



Blood eosinophil count in the general population: typical values and potential confounders
- Sylvia Hartl1,2⇑,
- Marie-Kathrin Breyer3,
- Otto C. Burghuber2,3,
- Alina Ofenheimer2,
- Andrea Schrott1,
- Matthias H. Urban3,
- Alvar Agusti4,
- Michael Studnicka5,
- Emiel F.M. Wouters6 and
- Robab Breyer-Kohansal1
- 1Second Dept of Respiratory and Critical Care Medicine and Ludwig Boltzmann Institute for COPD and Respiratory Epidemiology, Otto Wagner Hospital, Vienna, Austria
- 2Sigmund Freud Medical University, Vienna, Austria
- 3First Dept of Respiratory Medicine and Ludwig Boltzmann Institute for COPD and Respiratory Epidemiology, Otto Wagner Hospital, Vienna, Austria
- 4Respiratory Institute, Hospital Clinic, IDIBAPS, University of Barcelona and National Spanish Network for Respiratory Research (CIBERES), Barcelona, Spain
- 5Dept of Respiratory Medicine, Paracelsus Medical University, Salzburg, Austria
- 6Dept of Respiratory Medicine, MUMC, Maastricht University, Maastricht, The Netherlands
- Sylvia Hartl, Second Dept for Respiratory and Critical Care Medicine and Ludwig Boltzmann, Institute for COPD and Respiratory Epidemiology Otto Wagner Hospital, Sanatoriumstrasse 2, 1140 Vienna, Austria. E-mail: hartlsylvia{at}icloud.com
Abstract
There is growing interest in blood eosinophil counts in the management of chronic respiratory conditions such as asthma and chronic obstructive pulmonary disease (COPD). Despite this, typical blood eosinophil levels in the general population, and the impact of potential confounders on these levels have not been clearly defined.
We measured blood eosinophil counts in a random sample of 11 042 subjects recruited from the general population in Austria. We then: 1) identified factors associated with high blood eosinophil counts (>75th percentile); and 2) excluded subjects with these factors to estimate median blood eosinophil counts in a “healthy” sub-population (n=3641).
We found that: 1) in the entire cohort, age ≤18 years (OR 2.41), asthma (OR 2.05), current smoking (OR 1.72), positive skin prick test (OR 1.64), COPD (OR 1.56), metabolic syndrome (OR 1.41), male sex (OR 1.36) and obesity (OR 1.16) were significantly (p<0.05) associated with high blood eosinophil counts (binary multivariable logistic regression analysis), and had an additive effect; and 2) after excluding these factors, in those older than 18 years, blood eosinophil counts were higher in males than in females (median 120 (5%–95% CI: 30–330) versus 100 (30–310) cells·µL−1, respectively) and did not change with age.
Median blood eosinophil counts in adults are considerably lower than those currently regarded as normal, do not change with age beyond puberty, but are significantly influenced by a variety of factors which have an additive effect. These observations will contribute to the interpretation of blood eosinophil levels in clinical practice.
Abstract
The level of circulating blood eosinophils in healthy subjects is much lower than currently considered, is age dependent until 18 years, is higher in males and is influenced by several multimorbid conditions and lifestyle factors http://bit.ly/37W7EDd
Introduction
The Global Initiative for Asthma (GINA) recommends the use of blood eosinophil counts to identify patients with type II inflammation, and to target the use of biologics for the management of severe asthma [1]. Type II inflammation is mainly triggered by allergy, and causes 50% of asthma manifestations [2–4]. Moreover, excluding persons with allergic sensitisation measured by positive skin prick test reduced the overall average blood eosinophil count in an early study by Felarca and Lowell [5], underlining the important relationship between allergy and blood eosinophils.
