



Change in blood eosinophils following treatment with inhaled corticosteroids may predict long-term clinical response in COPD
- Alexander G. Mathioudakis1,2,
- Andras Bikov1,2,
- Philip Foden3,
- Lies Lahousse4,
- Guy Brusselle5,6,
- Dave Singh1,2,7 and
- Jørgen Vestbo1,2
- 1Division of Infection, Immunity and Respiratory Medicine, School of Biological Sciences, The University of Manchester, Manchester, UK
- 2North West Lung Centre, Wythenshawe Hospital, Manchester University NHS Foundation Trust, Manchester Academic Health Science Centre, Manchester, UK
- 3Dept of Medical Statistics, Wythenshawe Hospital, Manchester University NHS Foundation Trust, Manchester, UK
- 4Dept of Bioanalysis, Ghent University, Ghent, Belgium
- 5Depts of Epidemiology and Respiratory Medicine, Erasmus Medical Center, Rotterdam, the Netherlands
- 6Dept of Respiratory Medicine, Ghent University Hospital, Ghent, Belgium
- 7Medicines Evaluation Unit, Manchester, UK
- Jørgen Vestbo, Division of Infection, Immunity and Respiratory Medicine, The University of Manchester, Southmoor Road, M23 9LT, Manchester, UK. E-mail: jorgen.vestbo{at}manchester.ac.uk
Abstract
There is an emerging role for blood eosinophil count (EOS) as a biomarker to guide inhaled corticosteroid (ICS) therapy in COPD. Since ICS administration could influence EOS, we hypothesised that change in EOS following treatment with ICS may predict outcomes of long-term therapy.
In a post hoc analysis of ISOLDE, a 3-year, double-blind trial comparing 500 µg fluticasone propionate twice daily with placebo in 751 patients with moderate-to-severe COPD, we evaluated whether the initial changes in EOS during ICS treatment were predictive of ICS treatment response.
EOS change within 1 year after the introduction of ICS was strongly predictive of treatment response. A suppressed EOS was associated with treatment effect. Characteristically, in patients with EOS suppression of ≥200 cells·μL−1, ICS use was associated with a decelerated rate of decline of forced expiratory volume in 1 s (FEV1), by 32 mL·year−1, and a 30% reduction in the exacerbation rate. In contrast, in patients experiencing an increase in EOS of ≥200 cells·μL−1, ICS use was associated with an accelerated rate of decline of FEV1, by 37 mL·year−1 and an 80% increase in the exacerbation rate (p<0.0001). EOS change was not predictive of clinical response with regards to health status evaluated using the St George's Respiratory Questionnaire.
These findings suggest that EOS change after ICS administration may predict clinical response to ICS therapy in patients with moderate-to-severe COPD at risk of exacerbations. ICS administration may be associated with more frequent exacerbations and an accelerated lung function decline in the 20% of patients in whom EOS increases after the administration of ICS. These hypothesis-generating observations will need validation in prospectively designed studies.
The ISOLDE trial was conducted before the ICJME recommended a prospective registration of RCT protocols.
Abstract
Blood eosinophil change in response to ICS may predict long-term response to ICS in COPD. A rise in eosinophils was observed in 20% of participants in ISOLDE and was associated with lack of clinical benefit and a potential risk of harm. http://bit.ly/3bPKLnD
Introduction
COPD, characterised by marked heterogeneity in both clinical manifestations and underlying mechanisms [1, 2], represents a prime target for the introduction of precision medicine interventions. In recent years, clinical studies have evaluated strategies aimed to tailor the administration of inhaled corticosteroids (ICS), which only appear to be effective in a subset of patients with COPD [1, 2]. These studies were actuated by concerns that ICS benefits come at the expense of side-effects that include a significant increase in the risk of pneumonia [3, 4].
It has been suggested that ICS may only be effective in COPD patients with enhanced eosinophilic inflammation in the airways [5, 6]. Blood eosinophil count (EOS) as a biomarker to guide the administration of ICS has been tested in several trials, either in post hoc [7–13] or prespecified [14–17] analyses, which have consistently demonstrated a positive association between blood EOS count and treatment response to ICS. Based on these analyses, the Global Initiative for Chronic Obstructive Lung Disease now recommends the use of EOS to assist with the clinical decision of whether or not to use ICS in patients at risk of exacerbations [18].
However, the association between ICS and EOS may not be that simple. In asthma, eosinophils appear to be a responsive biomarker of therapeutic response to corticosteroids. The administration of either inhaled [19, 20] or systemic [21, 22] corticosteroids leads to a reduction in eosinophil count, which is proportionate to corticosteroid treatment efficacy. This is not unexpected, since blood eosinophil reduction probably reflects a suppression of eosinophilic airway inflammation. In addition, in COPD, it has been demonstrated that both oral [23] and inhaled [24] corticosteroids could significantly suppress sputum eosinophils. Therefore, we hypothesised that ICS administration may influence blood EOS as well and that change in blood EOS following ICS treatment could predict the long-term efficacy of this treatment.
