



Characteristics of effective self-management interventions in patients with COPD: individual patient data meta-analysis
- Nini H. Jonkman1⇑,
- Heleen Westland1,
- Jaap C.A. Trappenburg1,
- Rolf H.H. Groenwold2,
- Erik W.M.A. Bischoff3,
- Jean Bourbeau4,
- Christine E. Bucknall5,
- David Coultas6,
- Tanja W. Effing7,
- Michael Epton8,
- Frode Gallefoss9,
- Judith Garcia-Aymerich10,11,12,
- Suzanne M. Lloyd13,
- Evelyn M. Monninkhof14,
- Huong Q. Nguyen15,
- Job van der Palen16,17,
- Kathryn L. Rice18,
- Maria Sedeno4,
- Stephanie J.C. Taylor19,
- Thierry Troosters20,
- Nicholas A. Zwar21,
- Arno W. Hoes2 and
- Marieke J. Schuurmans1
- 1Dept of Rehabilitation, Nursing Science and Sports, University Medical Center Utrecht, Utrecht, The Netherlands
- 2Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht, The Netherlands
- 3Dept of Primary and Community Care, Radboud University Medical Center, Nijmegen, The Netherlands
- 4Respiratory Epidemiology and Clinical Research Unit, Dept of Medicine, McGill University Health Center, McGill University, Montreal, Canada
- 5Dept of Respiratory Medicine, Glasgow Royal Infirmary, Glasgow, UK
- 6Veterans Administration Portland Health Care System and Oregon Health & Science University, Portland, OR, USA
- 7Dept of Respiratory Medicine, Repatriation General Hospital, Adelaide, Australia
- 8Canterbury District Health Board, Respiratory Services, Christchurch Hospital, Christchurch, New Zealand
- 9Dept of Pulmonary Medicine, Sorlandet Hospital, Kristiansand, Norway
- 10Centre for Research in Environmental Epidemiology (CREAL), Barcelona, Spain
- 11Universitat Pompeu Fabra (UPF), Barcelona, Spain
- 12CIBER Epidemiología y Salud Pública (CIBERESP), Barcelona, Spain
- 13Robertson Centre for Biostatistics, University of Glasgow, Glasgow, UK
- 14Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht, The Netherlands
- 15Dept of Research and Evaluation, Kaiser Permanente Southern California, Pasadena, CA, USA
- 16Dept of Research Methodology, Measurement and Data Analysis, University of Twente, Enschede, The Netherlands
- 17Department of Clinical Epidemiology, Medisch Spectrum Twente, Enschede, The Netherlands
- 18Division of Pulmonary, Allergy, Critical Care and Sleep Medicine, Minneapolis Veterans Affairs Health Care Service and University of Minnesota, Minneapolis, USA
- 19Centre for Primary Care and Public Health, Queen Mary University of London, London, UK
- 20Dept of Rehabilitation Sciences, Catholic University of Leuven, Leuven, Belgium
- 21School of Public Health and Community Medicine, UNSW Australia, Sydney, Australia
- Nini H. Jonkman, Department of Rehabilitation, Nursing Science & Sports, HP W01.121, University Medical Center Utrecht, Heidelberglaan 100, 3508 GA, Utrecht, The Netherlands. E-mail: n.jonkman{at}umcutrecht.nl
Abstract
It is unknown whether heterogeneity in effects of self-management interventions in patients with chronic obstructive pulmonary disease (COPD) can be explained by differences in programme characteristics. This study aimed to identify which characteristics of COPD self-management interventions are most effective.
Systematic search in electronic databases identified randomised trials on self-management interventions conducted between 1985 and 2013. Individual patient data were requested for meta-analysis by generalised mixed effects models.
14 randomised trials were included (67% of eligible), representing 3282 patients (75% of eligible). Univariable analyses showed favourable effects on some outcomes for more planned contacts and longer duration of interventions, interventions with peer contact, without log keeping, without problem solving, and without support allocation. After adjusting for other programme characteristics in multivariable analyses, only the effects of duration on all-cause hospitalisation remained. Each month increase in intervention duration reduced risk of all-cause hospitalisation (time to event hazard ratios 0.98, 95% CI 0.97–0.99; risk ratio (RR) after 6 months follow-up 0.96, 95% CI 0.92–0.99; RR after 12 months follow-up 0.98, 95% CI 0.96–1.00).