More recently, the Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Lung Disease (GOLD) recommends the use of circulating eosinophils to guide therapy with inhaled corticosteroids (ICS) in patients with stable chronic obstructive pulmonary disease (COPD) who continue to exacerbate despite appropriate bronchodilator therapy [6, 7]. According to GOLD, a blood eosinophil count threshold of 300 cells·µL−1 can be used to identify patients that are most likely to benefit from treatment with ICS [6]. The blood eosinophil thresholds that these documents use are often criticised because they are believed to be within the normal eosinophil range [5, 8]. However, the typical range of blood eosinophil counts in the general population is not well established, since the role of potential confounding factors other than atopy [2, 5], such as age, sex, environmental exposures [3, 9, 10] or presence of disease [4, 11–15] is unclear.
To address these gaps, we measured blood eosinophil counts in a large (n=11 423), representative and carefully characterised cohort of individuals living in Austria, who were recruited from the general population and stratified by age, sex and residential area (urban/rural). In these individuals, we aimed to: 1) identify factors associated with high blood eosinophil counts (which we a priori defined as >75th percentile); and 2) estimated blood eosinophil counts in a “healthy” sub-population that excluded the identified confounders.
Methods
Study design
The LEAD (Lung, hEart, sociAl, boDy) study (ClinicalTrials.gov; NCT01727518) is a longitudinal, observational, population-based Austrian cohort, the design and methodological details of which have been published elsewhere [16]. Briefly, LEAD aims to investigate the impact of genetic, environmental, social, developmental and ageing factors on respiratory health and associated comorbidities through life. Between 2011 and 2016, LEAD recruited 11 423 participants, aged 6 to 82 years, who will be followed-up every 4 years. The cross-sectional data gathered at recruitment was used for the current analysis. The Vienna Ethics Committee approved the study (EK-11-117-0711). All participants signed informed consent; for children below the age of 18 years, informed consent was signed by their parents or legal representative.
Measurements
The methods used in LEAD have been detailed elsewhere [16]. In brief, the following measurements were obtained in all participants at recruitment: 1) demographics (age, sex, height, weight, and body mass index (BMI)); 2) smoking status (never, former, current), with cumulative smoking exposure obtained by questionnaire (heavy smoking was defined as ≥20 pack-years); 3) blood pressure and electrocardiogram; 4) skin prick test; 5) forced spirometry, conducted according to international standards [17–19], with the diagnosis of asthma established following GINA recommendations and that of COPD on the basis of a post-bronchodilator forced expiratory volume in 1 s to forced vital capacity ratio below the lower limit of normal in participants >40 years, with reference values derived from the Global Lung Function Initiative [20] (for the purpose of the current analyses, 79 participants with a diagnosis and symptoms of both asthma and COPD, were excluded); 6) cardiovascular disease (hypertension, coronary artery disease, heart failure, atrial fibrillation), based on doctor's diagnosis and validated by specific medication use; and 7) fasting venous blood sample for standard blood chemistry (including blood glucose, haemoglobin A1c (HbA1c), cholesterol) and total and differential cell counts using a certified hospital laboratory. The diagnoses of diabetes (blood glucose ≥126 mg·dL−1, HbA1c ≥6.5% and/or medication), metabolic syndrome (central obesity plus at least two of: triglycerides ≥150 mg·dL−1 or specific medication; high-density lipoprotein cholesterol <40 mg·dL−1 in men, <50 mg·dL−1 in women or specific medication; fasting glucose ≥100 mg·dL−1; systolic blood pressure ≥130 mmHg, or diastolic blood pressure ≥85 mmHg, or specific medication) and obesity (BMI >30 kg·m−2) were established following international recommendations [21].
Data analysis
Results are presented as total counts (%), mean±sd, median (IQR) or geometric mean (95% CI), as appropriate. Normality of data was tested via a Kolmogorov–Smirnov test. The Mann–Whitney U-test was used to compare medians, and the Levene's test was used to compare interquartile ranges. We used a forced entry binary multivariable logistic regression model (OR and 95% CI) to investigate associations between “high” blood eosinophil counts (>75th percentile) and potential confounders. The following covariates were included in the model: sex, age group, positive skin prick test, current smoking, former smoking, smoking history ≥20 pack-years (heavy smoking), obesity, metabolic syndrome, cardiovascular disease (hypertension, coronary artery disease, heart failure, atrial fibrillation), diabetes, asthma and COPD. All analyses were performed with SPSS Statistics for Windows, 2016 release (IBM Corp., Armonk, NY, USA).