The availability of multiple EOS measurements in the ISOLDE trial dataset allowed us to test this hypothesis. In a post hoc analysis of the ISOLDE trial, we assessed whether EOS change after initiation of ICS could more accurately predict response to ICS than a single measurement of EOS. In addition, we assessed the predictive value of EOS measured either while patients were not receiving any corticosteroids or while they were receiving ICS. The ISOLDE trial compared fluticasone propionate 500 μg twice daily with placebo in 751 patients with moderate-to-severe COPD. The trial included an 8-week run-in period where participants were not receiving ICS. EOS were conveniently measured before at the end of the run-in period and every year thereafter (supplementary figure S1), allowing us to evaluate these EOS biomarkers.
Methods
This retrospective analysis of data from the ISOLDE trial was based on a prospectively designed analysis plan, submitted to GSK via Clinical Study Data Request (www.clinicalstudydatarequest.com), and was peer reviewed by an independent expert review panel.
Overview of the ISOLDE study
The ISOLDE study, a 3-year, double-blind, randomised controlled trial (RCT), compared fluticasone propionate 500 μg twice daily (ICS) versus placebo [25]. Eligible COPD patients were aged 40–75 years, current or former smokers not suffering from asthma, with a post-bronchodilator forced expiratory volume in 1 s (FEV1) of <85% predicted with limited bronchodilator reversibility (a FEV1 response to 400 μg salbutamol of ≤10% pred), and without concurrent severe diseases limiting their life expectancy to <5 years. Enrolled patients underwent an 8-week run-in period, during which ICS were not allowed. After this period, they were randomised to receive either fluticasone propionate 500 μg or placebo twice daily, via a metered dose inhaler with a spacer device for 3 years. After the run-in, but before the double-blind phase, participants received a 2-week course of oral prednisolone, unless it was contraindicated. Patients were followed every 3 months for the duration of the trial. Pulmonary function, exacerbations, health status and adverse events were evaluated at every visit. Blood biomarkers, including EOS, were monitored before and at the end of the run-in period, after the 2-week course of oral prednisolone, and annually thereafter. The primary end-point was the decline (mL·year−1) in FEV1, while other key end-points included exacerbation frequency, changes in health status and withdrawals due to respiratory disease. Details in the design and outcomes of the ISOLDE trial have been reported previously [25].
Predictive value of blood EOS
We evaluated whether 1) change in EOS following initiation of ICS treatment, 2) EOS while patients were not receiving any oral or inhaled corticosteroids or 3) EOS while on ICS could predict response to ICS with regards to pulmonary function, exacerbations and health status.
We captured EOS values measured during the first year of the ISOLDE trial. For EOS while not receiving corticosteroids, we used EOS values measured while patients were not receiving oral or inhaled corticosteroids for ≥8 weeks, prioritising EOS measured at the end of the run-in period. For EOS while on ICS, we used EOS values measured while patients were receiving ICS for ≥8 weeks. We used baseline EOS measurements for patients receiving ICS at baseline, or EOS measured during the first year of treatment, for patients who were randomised to receive ICS. The ISOLDE investigators recorded in detail medications that participants received before and during the study period. These included the study medications (ICS or placebo), during the study period, but also the use of ICS before recruitment and the use of oral corticosteroids before or during the study period. Therefore, we are confident that the selected EOS values satisfy the above criteria. While we accepted EOS values measured during the first year of follow-up for our main analysis, aiming to increase our study sample, we conducted sensitivity analyses where we only used EOS measurements captured at baseline (before and after the run-in period).
We used mixed-effect model repeated measures (MMRM) for analysing the impact of ICS administration on the rate of decline in post-bronchodilator FEV1, focusing on the three-way interaction of treatment, time and EOS (or EOS change) on FEV1. In a sensitivity analysis, we only used FEV1 values measured between the 3rd and 36th months of treatment, to account for the increase that the course of prednisolone and initiation of inhaled treatment conferred to the mean FEV1. Since ICS are currently not indicated as a monotherapy for COPD, in a subgroup analysis we only included participants concurrently receiving a long-acting β2-agonist (LABA), to test whether our results are generalisable to these patients.
For exacerbations, we used a Cox proportional hazards model to explore time-to-first exacerbation and a generalised linear model assuming a negative binomial distribution, with the number of on-treatment moderate and severe exacerbations per patient per year as the response variable. The proportional hazard assumption was assessed based on the Kaplan–Meier curves and the Schoenfeld residuals.