Our results showed that longer duration of self-management interventions conferred a reduction in all-cause hospitalisations in COPD patients. Other characteristics are not consistently associated with differential effects of self-management interventions across clinically relevant outcomes.
Abstract
Increasing duration of self-management interventions reduces risk of all-cause hospitalisations in patients with COPD http://ow.ly/YVw9E
Introduction
Chronic obstructive pulmonary disease (COPD) is a serious health problem, as it is one of the major causes of death worldwide [1] and negatively impacts patients' health status [2]. To counteract deterioration, patients with COPD are encouraged to adjust their lifestyle, monitor signs and symptoms, and adhere to complex medication regimes [2]. Interventions to improve these self-management behaviours have received considerable attention over recent years [3], as randomised trials showed beneficial effects on various outcomes, including health-related quality of life (HRQoL), dyspnoea, and healthcare utilisation [4]. However, new questions regarding the effectiveness of self-management interventions have emerged, since several recent randomised trials have shown inconclusive results [5, 6], or even deleterious effects [7].
The heterogeneous results of available trials can at least partly be attributed to the diversity of self-management interventions being evaluated. Although most self-management interventions involve an action plan to stimulate patients to anticipate on exacerbations [4] and several interventions [5–9] are based on the programme “Living Well with COPD” [8], the actual interventions vary widely in terms of intensity, duration, delivery, and content. Knowledge of which programme characteristics constitute the effective ingredients of self-management interventions might lead to the optimum design of this type of intervention.
A meta-analysis comparing the effectiveness of different self-management interventions could be a first step to provide evidence on which programme characteristics yield beneficial effects. The most recent Cochrane review on self-management interventions in patients with COPD attempted to identify effective programme characteristics, but this study was largely unrevealing due to little variation in the programme-specific determinants that were analysed [4]. Another recent systematic review on interventions containing self-management support for COPD patients found that from all included multicomponent interventions, those involving structured exercise or enhanced professional care were associated with better outcomes [10]. In this review, interventions with those specific characteristics were compared to usual care. A comprehensive analysis, in which treatment effects of interventions with and without specific characteristics are compared directly, is however needed to enable the identification of effective characteristics of self-management interventions.
An individual patient data (IPD) meta-analysis is the best tool for such an analysis. It enables a uniform statistical analysis and imputation of missing values across studies, while uncertainties (e.g. information on programme characteristics) can be checked with principal investigators [11]. Our IPD meta-analysis aimed to identify programme characteristics of self-management interventions in patients with COPD that affect HRQoL, all-cause and respiratory-related hospitalisation, and mortality.
Methods
Data sources and study selection
This study was conducted as part of a larger project on self-management interventions in patients with different chronic conditions for which the study protocol has been published [12].To identify randomised trials on self-management interventions in patients with COPD, the electronic databases of PubMed, EMBASE, CENTRAL, PsycINFO and CINAHL were searched from January 1985 through until June 2013 (search syntax can be found in table S1 in the online supplementary material). We also searched reference lists of any identified systematic reviews and consulted experts to avoid omission of available trials.
Studies were screened on title/abstract by one researcher (N.H. Jonkman). The full text of potentially eligible studies were retrieved and assessed by two independent researchers (N.H. Jonkman and H. Westland). Any discrepancies were resolved through consensus in presence of a third researcher (J.C.A. Trappenburg). This IPD meta-analysis only included studies on self-management interventions. Given that current views highlight the multifaceted nature of self-management interventions [3, 13], these were defined as interventions providing information to patients and including minimally two of the following components: 1) stimulation of sign/symptom monitoring; 2) education in problem solving skills, i.e. self-treatment of acute exacerbations and stress/symptom management; 3) smoking cessation; and stimulation of 4) medical treatment adherence; 5) physical activity; or 6) improving dietary intake. The general approach for each component had to be on enhancing the patient's active role and responsibility. Therefore, interventions focussing on pulmonary rehabilitation or tele-monitoring devices with passive surveillance were not considered eligible.
Studies were included in the IPD meta-analysis if they: 1) met the definition of self-management intervention above; 2) had a randomised trial design; 3) included patients with an established diagnosis of COPD according to the prevailing guidelines [2]; 4) compared the self-management intervention to usual care or another self-management approach; 5) reported data on one or more of the selected outcomes; 6) followed patients for at least 6 months; and 7) were reported in English, Dutch, French, German, Italian, Portuguese, or Spanish. No additional criteria were applied to exclude individual patients from the IPD meta-analysis.