Results
Characteristics of participants
Of the overall 11 423 participants in LEAD who completed lung function testing and the study questionnaires, 11 042 (96.7%) had blood eosinophil counts measured. Table 1 shows the main demographic characteristics of these 11 042 participants. Males and females were similarly represented; the mean±sd age was 44.9±19.3 years, spanning from 6 to 80 years. Atopy (positive skin prick test) was observed in 37.9% of participants, and 21.7% of individuals were current smokers, often heavy smokers (17.3%). Hypertension, obesity and metabolic syndrome were identified in around 17% of the population studied, whereas COPD was diagnosed in 2.7% and asthma in 4.1% of participants. Cardiovascular diseases and diabetes occurred in 8.3% and 5.5% of individuals.
Population baseline demographics, blood eosinophil counts and comorbidities
Blood eosinophil counts and potential confounders
Eosinophil counts ranged from 0 to 2020 cells·μL−1, and were non-normally distributed (figure 1) with a right skewed shape (skewness 3.395; p<0.0001), so the geometric mean was calculated from log transformed data (128 cells·μL−1; table 1). From these data, the 75th percentile (our definition of “high eosinophil”) provided a cut-point of 210 cells·μL−1 (figure 1).

Frequency distribution of blood eosinophil counts in the entire LEAD cohort. The black line indicates geometric mean (128 cells·μL−1) and the dotted line indicates the 75th percentile (>201 cells·μL−1). For further explanations, see text.
Figure 2 presents the results of the binary multivariable logistic regression model used to identify the factors that were significantly associated with high blood eosinophil counts. We found that male sex (OR 1.36 (95% CI 1.24–1.50)), younger age (≤18 years; 2.41 (2.01–2.89)), positive skin prick test (1.64 (1.50–1.80)), current smoking (1.72 (1.52–1.96)), obesity (1.16 (1.02–1.33)), presence of metabolic syndrome (1.41 (1.22–1.64)) and a diagnosis of asthma (2.05 (1.70–2.51)) or COPD (1.56 (1.20–2.03)) were all significantly associated with high blood eosinophil counts. By contrast, former smoking, hypertension, cardiovascular disease (myocardial infarction, atrial fibrillation, chronic heart failure) and diabetes were not. Of note, although current smoking was significantly associated with high blood eosinophil counts, high cumulative smoking exposure (≥20 pack years) was not (1.11 (0.96–1.27)). In a separate model, we checked for possible interactions between the covariates; there was none. However, atopy (positive skin prick test), current smoking and metabolic syndrome coexisted with increased mean blood eosinophil counts in the total study population (figure 3a). The figure shows that individuals with atopy have higher blood eosinophil counts than those without atopy, as do current smokers compared to former/never smokers, and individuals with metabolic syndrome compared to those without the syndrome, demonstrating independent attributable risks for each single risk factor. In addition, the combination of atopy, current smoking and metabolic syndrome was associated with the highest blood eosinophil counts in these subgroups. After excluding age and sex, of the remaining six significantly associated factors that are potentially modifiable (positive skin prick test, current smoking, obesity, presence of metabolic syndrome, and a diagnosis of asthma or COPD), the presence of an increasing number of concomitant associated factors was associated with higher blood eosinophil counts (figure 3b). Note that each individual could have a maximum of five associated factors, given that those with both asthma and COPD were excluded from these analyses.

Logistic multivariable regression analysis results (OR and 95% CI) for “high blood eosinophil” (>210 cells·µL−1) in the LEAD cohort. Dark symbols indicate significant OR (p<0.05); light symbols denote non-significant associations. For further explanations, see text.