Finally, for health status, we assessed changes in St George's Respiratory Questionnaire (SGRQ) total scores, which range from 0 to 100, with higher scores indicating more limitations [26]. We used MMRM to assess the three-way interaction of treatment, EOS and time on SGRQ.
We considered age, sex, ICS use prior to treatment, smoking status and baseline FEV1 as covariates in all analyses. We only included patients who underwent randomisation and received at least one study drug dose. We only included measurements taken while participants were receiving study treatments. In each analysis, patients who did not have the required EOS measurements (EOS change, EOS while not on corticosteroids or EOS while on ICS) were excluded.
Statistical analyses were performed using R statistical software (version 3.4.3; R Foundation for Statistical Computing, Vienna, Austria).
Results
The design and main results of the ISOLDE trial, which randomised 751 patients to receive either fluticasone propionate (n=376) or placebo (n=375) have been reported previously (figure 1) [25]. In brief, there was no significant between-group difference in the baseline characteristics of the participants. ICS did not affect the annual rate of decline in FEV1, but reduced exacerbations by 25% and improved health status, evaluated by SGRQ.

The ISOLDE trial patient flow diagram. EOS: blood eosinophil count; ICS: inhaled corticosteroids.
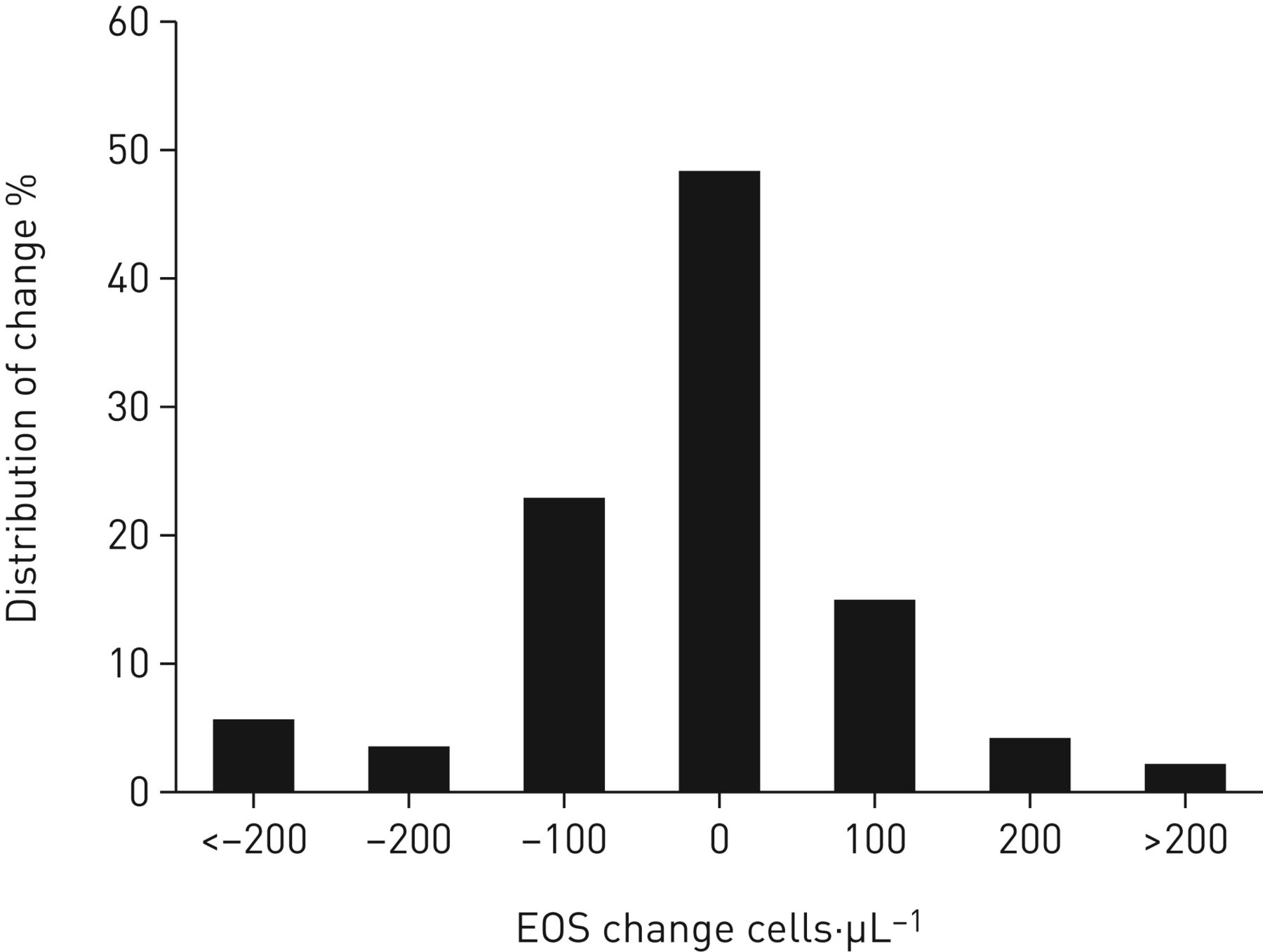
As a result of the analysis plan of this post hoc study, different numbers of patients were available for the different analyses. Details on the number of evaluable participants for each analysis are summarised in table 1. The degree of change in EOS values after the initiation of ICS therapy is summarised in figure 2.