Methodological quality was assessed by two researchers independently (N.H. Jonkman and H. Westland) using three relevant criteria from the Cochrane “Risk of bias” tool [14]: 1) random concealed treatment allocation; 2) intention-to-treat analysis; and 3) absence of other major sources of bias, e.g. high drop-out and risk of contamination. Discrepancies were solved through consensus with a third researcher (J.C.A. Trappenburg).
Data collection
Principal investigators of selected studies were invited to participate in this IPD meta-analysis and share their de-identified original trial data. A complete list of all requested variables and details on collaboration with principal investigators can be found in the protocol [14]. Data from each trial were checked and questions that arose were discussed and resolved with principal investigators.
Outcomes
To identify effective programme characteristics of self-management interventions across different health outcomes measured at the patient level, this study could only address outcomes collected in a uniform way across trials in COPD patients: HRQoL at 6- and 12-month follow-ups (measured with the Chronic Respiratory Questionnaire [15] or the St. George's Respiratory Questionnaire [16]), all-cause hospitalisation (time to first event, 6 months, and 12 months), respiratory-related hospitalisation (time to first event, 6 months, and 12 months), and mortality (time to event, 6 months, and 12 months).
Programme characteristics
Potential determinants of effective self-management interventions were selected prior to data analysis based on self-management and behaviour change literature and presence of programme characteristics across included studies: 1) Intensity (planned contacts, n) [17], 2) Duration of the intervention (months) [17], 3) Training given to interventionist(s) who delivers intervention to patients (standardised/heterogeneous) [18], 4) Type of interventionist(s) (multidisciplinary team/single interventionist) [19], 5) Contact with peer patients (yes/no) [20]. 6) Self-monitoring through keeping logs (yes/no) [21], 7) Goal-setting skills (yes/no) [20], 8) Problem-solving skills (yes/no) [20], 9) Skills for seeking support in social network or from healthcare professionals (yes/no) [20], 10) Easy telephone access to case manager (yes/no) [22], and 11) Action plan including prescription for emergency treatment (yes/no) [23].
Information on programme characteristics was extracted for intervention and control arms from published manuscripts and trial protocols by two independent researchers (N.H. Jonkman and H. Westland), and checked with the principal investigators of the specific studies.
Data analysis
Data from individual studies were merged to create one database. Missing values were assumed to be missing at random (overall 2.7% missing data, except 33.7% for HRQoL follow-up data). Using multiple imputation by chained equations (25 imputations) [24], missing values for baseline variables and outcomes of individual patients were imputed within studies only. The imputed datasets were used for the primary analysis and the results were pooled using Rubin's rules [25].
All analyses were performed according to the intention-to-treat principle. Studies were analysed using a one-stage approach, i.e. simultaneously analysing all observations while accounting for clustering of observations within studies [26]. The continuous outcomes (HRQoL at 6 and 12 months) were quantified by standardised mean differences (SMD) between intervention and control arms and were analysed using linear mixed effects models. Binary outcome data (all-cause, respiratory-related hospitalisation, and mortality at 6 and 12 months) were analysed with log-binomial mixed effects models, which estimated risk ratios (RRs). All mixed effects models included a random intercept and random slope for the treatment effect per study. For time-to-event endpoints, effects of self-management were quantified by estimating hazard ratios (HRs) using Cox proportional-hazard models including a frailty term per study.
As an intermediary step in the analysis, we estimated the main effects of self-management interventions, i.e. without focusing on specific programme characteristics. Main effects have been reported elsewhere [27], but are presented to enable a comparison of the effects of specific programme characteristics with overall effects of self-management. The primary analysis comprised identification of effective programme characteristics of self-management interventions. Characteristics were evaluated one-by-one in separate analyses. Four trials had multiple intervention arms [5, 28–30], which were included as separate interventions. To identify the effect of intensity and duration of interventions, the aforementioned models were repeated with the covariate for treatment allocation (and random slope) being replaced by either intensity or duration of interventions.
For analysis of binary programme characteristics, studies were grouped according to the presence or absence of the characteristic and regression models were then fitted in both sets of studies separately. Differences between the two estimated effects from the sets of studies were tested on significance of effect modification across trials using a Q-test for heterogeneity [31], which was considered statistically significant if p<0.05. Only statistically significant findings from the primary analysis are presented for a direct comparison across different endpoints.