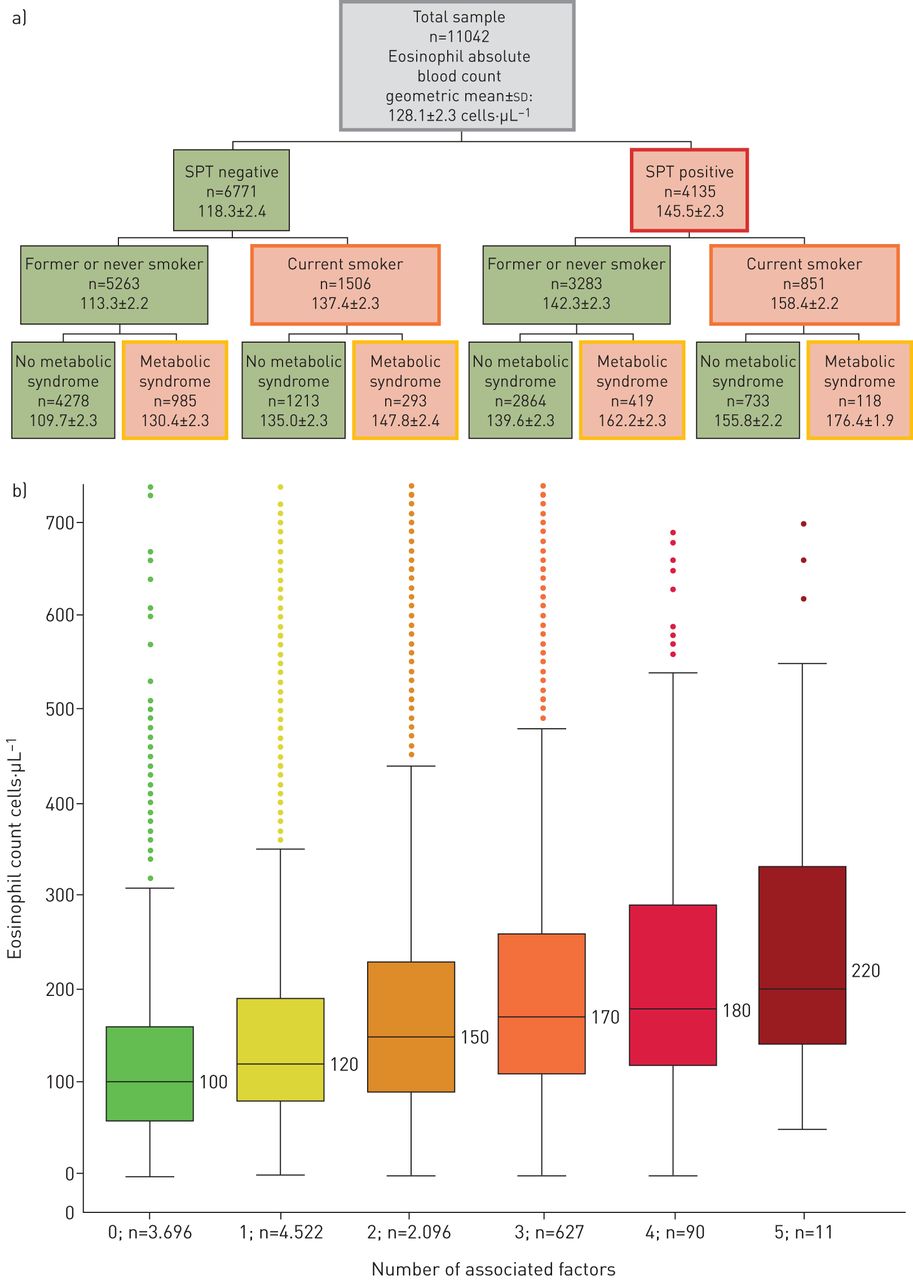
a) Flow chart showing the coexistence of increased mean blood eosinophil counts and clinical characteristics. Sample sizes (n), geometric mean±sd. Green boxes indicate no coexistence; orange boxes indicate coexistence of the characteristic and increased eosinophil counts; coloured frames indicate the characteristic (red: skin prick test+; orange: current smoking; yellow: metabolic syndrome). b) Cumulative effect on blood eosinophil counts of concomitant associated factors in the total population cohort. (n=sample size; boxes represent IQR: 25th percentile–75th percentile; black line=median; Whiskers show min–max values; bullets show extremes). The six factors included were positive skin prick test, current smoking, obesity, presence of metabolic syndrome and a diagnosis of asthma or COPD. Note that this analysis includes a maximum of five factors, since individuals with comorbid asthma and COPD were excluded from the analyses. For further explanations, see text.