Participants with available data that could be used in each analysis

Distribution of blood eosinophil count (EOS) change in the ISOLDE population after the administration of inhaled corticosteroid therapy. n=392.
Decline in FEV1
Change in EOS following initiation of ICS treatment (suppression or rise) strongly predicted ICS treatment response on post-bronchodilator FEV1 decline as outcome (p<0.0001) (figure 3). Compared to placebo, ICS administration did not appear to have any impact on FEV1 decline rate in cases where EOS remained unchanged. ICS decelerated FEV1 decline in cases of EOS suppression and accelerated FEV1 decline in cases of EOS rise. Characteristically, in patients experiencing an EOS suppression of ≥200 cells·μL−1, ICS administration decelerated the mean annual FEV1 decline by 37 mL·year−1, while in those experiencing EOS rise of ≥200 cells·μL−1, ICS treatment accelerated the mean FEV1 decline by 32 mL·year−1, favouring placebo.
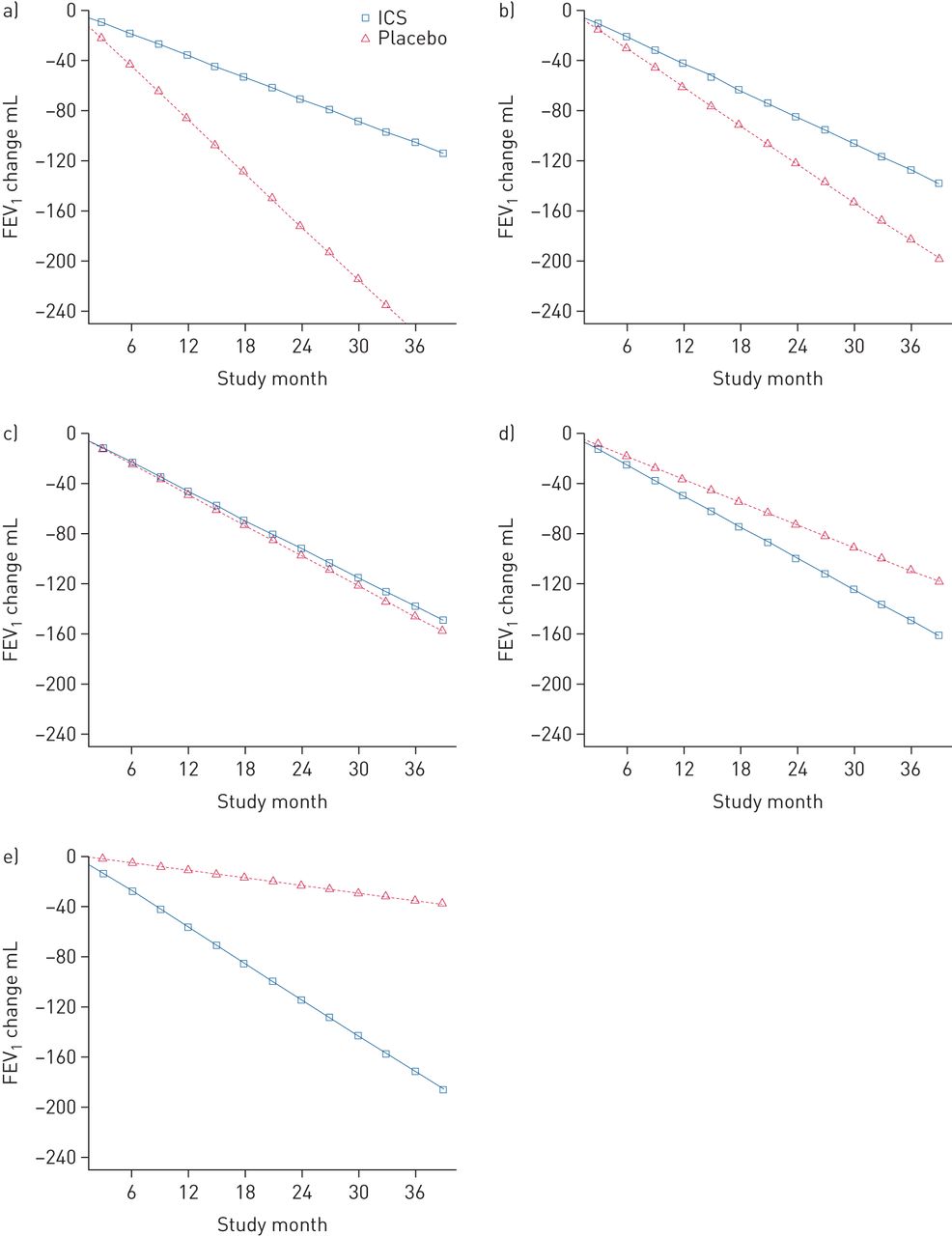
Mean changes from baseline in forced expiratory volume in 1 s (FEV1) in patients receiving fluticasone or placebo according to the change in their blood eosinophil count: a) suppressed by 300 cells·μL−1; b) suppressed by 100 cells·μL−1; c) unchanged; d) raised by 100 cells·μL−1; e) raised by 300 cells·μL−1. Estimates are derived from the mixed-effect model repeated measures model. ICS: inhaled corticosteroids.