The univariable approach did not allow adjustment for other programme characteristics, which may introduce confounding by other programme characteristics. For example, interventions including goal-setting skills might have had a longer duration than interventions without goal-setting skills. A multivariable analysis simultaneously estimating the effects of all programme characteristics overcomes this problem. Random slopes for each programme characteristic must be included to preserve the randomisation in individual trials and avoid confounding by patient characteristics. However, the number of included studies (N=14) was too small to perform this analysis. To check for confounding by other programme characteristics in the primary analysis, we performed a secondary analysis using only fixed effect regression models for the multivariable analysis. The regression models included all programme-specific covariates and a dummy variable indicating study. Additionally, the models were adjusted for sex, age, and forced expiratory volume in 1 s (FEV1) as a percentage of predicted of individual patients to adjust for baseline differences. Effect sizes and 95% confidence interval were estimated to compare these with observed effects from the primary analysis.
Several sensitivity analyses were performed to assess robustness of findings from the primary univariable analysis. Main effects were pooled with published main effects of eligible studies that could not provide original data to assess the impact of missing those studies. A complete-case analysis was performed to assess the impact of imputing data and the analyses were repeated by excluding the largest trial [9]. All analyses were performed in R for Windows version 3.1.1 (R Foundation for Statistical Computing, R Development Core Team, Vienna, Austria).
Results
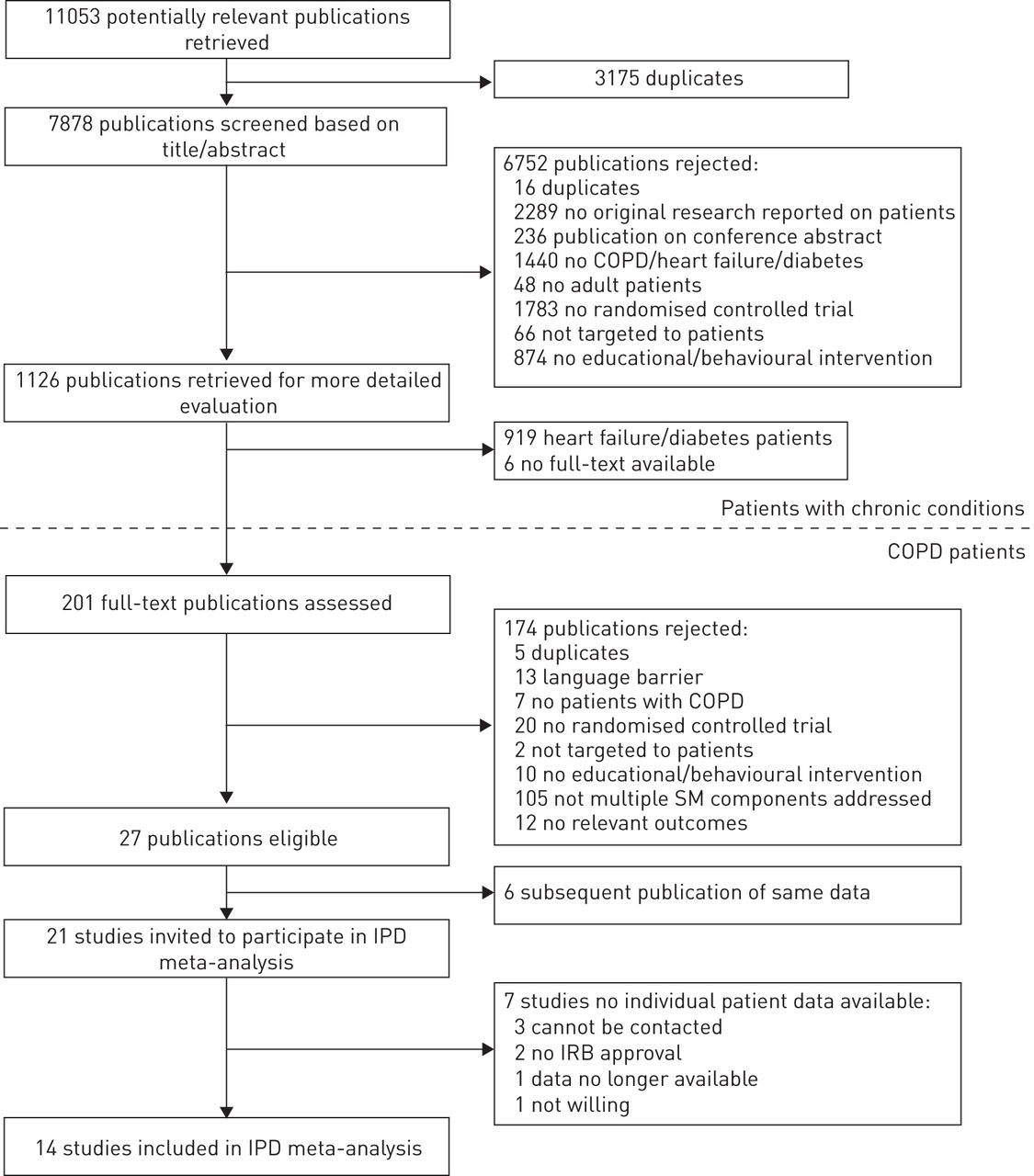
21 studies met the inclusion criteria and principle investigators were approached to participate in this IPD meta-analysis (figure 1). 14 principal investigators responded positively and shared their non-identifiable trial data. Investigators of three studies could not be contacted, for two studies no approval from the local Institutional Review Board was given, the investigators of one study were not willing to participate, and data from another study were no longer available. Patients, programmes, and outcomes of eligible studies that could not provide original data were comparable to those of included studies (tables S2–S4).

{kind=link}
Flowchart of study selection for individual patient data meta-analysis. The present study was conducted as part of a larger project including patients with other chronic conditions (i.e. patients with heart failure or type 2 diabetes mellitus). COPD: chronic obstructive pulmonary disease; SM: self-management; IPD: individual patient data; IRB: institutional review board.
Baseline characteristics of 3282 included patients (75% of eligible patients) are presented in table 1. The majority of the patients were male (65.6%). Patients had a mean±sd age of 68.1±9.6 years and FEV1 of 18.9±47.7 % pred. Only dyspnoea classification showed an imbalance between intervention arms, with 62.6% of the control patients classified as experiencing a high level of breathlessness at baseline compared to 49.8% of the intervention patients.