Figure 4 shows the age and sex dependency of blood eosinophil counts in the total LEAD cohort (top) and in the “healthy” sub-population (bottom) in which all subjects with any of the factors identified by multivariable logistic regression (figure 2) were excluded; in other words, we excluded individuals with a positive skin prick test, who were current smokers or were obese, or who had metabolic syndrome, COPD or asthma. In both cases blood eosinophil counts were higher: 1) in early life, plateauing after 18 years of age; 2) in males (blue) than females (red); and 3) in the total LEAD cohort (meangeom 128 cells·µL−1) than in the “healthy” sub-population (meangeom 107 cells·µL−1). The range (5%–95%) of eosinophil counts in the “healthy” adult sub-population was 30–330 cells·μL−1 in males and 30–310 cells·μL−1 in females. Table 2 shows the details of the range of blood eosinophil counts per age group and sex (depicted in figure 4) in the total population and the “healthy” sub-population.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Age and sex dependency of blood eosinophil counts in the total LEAD cohort (top) and the “healthy” sub-population (bottom). Lines represent median values and ribbons the range (5th to 95th percentile) for males (blue) and females (red). The “healthy” sub-population excluded individuals with a positive skin prick test, who were current smokers, were obese, had metabolic syndrome, or had been diagnosed with asthma or COPD. For further explanations, see text.
Blood eosinophil counts in the total LEAD cohort and in a “healthy” sub-population by age and sex
Discussion
This cross-sectional study in a large (n=11 042) and well-characterised general population cohort in Austria [16], provides several important and novel observations: 1) blood eosinophil counts are highest in infancy and adolescence, and are independent of age after the age of 18 years, both in males and females; 2) eosinophil counts are higher in males than in females in all age groups; 3) a number of factors besides age and sex, including atopy, smoking, asthma, COPD, obesity and metabolic syndrome, are independently associated with high eosinophil counts, with these factors having an additive effect; 4) when these factors are excluded, circulating eosinophil levels in a healthy population aged 18 years and older is lower than that generally used in the clinic (median (5%–95% CI) of 120 (30–330) cells·µL−1 in males and 100 (30–310) cells·µL−1 in females).
Previous studies
That blood eosinophil counts are higher both in children and atopic subjects was already known [22–26] and, in fact, our results provide further confirmatory evidence. Yet, we describe here other novel factors associated with high eosinophil counts, which likely help to explain the skewed distribution of blood eosinophil counts in the general population. Smoking is associated with exacerbations both in patients with asthma and those with COPD [23, 27–29], but the association with blood eosinophil counts in population cohorts has not been extensively studied. A recent analysis from the Copenhagen population cohort [30] showed an increase in leucocytes but not in eosinophils in current smokers, whereas in a Japanese longitudinal cohort study, current smoking increased levels of white blood cells and eosinophils, with smoking cessation reducing levels to normal [10]. Moreover, an experimental study in young adults that measured blood eosinophils after smoking exposure and exercise showed a significant increase in blood eosinophil counts [31]. We hypothesise that exposure to tobacco smoke could activate different pathways of inflammation, resulting in increased blood eosinophil counts via innate lymphocytes such as in nonallergic asthma, or could result in neutrophilic inflammation associated with symptoms of bronchitis in smokers [29, 30]. As we did not find any association between C-reactive protein level and eosinophils (data not shown), it is unlikely that the increased level of blood eosinophils in our population is driven by common systemic inflammation. Furthermore, the few studies that have examined the relationship between eosinophil counts and obesity or metabolic syndrome have had contradictory results in general population cohorts [13, 32, 33], although one recent study showed that, in metabolic syndrome, blood eosinophil counts were increased in concordance with adipose tissue infiltration by eosinophils [34]. Our data highlight the complexity of the problem, given the associated factors had an independent, additive effect on blood eosinophil counts. To our knowledge this has not previously been demonstrated, and so warrants further attention when multimorbid patients are studied.