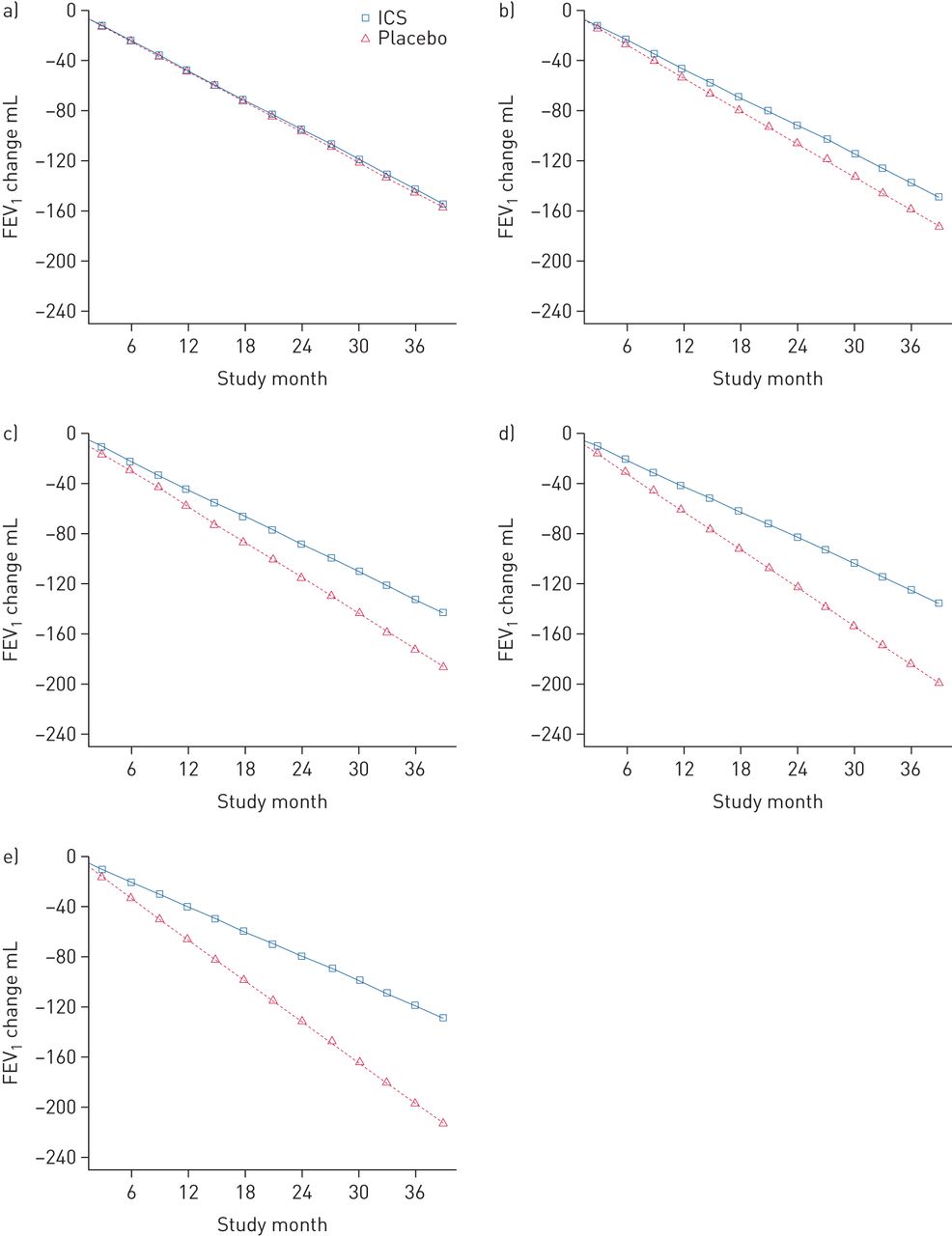
Higher EOS while not on corticosteroids was associated with a significantly greater ICS treatment efficacy (p=0.005) (figure 4). Compared to placebo, ICS decelerated the mean annual rate of post-bronchodilator FEV1 decline by 0, 7, 15, 21 and 28 mL·year−1 for patients with 0, 100, 200, 300 and 400 cells·μL−1, respectively. In contrast, high EOS following initiation of ICS treatment was associated with lower subsequent efficacy of ICS on FEV1 decline. Patients with EOS while on ICS ≥200 cells·μL−1 receiving ICS experienced an accelerated FEV1 decline compared to placebo (p=0.004) (figure 5).

