and starts propagating towards the lower respiratory tract reaching the alveoli where it infects preferentially alveolar type II cells [8]. Extensive viral replication leads to their apoptosis and cell-death, triggering through several inflammatory cascades DAD, clinically presenting as ARDS [9]. SARS-CoV-2 for its potential to induce pneumonia represents the novel infectious agent that could trigger in patients with IPF life-threatening AEs [10].
We hypothesised, that Greek IPF patients might have presented a spike increase in both hospitalisations and deaths during the first phase of the new viral epidemic. In this retrospective study we assessed the frequency, characteristics and outcome of COVID-19 in IPF patients followed-up in 11 specialised referral centers and 2 dedicated private practices all over Greece. Patients included in the study fulfilled ATS/ERS/JRS/ALAT criteria for definite/probable UIP/IPF (550 patients); excluded were patients with indeterminate or alternative ILD diagnosis (around 15% in each registry) [1]. COVID-19 diagnosis was based on the European Centre for Disease Prevention and Control “case definition for coronavirus disease 2019 criteria” [11]. The study period ranged from February 26th, 2020 when the first COVID-19 case was confirmed in Greece to May 2020, where after a strict lockdown, authorities started to lift restrictions. During this time-period 2632 COVID-19 cases and 146 deaths were officially reported distributed in every administrative region of the country [12]. IPF referral centers were located in university and tertiary hospitals all over Greece. Patients management was accomplished mainly by telephone or/and video appointments and by electronic prescription of treatment. Hospitalisations were not performed unless absolutely necessary. All registered IPF patients were contacted for informed consent. Demographic, epidemiologic, functional, clinical and microbiology data were retrospectively obtained by the medical records or/and hospital databases. Apart from COVID-19, any other lower respiratory tract infection necessitating hospitalisation, as well as, disease outcome was reported. Data concerning hospital admissions, lower respiratory tract infections necessitating hospitalisations and in-hospital deaths were compared with data of the same time-period of the year 2019. Patients deceased between May 2019 and March 2020 were not included in the cohort examined in 2020. Data were analysed using SPSS 18.0 for Windows (SPSS Inc, Chicago, IL, USA). The study was approved by the Medical Ethics Committee of the General University Hospital “Attikon”, Athens, Greece (ΕΒΔ 271/26-5-2020).
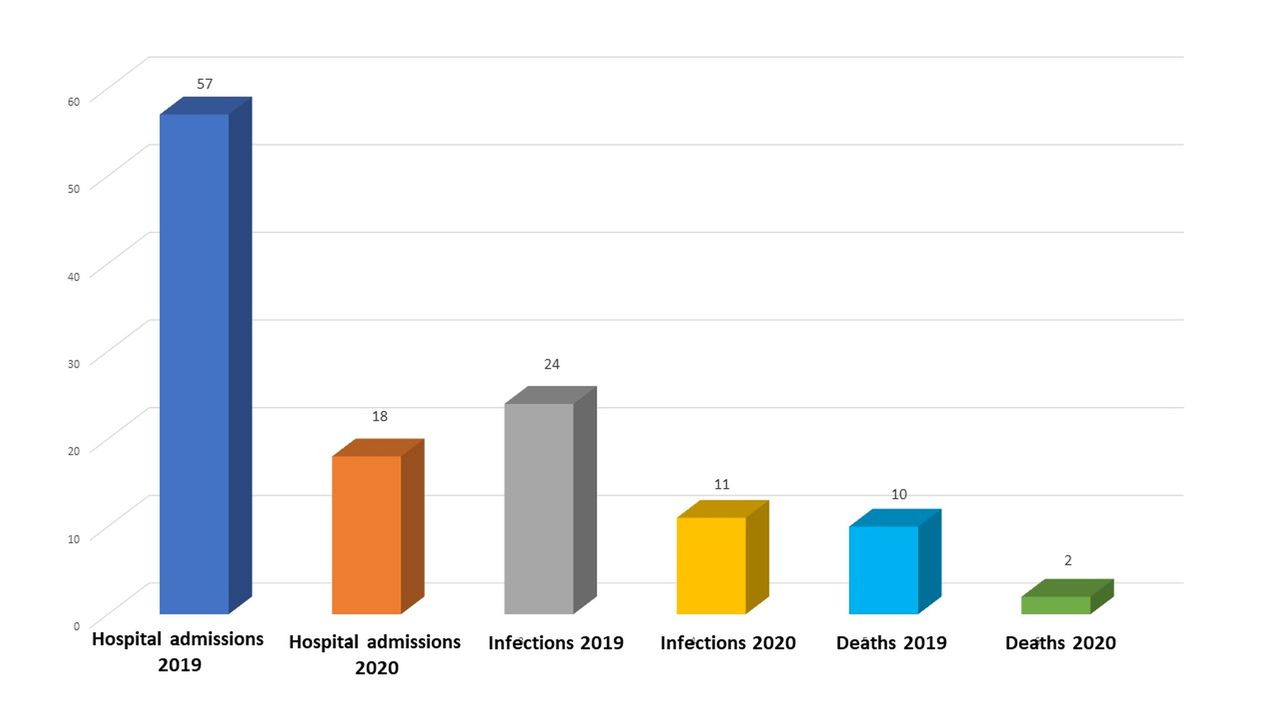
Overall, 550 patients, median age (IQR) of 74 years (68–78), 80.7% male, 72% ever- smokers with a median (IQR) FVC and DLCO % predicted, of 78 (64–91) and 46 (34–59) respectively and a median disease duration (IQR) of 26 months (12–43) were included in the study. Under antifibrotic treatment were 458 (83.3%), 76 (13.8%) were receiving no treatment and 16 (3%) were receiving immunosuppressive treatment. The majority suffered from at least one comorbidity such as arterial hypertension (51.3%), coronary artery disease (25.8%), diabetes mellitus (18.4%) and neoplastic disease (9.1%). Only 6.1% necessitated long-term oxygen therapy. Almost all patients were immunised against influenza (96.4%) and Streptococcus pneumoniae (87.1%). Only 2 patients (0.4%), one male 60 years-old and one female 91 years-old, first-degree relatives with recently diagnosed familial IPF developed COVID-19 and survived. Finally, during the lockdown compared to the same