



Donor surfactant protein A2 polymorphism and lung transplant survival
- Frank D'Ovidio1⇑,
- Joanna Floros2,
- Beatrice Aramini1,
- David Lederer1,
- Susan L. DiAngelo2,
- Selim Arcasoy1,
- Joshua R. Sonett1,
- Hillary Robbins1,
- Lory Shah1,
- Joseph Costa1 and
- Andreacarola Urso1
- 1Division of Thoracic Surgery, Lung Transplant Program, Columbia University Medical Center, New York, NY, USA
- 2Center for Host Defense, Inflammation, and Lung Disease (CHILD) Research Department of Pediatrics, The Pennsylvania State University College of Medicine, Hershey, PA, USA
- Frank D'Ovidio, Surgical Director Lung Transplant Program, New York-Presbyterian Hospital, 161 Fort Washington Ave, New York, NY 10032, USA. E-mail: fd2133{at}cumc.columbia.edu
Abstract
Purpose Gene polymorphisms of surfactant proteins, key players in lung innate immunity, have been associated with various lung diseases. The aim of this study was to investigate the potential association between variations within the surfactant protein (SP)-A gene of the donor lung allograft and recipient post-transplant outcome.
Methods Lung-transplant patients (n=192) were prospectively followed-up with pulmonary function tests, bronchoscopies with bronchoalveolar lavage and biopsies. Donor lungs were assayed for SP-A1 (6An) and SP-A2 (1An) gene polymorphism using the pyrosequencing method. Unadjusted and adjusted stratified Cox survival models are reported.
Results SP-A1 and SP-A2 genotype frequency and lung transplant recipient and donor characteristics as well as cause of death are noted. Recipients were grouped per donor SP-A2 variants. Individuals that received lungs from donors with the SP-A2 1A0 (n=102) versus 1A1 variant (n=68) or SP-A2 genotype 1A01A0 (n=54) versus 1A0A1 (n=38) had greater survival at 1 year (log-rank p<0.025). No significant association was noted for SP-A1 variants. Stratified adjusted survival models for 1-year survival and diagnosis showed a reduced survival for 1A1 variant and the 1A01A1 genotype. Furthermore, when survival was conditional on 1-year survival no significance was observed, indicating that the survival difference was due to the first year's outcome associated with the 1A1 variant.
Conclusion Donor lung SP-A gene polymorphisms are associated with post-transplant clinical outcome. Lungs from donors with the SP-A2 variant 1A1 had a reduced survival at 1 year. The observed donor genetic differences, via innate immunity relate to the post-transplant clinical outcome.
Abstract
Donor genetic polymorphisms of the lung-specific innate defence systems determine post-lung transplant recipient outcome http://bit.ly/2QNpX7Q
Introduction
Lung transplantation is a widely accepted therapeutic option for end-stage lung disease. Yet, clinical outcome is challenged by primary graft failure, responsible for the majority of the early mortality, and by chronic allograft dysfunction and chronic rejection accounting for >30% of deaths after the third post-operative year. Lung transplantation suffers recipient and graft survival, significantly lower than for liver, kidney and heart transplantation. The lung's ongoing exposure to the environment is probably the determining factor, with a significant role attributed to the performance of its defence mechanisms.
Pulmonary surfactant and the surfactant-related proteins are primary components of the organ's specific innate immunity. As such, they serve as one of the first host defence mechanisms mounted by the lung against the various insults. In addition to lowering the alveolar surface tension, surfactant phospholipids serve as part of the physical mucosal barrier [1, 2]. Similarly, surfactant associated proteins A, B, C and D play different specific roles with respect to surface tension lowering function, phospholipid homeostasis and innate and adaptive immunity [3–8]. The hydrophilic surfactant proteins (SP)-A and SP-D play essential roles in innate host defence, interacting between the innate and the adaptive immune systems [3–8].
SP-A biological activity seems to be genetically determined and its polymorphisms have been associated with several lung disease: respiratory distress syndrome, idiopathic pulmonary fibrosis and emphysema [9, 10]. The two sftpa1 and sftpa2 genes, encoding the proteins SP-A1 and SP-A2, respectively, have been identified with several polymorphisms within the coding regions, SP-A1 (6A, 6A2–20) and SP-A2 (1A, 1A0–13) [11, 12]. In particular, SP-A2 is the predominant and very polymorphic SP-A protein present in the adult human airways [13].
We showed a differential SP-A protein expression in the peri-lung transplant phase according to the SP-A2 variants and further showed a significant pharmacogenetic relationship with of the SP-A2 methylprednisolone treatment [14, 15].