Mean changes from baseline in forced expiratory volume in 1 s (FEV1) in patients receiving fluticasone or placebo according to their blood eosinophil count while not receiving corticosteroids: a) 0 cells·μL−1; b) 100 cells·μL−1; c) 200 cells·μL−1; d) 300 cells·μL−1; e) 400 cells·μL−1. Estimates are derived from the mixed-effect model repeated measures model. ICS: inhaled corticosteroids.

Mean changes from baseline in forced expiratory volume in 1 s (FEV1) in patients receiving fluticasone or placebo according to their blood eosinophil count while on inhaled corticosteroids (ICS): a) 0 cells·μL−1; b) 100 cells·μL−1; c) 200 cells·μL−1; d) 300 cells·μL−1; e) 400 cells·μL−1. Estimates are derived from the mixed-effect model repeated measures model.
These results remained robust in sensitivity analyses where we 1) excluded FEV1 measurements at baseline and up to 3 months after randomisation or 2) only included baseline EOS measurements (supplementary material).
In a subgroup analysis where we evaluated only participants concurrently receiving LABA (n=51, 8.8% of the participants), higher EOS suppression and higher EOS while not receiving ICS were associated with response to ICS (supplementary material).
Exacerbations
Change in EOS following initiation of ICS and EOS while not receiving ICS did not predict response to ICS with regards to time to first exacerbation. EOS while on ICS appeared predictive (p<0.01): hazard ratios (95% CI) for ICS versus placebo were 0.66 (0.39–1.12) and 0.90 (0.73–1.10) for participants with EOS while on ICS ≥200 and <200 cells·μL−1, respectively. Kaplan–Meier curves and the Schoenfeld residuals confirmed that the proportional hazard assumption was met.
In contrast, EOS change was strongly associated with ICS response with regards to exacerbation frequency (p<0.0001). Subjects with EOS suppression of 200 cells·μL−1, unchanged EOS or EOS rise by 200 cells·μL−1 experienced a 33% decrease, no impact and an 80% increase in their exacerbation frequency with ICS compared to placebo, respectively (figure 6). The results remained robust in sensitivity analyses (supplementary material). Neither EOS while not receiving corticosteroids nor EOS while on ICS were predictive of the impact of ICS administration on exacerbation frequency.

Relative risk of exacerbation in patients receiving inhaled corticosteroid versus placebo, by blood eosinophil count (EOS) change. Estimates are derived from the generalised linear model.
Health status
Overall, we observed a progressive decline in subjects' health status over time. This decline was delayed by the administration of ICS among participants with higher EOS while not receiving ICS (p<0.01) (figure 7). Over the duration of the study, ICS limited the mean SGRQ score decline by −0.9, 1.6, 4.5, 6.6 and 9.1 units among subjects with EOS while not receiving ICS of 0, 100, 200, 300 and 400 cells·μL−1, respectively. Neither change in EOS after initiating ICS nor EOS while on ICS predicted treatment efficacy of ICS, with regards to SGRQ. The findings were similar in a sensitivity analysis in which we only included EOS values measured at baseline (supplementary material).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean changes from baseline in St George's Respiratory Questionnaire (SGRQ) score in patients receiving fluticasone or placebo according to their blood eosinophil count while not receiving corticosteroids: a) 0 cells·μL−1; b) 100 cells·μL−1; c) 200 cells·μL−1; d) 300 cells·μL−1; e) 400 cells·μL−1. Estimates are derived from the mixed-effect model repeated measures model. ICS: inhaled corticosteroids.
Discussion
In an exploratory post hoc analysis, we evaluated EOS as a responsive therapeutic biomarker to guide the administration of ICS in COPD. In the ISOLDE population, EOS change (increase or decrease) in response to ICS administration was predictive of clinical response to ICS with regards to FEV1 decline and exacerbation frequency. While the use of EOS to guide ICS administration has been evaluated in post hoc or prespecified analyses of several RCTs [7–17], this is the first study to test EOS change as a therapeutic biomarker.