When all these factors were excluded in the “healthy” sub-population, we observed that blood eosinophil counts were consistently higher in males than females regardless of age and, importantly, that the median (and associated 95th percentile) eosinophil values in this “healthy” population were lower than those regularly used in clinical practice. All in all, these observations will have to be considered in future studies that investigate the role of eosinophils in health and disease [35, 36].
Implications for asthma and COPD management
Several of this study's observations may have direct implications for asthma management. First, we have to consider the age range of the investigated population, as our study shows that younger individuals have much higher blood eosinophil counts. Second, multimorbidity increases with age, both in patients with asthma and in the total population in our study. We hypothesise that the additive effect of factors associated with high eosinophil counts in our population cohort (metabolic syndrome, current smoking, obesity and atopy) could impact the predictive role of blood eosinophils for treatment efficacy in some subgroups of patients with asthma or COPD.
Our findings may also have implications for COPD management. First, the occurrence of COPD (like asthma) is, in itself, associated with increased blood eosinophil counts. Of note, the eosinophil counts of participants with COPD studied here are consistent with those reported in the Copenhagen general population study (median (IQR): 180 (120–270) cells·µL−1) [27] and in an analysis of the UK Clinical Practice Research Datalink (geometric mean (95% CI): 192.2 (190.2–194.1) cells·μL−1) [37]. Secondly, eosinophil counts were independent of age and higher in males, and COPD is most often diagnosed in males in their 6th or 7th decade of age. Thirdly, a threshold of 300 cells·µL−1 to support the use of ICS in patients with COPD is often questioned because it is believed to be within the “normal” range of blood eosinophil counts [38]. Yet, our results suggest that average values, especially in those over the age of 40 years, are lower than this value, with medians of 100–120 cells·µL−1 in the “healthy” sub-population, with the 95th percentiles of these median values being between 290 and 350 cells·µL−1. In contrast, in patients with severe asthma (all of whom should already be receiving medium- or high-dose ICS) a blood eosinophil threshold of 300 cells·µL−1 is suggested by GINA as suggesting eligibility for an anti-interleukin (IL) 5 or 5R, whereas a blood eosinophil threshold of 150 cells·µL−1 or a fractional exhaled nitric oxide threshold of 25 ppb suggests eligibility for an anti-IL4Rα [1].
Strengths and limitations
The large sample size, age and sex stratification from the general population and careful consideration of potential confounders associated with high eosinophil counts are clear strengths of our study; as is that the recruited population is representative of the general Austrian population (as discussed in a previous manuscript on the objectives and external validity of the cohort [16]). That it was a cross-sectional analysis of an ongoing longitudinal study is a limitation. In particular, the results of the analyses do not provide any information on the use of blood eosinophil counts as a biomarker of, for example, response to therapy, which could be possible from a longitudinal study. Likewise, parasitic infections are well-known causes of high eosinophil levels and they were not specifically investigated (or excluded) from this analysis. However, the prevalence of parasitic infections in Austria is small (only 0.28% of samples in one study using data from 1990 to 2000 having positive results [39], and thus unlikely influence the current results. However, this factor may need to be considered in other regions of the world [24].
Conclusions
The results of this study define typical blood eosinophil counts in “healthy” Austrian subjects and identify a number of factors associated with high eosinophil counts. The results clearly show that age and sex need more attention when defining “normal” values, and that in complex comorbid situations blood eosinophil counts are higher with an increasing number of comorbidities. Overall, this novel information will contribute to better interpretation of blood eosinophil counts, both in general population cohorts and in patients with airway diseases.