time-period in 2019 a decreased median number (IQR) of hospital admissions [0 (0,3) versus 3 (0,8)], lower respiratory tract infections necessitating hospitalisations [0 (0, 1.5) versus 2 (0, 3.5)] and in-hospital deaths [0 (0,0) versus 0 (0,2)] were reported. Despite numerical decrease in all aforementioned outcomes, statistical significance was not reached probably due to the small number of events (p=0.153, p=0.287, p=0.390, respectively) (fig. 1a and b). All in-hospital deaths, 10 in 2019 and 2 in 2020 (COVID-19 negative) were related to IPF-AE.

{kind=link}
{kind=link}
a) Histogram representation of the hospital admissions, lower respiratory tract infections necessitating hospitalisation and deaths in absolute numbers (axis y), during two comparative three-month time-periods (March-May 2019 and the lockdown period March to May 2020) regarding 550 IPF patients followed-up in 11 specialised referral centers and 2 dedicated private practices all over Greece. More precisely each number from 1 to 13 (axis x) corresponds to each center as follows: 1) “Attikon”, Athens (39 patients), 2) “Iatriko” and “Sotiria”, Athens (100 patients), 3) “G Papanikolaou” I, Thessaloniki (107 patients), 4) “Sotiria”, Athens (33 patients), 5) Patras (74 patients), 6) “G. Papanikolaou” II, Thessaloniki (65 patients), 7) Larissa (52 patients), 8) Alexandroupolis (22 patients), 9) Heraklion (18 patients), 10) Ioannina I (16 patients), 11) Corfu (16 patients), 12) Messini (5 patients) 13) Ioannina II (3 patients). b) Histogram representation of the overall hospital admissions, lower respiratory tract infections necessitating hospitalisation and deaths in absolute numbers (axis y), during two comparative three-month time-periods (March-May 2019 and the lockdown period March-May 2020) regarding 550 IPF patients followed-up in 11 specialised referral centers and 2 dedicated private practices all over Greece.
This study shows that during the strict COVID-19 lockdown applied in Greece, patients with IPF experienced much lower than expected COVID-19. At the same time, besides discrepancies between centers that could be attributed mainly to the random development of events, the heterogeneity in the population of each region and the policies for in-hospital management of IPF, an overall decrease in both hospitalisations related to other lower respiratory tract infections and deaths were reported.
Given the high virulence of the novel virus and the already described vulnerability of the study population, this observation could be attributed to the beneficial impact beyond any expectation of early lockdown measures imposed all over the country. IPF patients proved to be a disciplined population, in close contact with the treating physicians that by respecting scrupulously prophylactic measures avoided effectively the diffusion of several viral infections including SARS-CoV-2. The results of the present study are in accordance with similar ones referring to other chronic lung diseases such as COPD, demonstrating a significant decrease in the number of admissions for exacerbations in first 3 months of 2020, due to the adoption of protective measures [13]. One could hypothesise that other parameters could also play a role. However, for the moment no evidence exists that antifibrotic treatment may lower the risk of COVID-19 [14] and/or that intrinsic mechanisms could alter favorably the characteristics of COVID-19 in IPF. On the contrary, both COVID-19 and pulmonary fibrosis are considered severe diseases characterised by lung injury and dysregulated repair [14] and comorbid ILD is a risk factor for poor outcomes from COVID-19 [10].