Baseline characteristics of chronic obstructive pulmonary disease patients in control and self-management intervention arm included in the individual patient data meta-analysis
Description of studies and interventions
Included studies have been reported previously and are presented in table 2. Studies were conducted between 1994 and 2008 in the Netherlands [5, 29, 36, 38], USA [9, 28, 30], UK [6, 37], Australia [39], Canada [8], New Zealand [35], Norway [34], and Belgium/Spain [33]. Most studies recruited clinically stable patients, experiencing at least one exacerbation in the previous year. Sample size ranged from 53 [34] to 743 patients [9]. Overall, methodological quality was good with few indications of high risk of bias (table S5). Interventions consisted on average of 10.5 planned contacts with healthcare professionals (range 1–35) and lasted on average 9.1 months (range 1 day–24 months). Extracted programme characteristics of each intervention arm are presented in table 3. The majority of interventions (15 out of 19) used a standardised protocol to train interventionists. Eight (42%) interventions included a multidisciplinary team, nine (47%) included peer contact, and in nine (47%) logs were used for symptom monitoring. Goal-setting skills were taught in seven (37%) interventions, problem-solving skills in 10 (53%), and support seeking skills in nine (47%). Patients had telephone access to a case manager in eight (42%) interventions and were given an action plan with prescription for emergency medication in 11 (58%) interventions.
Description of trials on self-management in COPD patients included in the individual patient data meta-analysis
Programme characteristics of the self-management interventions in patients with chronic obstructed pulmonary disease included in the individual patient data meta-analysis
Primary analysis programme characteristics
No single programme characteristic was effective on all outcomes considered, but several characteristics showed an effect on one or more outcomes (table 4). The intensity of interventions showed a risk reduction of all-cause hospitalisation for each increasing contact (time to first event HR 0.99, 95% CI 0.98–1.00; at 6 months RR 0.98, 95% CI 0.96–1.00; and at 12 months RR 0.98, 95% CI 0.97–1.00). Similarly, each increasing month of duration of intervention reduced the risk of all-cause hospitalisation (time to first event HR 0.98, 95% CI 0.97–0.99; at 6 months RR 0.96, 95% CI 0.92–0.99 and at 12 months RR 0.98, 95% CI 0.96–1.00). Interventions with peer contact reduced risk of respiratory-related hospitalisation at 6 months (RR 0.64, 95% CI 0.45–0.92), while there was no effect in the interventions without peer contact (RR 1.02, 95% CI 0.76–1.38; interaction p=0.049). The interventions using logs for symptom monitoring, irrespective of an action plan, showed no effect on time to first respiratory-related hospitalisation (HR 0.99, 95% CI 0.77–1.28), while the interventions not using logs showed a risk reduction (HR 0.64, 95% CI 0.50–0.82; interaction p=0.015). In the analyses of mortality (time to death), all interventions teaching problem-solving skills also taught support seeking skills, resulting in similar subsets of studies. Those interventions showed a (nonsignificant) increased risk of death (HR 1.39, 95% CI 0.91–2.11), which was not present in the interventions without those characteristics (HR 0.73, 95% CI 0.48–1.11; interaction p=0.033).