These observations allowed us to formulate the main hypothesis for this project which focuses on pulmonary SP-A2 polymorphisms determining lung allograft survival.
Methods
The study was approved by the institutional review board of the Columbia University Medical Center (New York, NY, USA). Informed consent in adherence to the principles set forth in the Helsinki Declaration was obtained from each patient for the collection of blood samples from the donor of the lung allograft prior to implantation. We performed a retrospective analysis of prospectively banked samples. All samples were prospectively collected specifically to test the hypothesis of gene and protein expression associations with post-lung transplant outcomes. This study included 192 patients consecutively transplanted. Post-lung transplantation patients underwent pulmonary function testing in the lung transplant clinic weekly for the first 3 months. Beyond 3 months, patients were seen monthly for the first year and on alternating months for the second year. Follow-up frequency was extended to every 3 months beyond the second year after surgery.
Recipient data were prospectively collected with regards to the development of chronic lung allograft dysfunction (CLAD) as determined by the permanent drop of the forced expiratory volume in 1 s (FEV1) by >20% from their post-transplant baseline and survival. CLAD development was monitored using routine pulmonary function tests. The interval of time from transplant to development of CLAD and survival after transplant was monitored.
Donor and recipient clinical information
Donor data were collected with regard to age, smoking history, sex, last oxygen tension/inspiratory oxygen fraction ratio prior to procurement and duration of cold ischaemic preservation.
All donors received 2 g methylprednisolone. Recipient data were collected with regard to the development of primary graft dysfunction in the first three post-transplant days; development of CLAD was determined by the permanent drop of the FEV1 by >20% from their post-transplant baseline and survival. The time from transplant to development of CLAD and death was monitored.
Biological samples from lung allograft
Blood samples from the donor of the lung allograft were collected at the time of lung procurement. Blood samples were stored at −80°C for subsequent analysis. All samples were batched and assayed at once. Total DNA was extracted from blood with a DNA extraction kit (Qiagen, Germantown, MD, USA), according to the manufacturer's instructions. The quality of the DNA was assessed prior to assaying. Donor demographics and clinical data were collected by organ procurement organisation personnel and recorded in the donor medical record.
Lung allograft SP-A gene variants
The SP-A1 and SP-A2 gene polymorphisms were assessed in a blinded fashion for donor and recipient characteristics and for clinical outcomes. The SP-A1 and SP-A2 single nucleotide polymorphism (SNPs) assessment was performed using a pyrosequencing protocol. The PCR-based restriction fragment length polymorphism genotype method for SP-A provided the basis for the pyrosequencing protocol, which is a primer-based DNA sequencing method. Pyrograms are scored by pattern-recognition software that compares the predicted SNP pattern (histogram) to the observed pattern (pyrogram) (Pyrosequencing AB, Uppsala, Sweden). Scoring of SP-A1 (6A, 6A2–20) and SP-A2 (1A, 1A0–13) gene variants was performed, as described previously [16, 17].
Statistical analysis
We analysed categorical data using Chi-squared and Fisher's exact tests. We constructed stratified Cox proportional hazards models to examine associations between genotype and time to events of interest (CLAD and survival) with strata for recipient disease and with adjustment for a priori purposely selected recipient variables known to affect outcome after lung transplantation (i.e. precision variables). For time-to-death analyses, we censored follow-up time at the end of the study. For the CLAD analyses, we censored follow-up time at death and at end of study. Variants were assumed to have additive effects. There were no missing covariate data.
Differences were considered significant when the p-value was <0.05. Continuous variables are expressed as medians and 25–75th percentile range. Statistical analysis was performed using SAS 9.2 software (SAS Institute, Cary, NC, USA).
Results
Donor and recipient information
Table 1 shows the donor lung SP-A1 and the SP-A2 variant frequencies seen in our cohort of lung transplant recipients. Supplementary table S1 shows the SPA1 and SPA2 genotype combinations. The overall characteristics of the 192 lung transplant recipients and of the donors are shown in table 2.
Surfactant protein (SP)-A1 and SP-A2 variant and genotype frequency
Lung transplant recipient and donor characteristics
The overall median follow-up time was 1290 (823–1843) days. To date, 60 out of 192 patients have died, four within 30 days of the lung transplant and 56 with a median survival of 719 (274–1269) days. The 132 patients currently alive have a median follow-up of 1595 (1091–2054) days. CLAD was diagnosed in 88 patients, 38 of whom have died, with median survival of 902 (575–1422) days and 50 of whom are currently alive with a median follow-up of 1841 (1450–2296) days. Patients alive and free of CLAD are 81 with a median follow-up of 1303 (1006–1823) days. Table 2 shows the overall recipient and donor characteristics of the study cohort.