Among the limitations of the study are its retrospective design and the potential bias related to missing patients. However, in this multicenter study it is very unlikely that IPF patients were hospitalised or deceased without being captured, since all hospitals of the IPF referral centers have been proclaimed COVID-19 referral centers too.
Given the life-saving impact of the lockdown in IPF patients concerning both COVID-19 and other viral lower respiratory tract infections, one wonders whether limited and periodically applied lockdown measures should be inflicted each year during the winter months in this specific population. Based on the fact that COVID-19 pandemic threatens both public health and human rights, we modern scientists could not impose such restrictive measures [15]. However, simple measures for the winter months, such as face masking, clean hands and physical distancing could be adopted and endorsed as the most recent and promising advances in non-pharmacological treatment in IPF.
Footnotes
Author's contributions: SAP conceived of the study, had major contribution to the analysis and interpretation of data and wrote with EDM the manuscript, DB had major contribution to the acquisition and interpretation of data for the work and revised critically this work for important intellectual content, KM had major contribution in the acquisition and interpretation of data for the work and revised critically this work for important intellectual content, LK participated in the design of the study and had major contribution to the acquisition, critical analysis and interpretation of data for the work, AIP performed the statistical analysis of the data, contributed substantially to the interpretation of data for the work and drafted parts of the manuscript and the figures, VT, AT, EF, DP, ZD, PS, AG, ICP, AH, AX, IK, IPT, SL had major contribution to the acquisition and analysis of data and were responsible for the integrity of data in their centers, RB, GK, CR, TK, ID, PK, AB, EV, KL, EMA, MB, EB, KK,MM had significant contribution to the acquisition and critical analysis of data, AK had substantial contribution to the analysis and interpretation of data and revised critically this work for important intellectual content, KMA participated at the conception and design of the study, had substantial contribution to the acquisition and analysis of data and was responsible for the integrity of data in her center, EDM had major contribution to the concept and design of the study, to the acquisition, analysis and interpretation of data, has access to all data, supervised the accuracy and integrity of any part of the work and wrote with SAP the manuscript. All authors read and approved of the final version of the submitted publication.
Conflict of interest: Dr. Papiris has nothing to disclose.
Conflict of interest: Dr. Bouros has nothing to disclose.
Conflict of interest: Dr. Markopoulou has nothing to disclose.
Conflict of interest: Dr. Kolilekas has nothing to disclose.
Conflict of interest: Dr. Papaioannou has nothing to disclose.
Conflict of interest: Dr. Tzilas has nothing to disclose.
Conflict of interest: Dr Tzouvelekis A has received advisory fees from Boehringer Ingelheim, Hoffmann La Roche, Chiesi Hellas and Elpen Pharma outside of the submitted work
Conflict of interest: Dr. Fouka has nothing to disclose.
Conflict of interest: Dr. Papakosta has nothing to disclose.
Conflict of interest: Dr. Daniil has nothing to disclose.
Conflict of interest: Dr. Steiropoulos has nothing to disclose.
Conflict of interest: Dr. Gogali has nothing to disclose.
Conflict of interest: Dr. Papanikolaou has nothing to disclose.
Conflict of interest: Dr. Xyfteri has nothing to disclose.
Conflict of interest: Dr. Haritou has nothing to disclose.
Conflict of interest: Dr. Korbila has nothing to disclose.
Conflict of interest: Dr. Tomos has nothing to disclose.
Conflict of interest: Dr. Loukides has nothing to disclose.
Conflict of interest: Dr. Bellelli has nothing to disclose.
Conflict of interest: Dr. Kounti has nothing to disclose.
Conflict of interest: Dr. Rabiadou has nothing to disclose.
Conflict of interest: Dr. Karampitsakos has nothing to disclose.
Conflict of interest: Dr. Dimeas has nothing to disclose.
Conflict of interest: Dr. Kirgou has nothing to disclose.
Conflict of interest: Dr. Bompoki has nothing to disclose.
Conflict of interest: Dr. Vasarmidi has nothing to disclose.
Conflict of interest: Dr. Loverdos has nothing to disclose.
Conflict of interest: Dr. Antonogiannaki has nothing to disclose.
Conflict of interest: Dr. Blizou has nothing to disclose.
Conflict of interest: Dr. E. Bouros has nothing to disclose.
Conflict of interest: Dr. Kagouridis has nothing to disclose.
Conflict of interest: Dr. Maniati has nothing to disclose.
Conflict of interest: Dr. Karakatsani has nothing to disclose.
Conflict of interest: Dr. Antoniou has nothing to disclose.
Conflict of interest: Dr. Manali has nothing to disclose.
- Received August 12, 2020.
- Accepted November 8, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.