An increase in EOS after ICS therapy revealed a vulnerable patient group, where treatment with ICS was inferior to placebo. Having a prevalence of 20% within the ISOLDE trial study population, this cluster requires further evaluation. The decreased therapeutic index of ICS in this group could be explained by the fact that these patients who do not gain any benefit from ICS still bear their immunosuppressive burden. As a result, they are at higher risk of recurrent acute respiratory infections, such as infective exacerbations of their COPD or pneumonias, which result in accelerated FEV1 decline. The mechanism leading to EOS increase in response to ICS is unclear.
A differential treatment response to ICS among patients with COPD has been shown in studies evaluating clinical outcomes [7–17], but also in a subanalysis of the GLUCOLD study evaluating the impact of ICS on airway gene expression [27]. Airway genes that were consistently upregulated or downregulated after the initiation of ICS (or ICS+LABA) versus placebo in steroid-naïve patients were identified. In addition, responders identified through the impact of ICS on their genes had a better clinical response with regards to FEV1 and SGRQ at 30 months, but this does not automatically imply an effect mediated through eosinophils.
In the ISOLDE trial, EOS as a biomarker to guide ICS administration has been tested previously in a post hoc analysis by Barnes et al. [8]. They used EOS measured at the end of the run-in period, while patients were not receiving ICS. However, they did not exclude a significant proportion of the participants who developed exacerbations during the run-in period and received oral corticosteroids, which are known to suppress EOS. Inclusion of these participants, whose EOS were suppressed because of the administration of oral corticosteroids, could have introduced confounding. Here, using detailed prescription data, which were available for all participants before and during the ISOLDE study, we captured EOS measurements while patients were not receiving any corticosteroids for ≥8 weeks and while they were receiving ICS for ≥8 weeks. In our analysis, only higher EOS measured while patients were not receiving any corticosteroids (and not EOS while on ICS) could predict clinical response to ICS with regards to pulmonary function and health status. This is the first study to test the impact of ICS administration on the ability of EOS to predict ICS response.
ISOLDE was the first large trial to evaluate exacerbations as a secondary outcome. At the time, standardisation in the definition and severity grading was lacking. Additionally, the methodology used to capture exacerbations in the ISOLDE trial might have been suboptimal. More importantly, exacerbation history prior to recruitment was not used as an inclusion criterion and was not documented. As a result, the study population was heterogeneous in terms of exacerbations history, probably reducing statistical power on this outcome. Despite these limitations, stratification of the participants by decrease versus rise in EOS in response to ICS administration was revealing. ICS administration resulted in an 80% increase in the frequency of exacerbations in patients with an EOS rise of 200 cells·μL−1 and in a 33% decrease in those with an EOS suppression of −200 cells·μL−1.
In contrast to the majority of the newer trials, ISOLDE was not enriched in exacerbations. Fewer than half of the participants experienced an exacerbation during the first year of the study. This may be the cause of our inconsistent results regarding different effects on exacerbations and health status. In subsequent clinical trials, which have all been enriched by exacerbating patients, there seems to be a clearer link between reduction of exacerbations and improvement in health status.
Blood eosinophil depletion following therapy with the interleukin-5 receptor antagonsists mepolizumab and benralizumab was not associated with treatment response to these medications. However, the impact of interleukin-5 receptor antagonists versus ICS on blood eosinophils differ mechanistically, as does their impact on other inflammatory cascades. This may be the cause of the difference in the clinical results. We use EOS change as a therapeutic biomarker and we do not suggest that there is a direct immunopathological link between EOS levels and COPD symptoms or prognosis.
This hypothesis-generating study has important limitations and our findings will need to be prospectively validated in future randomised controlled trials. Firstly, this was a retrospective post hoc analysis and therefore exploratory in nature. More importantly, whereas high-dose fluticasone propionate was used in the ISOLDE trial, low-to-medium dose ICS are currently recommended for patients experiencing exacerbations despite treatment with long-acting bronchodilator(s) [1]; however, none of the ISOLDE participants were receiving a long-acting muscarinic antagonist (LAMA), and only 51 evaluable subjects received a LABA for ≥6 months. Even though our findings remained robust in a subgroup analysis of subjects concurrently receiving LABA, our findings need to be tested in populations already receiving dual long-acting bronchodilator therapy. In addition, most participants in the ISOLDE trial received a 2-week course of oral corticosteroids after randomisation, which is no longer used in usual care. To minimise the impact that this course of corticosteroids may have had on our findings, we conducted a sensitivity analysis where we excluded FEV1 measurements during the first 3 months from recruitment (including baseline values). Our results were proved robust to this analysis.