Grouping of lung transplant recipients: SP-A2 variant and genotype associations
Lung transplant recipients were grouped according to the two most frequent donor SP-A1 (6A2 and 6A3) and SP-A2 variants (1A0 and 1A1). No association with clinical outcomes was noted for the SP-A1 variants. Figure 1 shows the non-adjusted survival curves for patients grouped according to the SP-A2 variants as well as the curves conditional to 1-year survival. No association was noted for freedom from CLAD. The characteristics of the patients grouped according to the SP-A2 SNP variants for 1A0 and 1A1 shown in table 3 include recipient age, sex, end-stage pulmonary disease, type of transplant, cytomegalovirus (CMV) mismatch and sex mismatch. With regard to the distribution of recipient diagnoses, some differences were noted; in particular, cystic fibrosis (24% for variant 1A0 versus 17% for variant 1A1) and chronic obstructive pulmonary disease (COPD) (25% for variant 1A0 versus 34% for variant 1A1), whereas interstitial lung disease and “other” were approximately half and half of each variant (table 3).
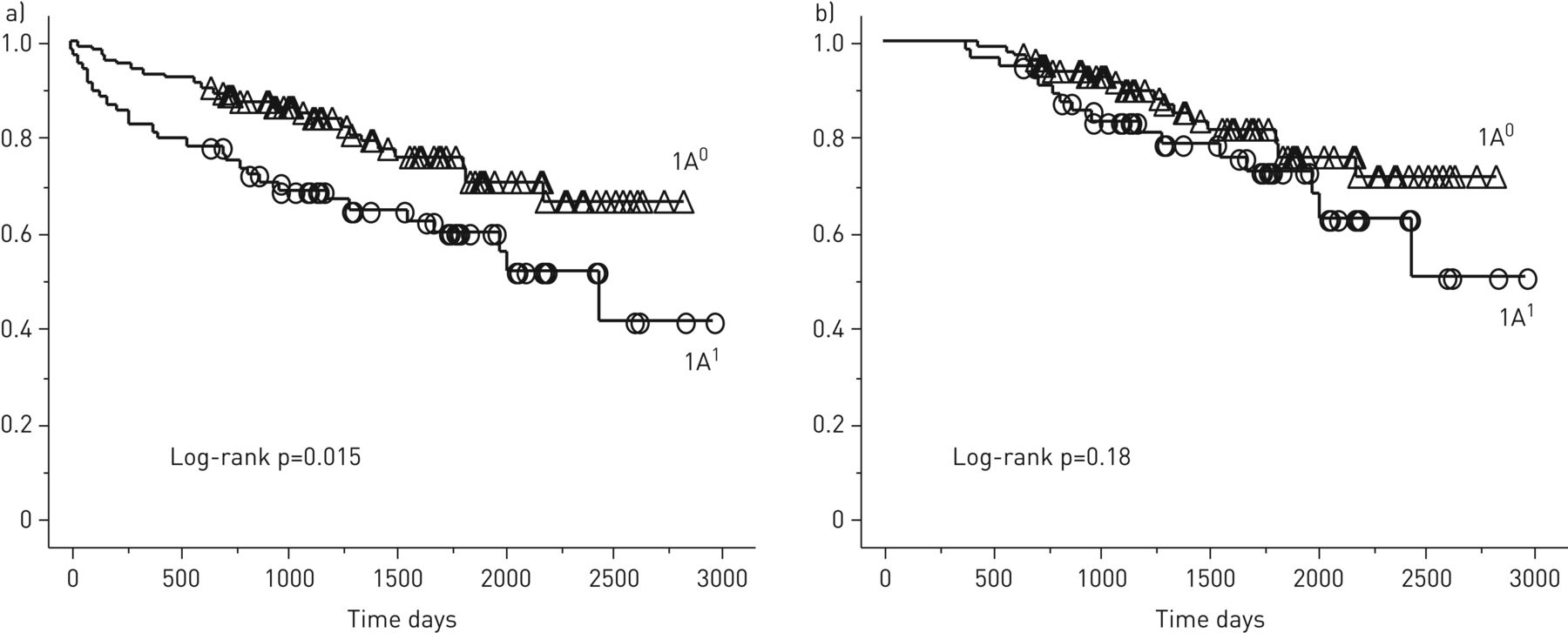
Non-adjusted lung transplant patient actual survival curves of recipients grouped according to the lung allograft donor surfactant protein (SP)-A2 polymorphic variants 1A0 and 1A1. A significantly greater survival during the first year post-lung transplantation was noted for recipients of donor lungs with SP-A2 variant 1A1. Mantel–Cox log-rank test showed p=0.015 for the overall survival analysis, although no significant difference for survival in patients that were alive at 1 year after lung transplantation. a) Survival; b) conditional 1-year survival.