Primary analysis of effects of self-management interventions and characteristics in patients with chronic obstructive pulmonary disease included in the individual patient data meta-analysis
Secondary analysis and sensitivity analysis
The secondary multivariable analysis confirmed the reduced risks of all-cause hospitalisation with increasing duration of intervention (table 5), but the reduced risk for increased intervention intensity on all-cause hospitalisation disappeared when correcting for other programme characteristics (time to first event HR 1.08, 95% CI 1.02–1.14; at 6 months RR 1.26, 95% CI 0.57–2.80; and at 12 months: RR 1.00, 95% CI 0.61–1.64). The increased risk of time to first respiratory-related hospitalisation for interventions including log keeping compared to those without log keeping in the primary analysis was not confirmed either as this became protective (HR 0.47, 95% CI 0.26–0.83). Due to the low number of cases of respiratory-related hospitalisation at 6-month follow-up and time to death, those multivariable models were over-fitted and effects could not be estimated reliably. The sensitivity analyses showed effects in similar direction compared to the primary analysis (not reported).
Secondary analysis of effects of programme characteristics in patients with chronic obstructive pulmonary disease included in the individual patient data meta-analysis adjusted for other characteristics
Discussion
Self-management interventions in patients with COPD have shown positive overall effects on HRQoL, all-cause and respiratory-related hospitalisations, but there is considerable heterogeneity in outcomes [4]. To our knowledge, this is the first study using individual patient data aiming at identifying effective programme characteristics of self-management interventions for patients with COPD. The only consistent association observed was a favourable effect of longer duration of interventions on all-cause hospitalisation; for each increasing month of the intervention there was a 2% risk reduction on time to first event, 4% risk reduction on 6-month hospitalisation, and 2% risk reduction on 12-month hospitalisation. Effects observed in univariable analysis for intensity of interventions, peer contact, log keeping, and problem-solving/support allocation could not be confirmed when corrected for other programme characteristics.
The association between self-management programme characteristics and outcomes in patients with COPD have been evaluated previously in two reviews, but both used summary data across included trials instead of data at the level of individual patients [4, 10]. One review pooled data from 174 trials that included a self-management component [10]. Multicomponent interventions and those with structured exercise or enhanced professional care did better when compared to usual care [10]. The results of this review are not comparable with our results, since the authors applied rather wide inclusion criteria and the study selection contained many pulmonary rehabilitation interventions with (very) limited self-management components. The authors of the other review pre-specified different programme characteristics for their analysis, including duration of follow-up ≥12 months [4]. Due to limited variation across the 23 included trials, no analyses could be undertaken on this characteristic [4] and the other analyses were largely unrevealing. Considering their findings, we chose to analyse the duration of interventions continuously, which revealed small favourable effects on all-cause hospitalisation. The beneficial effect of longer-lasting interventions may extend beyond the COPD population, since there is evidence that longer duration of behavioural interventions is associated with maintenance of behaviour change in the general population [40] and better clinical outcomes in patients with heart failure [41].
Longer-lasting interventions in our selection of studies generally consisted of an intensive start, followed by regular contacts with the patient over a defined period of time. This may have provided more opportunities to prompt and discuss feedback regarding patients' behaviour. Although our results suggest that longer-lasting self-management strategies should be recommended for clinical practice rather than brief interventions, we still lack knowledge on the minimum required duration or dosing and associated costs. Recently published 2-year follow-up data from one of the trials included in our study [29] demonstrated a fading out of the 1-year effect on exercise capacity while the effect on activity level was maintained [42]. This implies that self-management interventions suffer from at least some attrition of treatment effects once the intervention is terminated and that sustained contact with patients is needed.
