



Video-assisted thoracic lobectomy versus stereotactic body radiotherapy for stage I nonsmall cell lung cancer in elderly patients: a propensity matched comparative analysis
- Deniece D.E.M.A. Detillon1,2⇑,
- Mieke J. Aarts3,
- Katrien De Jaeger4,
- Casper H.J. Van Eijck2 and
- Eelco J. Veen1
- 1Dept of Surgery, Amphia Hospital, Breda, The Netherlands
- 2Dept of Surgery, Erasmus Medical Center, Rotterdam, The Netherlands
- 3Netherlands Cancer Registry, Netherlands Comprehensive Cancer Organization, Utrecht, The Netherlands
- 4Dept of Radiotherapy, Catharina Hospital, Eindhoven, The Netherlands
- Deniece D.E.M.A. Detillon, Dept of Surgery, Amphia Hospital, Molengracht 21, Breda, 4818 CK, The Netherlands. E-mail: DDetillon{at}amphia.nl
Abstract
Comparative studies of the overall survival (OS) in elderly patients with nonsmall cell lung cancer (NSCLC) after surgery or stereotactic body radiotherapy (SBRT) have been limited by mixed extents of resection and different surgical approaches.
792 patients aged ≥65 years with clinical stage I NSCLC underwent video-assisted thoracic surgery (VATS) lobectomy or SBRT between 2010 and 2015. The propensity score-matched primary analysis included data from the full cohort; the secondary analysis included data from a subgroup of patients with data on pulmonary function.
Median OS for unmatched patients was 77 months for patients undergoing VATS lobectomy and 38 months for SBRT. The 1-, 3- and 5-year OS rates after VATS lobectomy were 92%, 76% and 65%, and after SBRT were 90%, 52% and 29% (p<0.001). Median OS for matched patients in the primary analysis was 77 months for patients undergoing VATS lobectomy and 33 months for SBRT. The 1-, 3- and 5-year OS rates after VATS lobectomy were 91%, 68% and 58%, and after SBRT were 87%, 46% and 29% (p<0.001). The survival advantage with VATS lobectomy persisted in the secondary analysis after adjusting for non-matched variables (p=0.034).
We suggest that elderly patients with stage I NSCLC undergoing VATS lobectomy have a better rate of OS than patients undergoing SBRT, irrespective of matching. This could be clinically important in decision-making for elderly patients who can tolerate surgery.
Abstract
This matched analysis compared VATS lobectomy with SBRT in patients aged ≥65 years with clinical stage I NSCLC. VATS lobectomy resulted in better overall survival, which is important in decision-making for elderly patients who can tolerate surgery. http://ow.ly/LkWz30o8pXv
Introduction
Lung cancer is the leading cause of cancer death worldwide and in the Netherlands [1]. The highest incidence rates are found among men and women aged 70–79 years [1]. On the basis of demographic developments, the absolute number of new cases of lung cancer in the Netherlands is expected to increase by 37% between 2015 and 2040 [2].
Surgery offers the best potential cure for early-stage nonsmall cell lung cancer (NSCLC). It is not always offered, however, to elderly patients in view of their advanced age and comorbidities. In our previous study, only 52% of 2168 patients aged ≥65 years with stage I NSCLC were treated surgically and 15% did not receive any cancer-directed therapy [3]. Video-assisted thoracic surgery (VATS) is a minimally invasive surgical approach that was introduced in the Netherlands in 2006 and has been found superior to thoracotomy in terms of post-operative morbidity [4–6].
For patients with inoperable disease, radiotherapy is an alternative treatment with curative intent [6, 7]. Stereotactic body radiotherapy (SBRT) became available in the Netherlands in 2003 and became widespread after 2007 [6]. SBRT consists of the delivery of high doses of radiation in a limited number of fractions. SBRT is superior to conventionally fractionated radiotherapy in terms of local control and overall survival (OS) [8].
Studies comparing surgery with SBRT have produced conflicting OS results. Most of these studies have been limited by different surgical approaches (thoracotomy and VATS) [9–17] and mixed extents of resection (sublobar, lobectomy, bilobectomy, pneumonectomy) [10, 13, 16–18]. Therefore, we performed a study comparing OS between VATS lobectomy and SBRT for patients aged ≥65 years with clinical stage I NSCLC, taking into account differences in patient and tumour characteristics by using propensity score matching.
Materials and methods
Population-based data from the southern region of the Netherlands Cancer Registry (NCR) were used, because information on comorbidities is routinely collected only in this region. This region encompasses 2.4 million inhabitants (15% of the Dutch population). The NCR records data from all patients diagnosed with cancer and receives notifications of all newly diagnosed malignancies from the nationwide network and registry of histopathology and cytopathology in the Netherlands. Additional sources of data are radiotherapy institutes and the Dutch national registry of hospital discharge. These data are supplemented with data from medical records. Cause of death was not available. Follow-up data were complete until February 2018.