Donor and recipient characteristics according to the donor surfactant protein (SP)-A2 variants
Figure 2 shows the non-adjusted survival curves for patients grouped according to the SP-A2 genotypes 1A01A0 and 1A01A1 as well as the curves conditional to 1-year survival. The characteristics of the patient grouped according to the SP-A2 genotypes for 1A01A0 and 1A01A1 shown in table 4 include recipient age, sex, end-stage pulmonary disease, type of transplant, CMV mismatch and sex mismatch. With regard to the distribution of the recipient diagnoses, some differences were noted: cystic fibrosis 28% for genotype 1A01A0 versus 18% for variant 1A01A1; COPD 24% for genotype 1A01A0 versus 37% for 1A01A1; and for interstitial lung disease and “other” about half and a half with each genotype (table 4).

{kind=link}
{kind=link}
Non-adjusted lung transplant patient actual survival curves for recipients grouped according to the lung allograft donor surfactant protein (SP)-A2 polymorphic genotypes 1A01A0 and 1A01A1. A significant greater survival during the first year post-lung transplantation was noted for recipients of donor lungs with SP-A2 genotype 1A01A0. The Mantel–Cox log-rank test showed (p=0.016) for the overall survival, although no significant difference in patients that were alive at 1 year after lung transplantation. a) Survival; b) conditional 1-year survival.
Donor and recipient characteristics according to the donor surfactant protein (SP)-A2 genotypes
1-year survival
Table 5 shows the 1-year survival models stratified for recipient diagnosis, with adjustment for donor polymorphic variation in 1A1, recipient age, sex, procedure type, CMV status and sex mismatch. The data showed a significant effect in recipients with regards to the presence of donor variant 1A1 (p=0.02), age (p=0.04) and bilateral lung transplant (p=0.04) on the 1-year survival. In addition, table 5 shows the 1-year survival models for the SP-A2 genotypes stratified for recipient diagnosis, with adjustment for donor polymorphic variation in 1A1, recipient age, sex, procedure type, CMV status and sex mismatch. The SP-A2 1A0A1 genotype was associated with a significant overall reduction in survival (p=0.02) in the first year. Table 6 shows the cause of death within the first year, according to the donor 1A1 and 1A0 variants as well as according to the donor SP-A2 genotypes 1A01A0 and 1A01A1.
Adjusted survival models for 1-year survival stratified per recipient diagnosis
Cause of death within first year
Discussion
The role of the genetic background of the donor lung has not been sufficiently explored in relation to lung transplant recipient outcomes. This study reports novel findings with regards to the role played by SP-A gene polymorphisms in clinical outcomes post-lung transplantation. Donor lung SP-A polymorphic variants may serve as predictors of post-transplant recipient survival. The SP-A1 and SP-A2 gene polymorphisms were investigated, uncovering a significant association between the donor lung SP-A2 variants and post-lung transplant recipient survival.
We have previously reported that donor lung SP-D polymorphisms predict chronic lung allograft dysfunction, although no association to survival was reported for any of those variants [18]. Hence, the two hydrophilic surfactant proteins SP-D and SP-A may have a distinct impact on the overall innate and adaptive response to pathogens.
The human SP-A locus consists of two functional genes, sftpa1 and sftpa2, encoding SP-A1 and SP-A2, respectively. Each gene has been identified with several polymorphisms within the coding region, which may or may not be subject to amino acid substitutions, SP-A1 (6A, 6A2–20), and SP-A2 (1A, 1A0–13) [12, 16]. Associations of SP-A1 and SP-A2 variants have been shown for several pulmonary diseases [9, 10] and mutations in these genes are found in patients with interstitial lung disease and lung cancer. Despite such frequency, their pathologic mechanism is poorly understood. Gene polymorphisms of SP-A1 and SP-A2 may be responsible for both quantitative and qualitative differences in levels of protein synthesis, variations in protein functionality, or an altered ratio between the two proteins SP-A1 and SP-A2 [19–23]. Hence, within the context of organ specific innate immunity, a compromised surfactant proteomic composition may largely contribute to a deficiency in first-line responses to various insults.