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-01874-2019.Shareable
Acknowledgements
Authors thank all participants for their willingness to contribute to medical research, and all field workers for their fantastic day-to-day work.
Footnotes
This article has an editorial commentary: https://doi.org/10.1183/13993003.00473-2020
This study is registered at ClinicalTrials.gov with identifier NCT01727518. Data availability: as this is an ongoing longitudinal cohort study, open access data will not be provided. Methodology and the hypothesis are published in J Epidemiol 2019; 29: 315–324. Study protocol is published at clinical trials.gov (NCT01727518). Data from the database are shared with CADSET (chronic airway disease early stratification): a new ERS clinical research collaboration initiative in collaborative projects and on request for specific research questions after approval of the research consortium of LEAD. Requests can be submitted to office@leadstudy.at
Conflict of interest: S. Hartl has received unrestricted research grants for the Ludwig Boltzmann Institute of COPD and Respiratory Epidemiology and is on advisory boards for GSK, Boehringer Ingelheim, Novartis, Menarini, Chiesi, AstraZeneca, MSD, Roche, Abbvie, Takeda and TEVA for respiratory oncology and COPD.
Conflict of interest: M-K. Breyer reports unrestricted grants for the LEAD study from GlaxoSmithKline, Novartis Pharma, AstraZeneca, Chiesi Pharma, Menarini Pharma, TEVA Ratiopharm, MSD, Air Liquide Health Care, Pfizer Corporation, Boehringer Ingelheim and Mundipharma.
Conflict of interest: O.C. Burghuber reports grants from Boehringer Ingelheim, GSK, AstraZeneca, Menarini, Teva, Pfizer, Chiesi, Federal State Goverment Dept of Health and Novartis, non-financial support from AirLiquid and Municipial Dept of Health in Vienna, during the conduct of the study; personal fees for advisory board work and lectures from Boehringer Ingelheim, AstraZeneca, Chiesi, MSD, Menarini and Roche, personal fees for advisory board work from GSK, outside the submitted work.
Conflict of interest: A. Ofenheimer has nothing to disclose.
Conflict of interest: A. Schrott has nothing to disclose.
Conflict of interest: M.H. Urban reports grants from Nycomed Pharma, during the conduct of the study; personal fees for lectures and advisory board work from AstraZeneca and Boehringer Ingelheim, outside the submitted work.
Conflict of interest: A. Agusti reports personal fees from AstraZeneca, Chiesi and Nuvaira, grants and personal fees from Menarini and GSK, outside the submitted work.
Conflict of interest: M. Studnicka reports personal fees for consultancy from Chiesi, AstraZeneca, Novartis, Boehringer and Almirall, and personal fees for lectures from GSK, AstraZeneca, Almirall, Novartis and Boehringer, outside the submitted work.
Conflict of interest: E.F.M. Wouters reports personal fees for advisory board work from Nycomed and Boehringer, grants from AstraZeneca and GSK, personal fees for lectures from AstraZeneca, Novartis, GSK and Chiesi, outside the submitted work.
Conflict of interest: R. Breyer-Kohansal reports personal fees for presentations and/or participations for AstraZeneca, Boehringer Ingelheim, Chiesi and Novartis outside the submitted work.
Support statement: This work was supported by The Municipal Department of Health and Environment of Vienna, the Federal State Governmental Department of Health of Lower Austria, the Ludwig Boltzmann Society, unrestricted scientific grants from GlaxoSmithKline, Novartis Pharma, AstraZeneca, Chiesi Farmaceutici SpA, Menarini Pharma, Teva, MSD, Air Liquide Health Care, Pfizer and Boehringer Ingelheim. None of the supporting parties has any participation in the data, nor have they contributed to the design or the content of the manuscript.
- Received September 20, 2019.
- Accepted January 28, 2020.
- Copyright ©ERS 2020