Additionally, there were limitations with regards to the availability of data on blood eosinophils. EOS measurements while patients were, or were not receiving corticosteroids were not specifically sought by the ISOLDE investigators and were not available for all participants. As a result, some subjects were excluded from the analyses due to missing data. We report the number of eligible participants included in each analysis and the study samples supporting our main findings range between 334 and 672 subjects. In addition, EOS while on ICS was measured 1 year after start of treatment with ICS versus placebo in some participants. Therefore, in the ISOLDE population, suppression of EOS by ICS could only be determined after 1 year of treatment. This is not optimal for predicting therapeutic response in clinical practice, but more frequent measurements were not available for all participants. In a sensitivity analysis where we only included baseline EOS measurements (before and after the run-in period), EOS values measured 6 weeks apart were used to estimate EOS change (supplementary material). Results of this analysis were consistent with the main analysis, suggesting that EOS measurements over a shorter period might be used in clinical practice, subsequent to validation of our findings.
Our findings are also limited by the fact that EOS values were recorded as multiples of 100 cells·mL−1, which is less accurate than other studies.
Major strengths of our study include the strict design of the ISOLDE trial and our statistical methodology. The ISOLDE trial compared ICS versus placebo using a double-blind, double-dummy design, while most other trials evaluated an ICS/LABA combination versus a LAMA or LABA+LAMA combination. Moreover, the 3-year duration of the ISOLDE trial provided longitudinal data required for evaluating lung function decline.
In conclusion, our study suggests that the relationship between EOS and the administration of ICS may be more complex than it has been anticipated until now. EOS change after ICS therapy may predict long-term clinical response in COPD. In addition, our findings indicate that in the interpretation of EOS values, clinicians may need to take into consideration whether patients were receiving ICS at the time of EOS measurement. However, in view of the limitations of the ISOLDE's trial design, our findings cannot be generalised until further data from prospective studies become available, hopefully from studies recruited from usual clinical practice.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary_material ERJ-02119-2019_supplementary_material
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-02119-2019.Shareable
Acknowledgement
The authors are grateful to the ISOLDE investigators and participants, and to GlaxoSmithKline and Clinical Study Data Request (CSDR, a consortium of clinical study sponsors and funders that was developed to facilitate patient level data sharing, ClinicalStudyDataRequest.com) for providing access to patient level data from the ISOLDE trial.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Author contributions: A.G. Mathioudakis and J. Vestbo contributed to the conception and design of the study. A.G. Mathioudakis conducted data analysis and drafted the manuscript with input from all authors. P. Foden provided statistical expertise. All authors contributed to data interpretation, discussion and critical revision of the paper for intellectual content.
Data availability: Data ownership lies with GlaxoSmithKline. Data sharing is possible via Clinical Study Data Request platform (www.clinicalstudydatarequest.com), after submission of a research proposal, which is reviewed by an independent research panel.
Conflict of interest: A.G. Mathioudakis reports grants from Boehringer Ingelheim, personal fees from Boehringer Ingelheim, personal fees from GlaxoSmithKline, outside the submitted work.
Conflict of interest: A. Bikov has nothing to disclose.
Conflict of interest: P. Foden has nothing to disclose.
Conflict of interest: L. Lahousse reports grants from AstraZeneca, grants from Chiesi, personal fees from Boehringer Ingelheim, personal fees from Novartis, outside the submitted work.
Conflict of interest: G. Brusselle reports personal fees from AstraZeneca, personal fees from Boehringer Ingelheim, personal fees from Chiesi, personal fees from GlaxoSmithKline, personal fees from Novartis, personal fees from Teva, personal fees from Sanofi, outside the submitted work.
Conflict of interest: D. Singh reports grants and personal fees from AstraZeneca, grants and personal fees from Boehringer Ingelheim, grants and personal fees from Chiesi, personal fees from Cipla, personal fees from Genentech, grants and personal fees from GlaxoSmithKline, grants and personal fees from Glenmark, grants and personal fees from Menarini, grants and personal fees from Mundipharma, grants and personal fees from Novartis, personal fees from Peptinnovate, grants and personal fees from Pfizer, grants and personal fees from Pulmatrix, grants and personal fees from Therevance, grants and personal fees from Verona, outside the submitted work.
Conflict of interest: J. Vestbo reports personal fees from Chiesi Pharmaceuticals, personal fees from Boehringer-Ingelheim, personal fees from Novartis, personal fees from AstraZeneca, outside the submitted work.
Support statement: A.G. Mathioudakis is supported by an Academic Clinical Fellowship in Respiratory Medicine from the National Institute for Health Research (NIHR, UK). A.G. Mathioudakis, D. Singh, A. Bikov and J. Vestbo are supported by the National Institute of Health Research Manchester Biomedical Research Centre (NIHR Manchester BRC). Funding information for this article has been deposited with the Crossref Funder Registry.
- Received June 30, 2019.
- Accepted February 17, 2020.
- Copyright ©ERS 2020