Our findings might also indicate that the observed effects of self-management interventions are strongly attributable to regular professional review and less to content. A study on self-management support in diabetes care showed that contacts of professionals with patients mainly improved biomedical monitoring instead of self-management behaviours [43]. Those findings support prior research revealing the difficulties professionals experience with implementing self-management interventions in practice [44, 45]. This emphasises that we should pay considerable attention to supporting professionals to change their own behaviour in approaching patients, to ensure that patients receive the self-management intervention as intended. Self-management interventions take time and continuous support to achieve better patient outcomes.
This IPD meta-analysis was the first study using original trial data of 3282 patients to identify effective characteristics of self-management interventions. This enabled a uniform statistical analysis and close collaboration with principal investigators ensured correct labelling of programme characteristics. Although we performed careful data collection and analysis, we only revealed a clear association for duration of interventions with all-cause hospitalisation. Several programme characteristics that seemed to modify the effect in the univariable analysis, disappeared as effect modifiers after adjustment for co-occurrence of other programme characteristics in multivariable models. Therefore, the counterintuitive negative effects observed in univariable analysis for log keeping, problem-solving skills, and support seeking skills may be attributable to another common characteristic of those studies. Potential explanations for not finding other pronounced effective programme characteristics might be related to methodological limitations of conducting an IPD meta-analysis on multicomponent self-management interventions. First, although individual patient data were used, programme characteristics were analysed on the level of complete studies, like a classic meta-analysis. The low number of included studies (N=14) limited the possibility of analysing programme characteristics in a multivariable mixed effects model and interpreting findings causally. However, we applied a secondary fixed effect analysis to assess whether univariable effects could be confirmed after adjustment.
Another explanation may be that some of the included studies actually failed to intervene, i.e. the intervention was not properly implemented or was not delivered to all the intervention patients. Data on the actual delivery of the intervention by the interventionist (fidelity of intervention delivery) and the adherence to the intervention by patients were requested but not collected by authors in a majority of the trials. Therefore, an additional on-treatment analysis to assess whether these phenomena played a role could not be performed. Insight into the delivery and uptake of self-management interventions through (mixed method) process evaluations alongside trials is essential as this can increase our understanding of how different programme characteristics contribute [46].
Third, the analysis required a simplification of the different programme characteristics through categorisation. This may have created large, still heterogeneous groups of studies being compared (i.e. peer contact in one study may have differed from that in another study), a problem more often encountered in meta-regression analyses [47]. Detailed, uniform reporting of different programme characteristics of interventions in future trials may facilitate a better comparison of interventions, for example, through the use of existing taxonomies [48].
Fourth, the analyses were not adjusted for differences in the control groups across studies since these differed on too many aspects (e.g. setting, country, and year of inclusion). Studies were performed in various countries over a time frame of 14 years, which may have introduced additional variability [49]. It is possible that programme characteristics may be particularly effective in a specific healthcare context. It is also likely that some programme characteristics are only effective in subgroups of patients instead of the entire study population. Future research should address the hypothesis that subgroups of patients might respond differently to specific self-management interventions. Behaviour change evolves over time, with different patterns and timelines for different people. This knowledge can further guide the development of tailored self-management approaches.
Finally, according to self-management [20] and behaviour change literature [21], we focused in our analyses on clinically relevant programme characteristics related to mode, dose, and techniques for delivery of the self-management interventions. Although we analysed a rather large selection of potential determinants, this selection was limited to characteristics that varied between studies and it is possible that we have missed critical characteristics. Nevertheless, we performed multiple analyses, which increased the risk of false-positive findings, so the findings should be interpreted with caution.
Conclusion
Duration of self-management interventions is the only programme characteristic that could be identified in this IPD meta-analysis to modify the effect of self-management interventions in patients with COPD, increasing duration was associated with reductions in all-cause hospitalisations. This suggests that longer-lasting self-management strategies are recommended for clinical practice rather than brief interventions. This study further highlights the need for process evaluations alongside randomised trials, with special attention for monitoring intervention delivery.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Conflict of interests: Disclosures can be found alongside the online version of this article at erj.ersjournals.com
- Received November 9, 2015.
- Accepted February 16, 2016.
- Copyright ©ERS 2016