Recent animal studies have shown that not only do SP-A1 and SP-A2 variants distinctively affect the alveolar macrophage miRNome [24], but, most relevantly, they differentially affect lung function and survival after infection [25, 26]. It is therefore conceivable that SP-A gene variants may contribute to the complex aetiologic pathogenesis of lung allograft dysfunction. This retrospective study, despite having a potential bias from uneven distribution of patient characteristics, which was taken in account in the adjusted statistical analysis, documents this association for the first time showing a significantly greater risk of death within the first year post-lung transplant for recipients of donor lungs with SP-A2 variant 1A1 and genotype 1A01A1 compared to others (figure 1 and table 5). This appears to be due to a greater incidence of death from infection (table 6). Interestingly, Dominic et al. [27] demonstrated that homozygosity of the SP-A2 variant, 1A1, was associated with an increased risk of meningococcal disease, suggesting a recessive effect of this variant. The carriage of another SP-A2 variant, 1A5, was significantly associated with a reduced risk of infection, suggesting a dominant effect of this variant. Variants 1A1 and 1A5 are identical at the codons that encode amino acids 9 and 140, but they differ at amino acids 91 and 223 [27]. The change in amino acid 223 between these two variants is significant. Variants 1A5 and 1A0 that were associated with reduced infection risk (1A5) [27] and better survival (1A0) in the present study and in a recent mouse study [26] have the same amino acid, namely a glutamine. This charged amino acid may contribute to a better outcome.
Low levels of SP-A mRNA measured in the lung allograft just prior to implantation appeared to be a negative predictor with respect to post-transplant survival [14]. An association between donor lung SP-A mRNA expression levels and SP-A2 genotype has been previously observed [14]. In particular, the SP-A2 genotype 1A0A0 had greater levels of SP-A mRNA expression in the allograft prior to implantation [14]. Lung donors are treated with very high levels of steroids prior to organ procurement. We recently reported a significant pharmacogenetic relationship between SP-A2 variants and methylprednisolone. Precision cut lung slices from organs with SP-A2 variant 1A0 and genotype 1A01A0 showed a significantly greater protein expression when treated with methylprednisolone [15]. These observations are consistent with the present results, where recipients from donors with 1A0 variant and 1A01A0 genotype exhibited greater survival, indicating that the total SP-A levels determined by donor lung genotype may play a role in post-transplant recipient survival. Interestingly, the survival advantage identified in this study was observed within the first year, during which recipient immunosuppressive regimes include the greatest levels of steroids.
The lungs, like the intestines, suffer the disadvantage of a continuous exposure to the environment compared to other solid organs, thus they rely on a more active organ-specific innate immunity for first-line protection against ongoing external pathogens [28–31]. Interactions between innate and adaptive immune responses in these organs in the setting of transplantation are probably a major contributor to the increased graft dysfunction that is seen. It is conceivable that the capability of the lung allograft to withstand the various transplant related insults is driven by its genetic background, and especially that of donor innate immunity. The innate immune molecules, SP-A1 and SP-A2, are subject to differential and complex regulation as shown in vitro and in fetal lung explants [32–35].
In conclusion, donor lung SP-A2 gene polymorphisms are associated with post-transplant recipient survival. Further studies are needed to explore the different roles of SP-D and SP-A polymorphisms within the innate and adaptive immune response post-lung transplantation. This study was not designed for a detailed assessment of confounding factors or interaction effects, nevertheless the interesting findings reported significantly add weight to further hypothesis generation regarding the potential impact of genetic polymorphisms for key proteins in the donor lung influencing post-lung transplant outcome(s). In fact our findings suggest a constitutive role of the donor innate immunity towards lung transplant recipient outcome.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Table S1. SP-A1 and SP-A2 genotype combinations. ERJ-00618-2019.SUPPLEMENT
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-00618-2019.Shareable
Footnotes
This article has supplementary material available from erj.ersjournals.com
Conflict of interest: F. D'Ovidio reports grants from NIH-NHLBI, during the conduct of the study.
Conflict of interest: J. Floros has nothing to disclose.
Conflict of interest: B. Aramini has nothing to disclose.
Conflict of interest: D. Lederer has nothing to disclose.
Conflict of interest: S.L. DiAngelo has nothing to disclose.
Conflict of interest: S. Arcasoy has nothing to disclose.
Conflict of interest: J.R. Sonett has nothing to disclose.
Conflict of interest: H. Robbins has nothing to disclose.
Conflict of interest: L. Shah has nothing to disclose.
Conflict of interest: J. Costa has nothing to disclose.
Conflict of interest: A. Urso has nothing to disclose.
Support statement: This work was supported by the National Institutes of Health, NHLBI, R21HL092478-01A2; HL34788. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received March 28, 2019.
- Accepted November 21, 2019.
- Copyright ©ERS 2020