We retrieved data for all patients aged ≥65 years diagnosed between 2010 and 2015 with clinical stage I NSCLC, according to the International Union Against Cancer Tumour Node Metastasis (TNM) edition 7 [19], whose primary treatment was VATS lobectomy or SBRT. The VATS procedure involved a multiportal approach without rib spreading. SBRT schedules varied between three to eight fractions delivered two to three times per week in case of multiple fractions. The NCR records the primary treatment given; it was not always clear if this was the same treatment as the intended treatment for surgical patients. The NCR does record VATS conversions, which resulted in some patients having a different extent of resection than lobectomy. An intention-to-treat analysis was performed, i.e. when a conversion was recorded with a resection other than lobectomy, the patient was analysed as having undergone VATS lobectomy (from now on referred to as intended VATS lobectomy). Demographic variables retrieved were age and sex. A slightly adapted version of the Charlson Comorbidity Index (CCI) was used (table 1). Comorbidities were analysed as number (0, 1, 2, 3, ≥4) and adapted CCI score (0, 1, 2, 3, ≥4). Tumour characteristics included clinical tumour stage, tumour location, histology and the presence or absence of pathological confirmation. Dutch national radiotherapy guidelines indicate that patients without pathological confirmation are eligible for radiotherapy in case of 1) a new or growing lesion on computed tomography (CT) scans with characteristics of malignancy, 2) a high risk for developing lung cancer based on age and smoking history and 3) a fluorodeoxyglucose positron emission tomography (FDG-PET) positive lesion [20]. According to the Dutch practice guidelines, all patients with NSCLC who are eligible for curative treatment should undergo PET-CT [7]. The NCR recorded whether a PET-CT was performed, which turned out to be the case in 75–90% of patients. Criteria to perform lung surgery were in accordance with the Dutch practice guidelines for the treatment of NSCLC [7]. Pulmonary function is not recorded in the database. Because we wished to include pulmonary function data as well, we identified patients diagnosed in one specific hospital (Amphia Hospital, Breda, the Netherlands), reviewed their charts manually and retrieved results on percentage predicted forced expiratory volume in 1 s (FEV1 % pred) and percentage predicted diffusing capacity of lung for carbon monoxide (DLCO % pred).
Adapted version of Charlson Comorbidity Index
Statistical analysis
Two analyses were performed using propensity score matching: the primary analysis included data from the full cohort and the secondary analysis included data from the subgroup of patients with data on pulmonary function. Propensity score matching reduces treatment selection bias when estimating causal treatment effects using observational data [21]. Patients were matched separately for the primary and secondary analysis using logistic regression, with the dependent variable being intended VATS lobectomy versus SBRT. Independent variables were selected on the basis of previous studies. Those included in the primary analysis were age, sex, all individual comorbidities from the adapted CCI, CCI score, number of comorbidities, clinical tumour T stage, tumour location, tumour histology and pathological confirmation [9, 10, 12, 13, 15, 18, 22–25]. In the secondary analysis, we included FEV1 % pred [9, 13, 23–25] and DLCO % pred [13] as independent variables, as well as all variables from the primary analysis except all individual comorbidities in the adapted CCI, tumour histology and pathological confirmation. These latter variables were excluded because they resulted in just a few matches. In the secondary analysis we made a distinction between the analysis with and without adjustment for an unbalanced matched variable and the unbalanced non-matched variables. In both analyses, patients were matched using one-to-one nearest neighbour matching without replacement. Calipers of a width equal to 0.2sd of the logit of the propensity score were used. This width results in optimal estimation of risk differences [21]. Balance was assessed with standardised differences because these are not influenced by sample size [26]. Standardised differences for almost all covariates were <0.1, indicating adequate balance [27]. The standardised differences for the remaining few covariates were >0.1 but <0.2, denoting only a small effect on balance [28].
In the full cohort, variables were compared using the Chi-squared test and t-test. In the matched cohorts, variables were compared using the McNemar test and the Wilcoxon signed rank test. Kaplan–Meier survival curves were constructed and p-values were calculated using the logrank test in the full cohort and Cox proportional hazard models stratified by matched pairs in the matched cohorts [29]. Hazard ratios (HR) and 95% confidence intervals were calculated for the first 15 months of follow-up and after 15 months of follow-up because the Kaplan–Meier curves were quite similar in the first 15 months. All statistical tests were two-sided, and p≤0.05 was considered to indicate statistical significance. Statistical analyses were performed using SPSS statistical software (SPSS version 22; Chicago, IL, USA).
Results
Between 2010 and 2015, 625 patients aged ≥65 years underwent lobectomy for stage I NSCLC: 211 (33.8%) by thoracotomy and 414 (66.2%) were scheduled for VATS. 490 patients were treated with radiotherapy: 112 (22.9%) with conventional radiotherapy and 378 (77.1%) with SBRT. In the present study we focused on 792 patients who underwent intended VATS lobectomy or SBRT. The mean±sd age of the studied group was 73.5±5.5 years and 62% were male. Pulmonary comorbidities were documented in 351 patients (44%), cardiac comorbidities in 291 patients (37%) and 232 patients (29%) had a history of a previous malignancy. Patients undergoing intended VATS lobectomy were younger (p<0.001), had better pulmonary function (p<0.001) and tended to have lower CCI scores (p<0.001) than patients undergoing SBRT (table 2). Tumour location was similar between groups. The presence of a T2a tumour significantly differed between groups: 35% of patients undergoing intended VATS lobectomy versus 24% of patients undergoing SBRT (p=0.003). VATS conversions were recorded in 68 patients (16%). Four patients had a different extent of resection than lobectomy only (one lobectomy and wedge resection, one lobectomy and segmentectomy, one wedge resection, and one lobectomy and rib resection). When table 2 was reconstructed with the exclusion of the 68 patients in whom a conversion was recorded, differences between patients undergoing VATS lobectomy and SBRT remained the same.
Characteristics of unmatched patients aged ≥65 years undergoing intended VATS lobectomy or SBRT for clinical stage I nonsmall cell lung cancer
Pathological confirmation of malignancy was not obtained in 48% of patients undergoing SBRT. Pathological upstaging was documented for 92 patients (22%) after surgery; cT1-2a became pT2b-4 in 48 patients (12%), and cN0 became pN1 in 36 patients (9%) and pN2 in 20 patients (5%). 12 patients (3%) were upstaged to pT2b-4 and pN1-2. Adjuvant treatment was administered to 48 upstaged patients (52%): 40 patients received chemotherapy, six radiotherapy and two chemoradiotherapy.
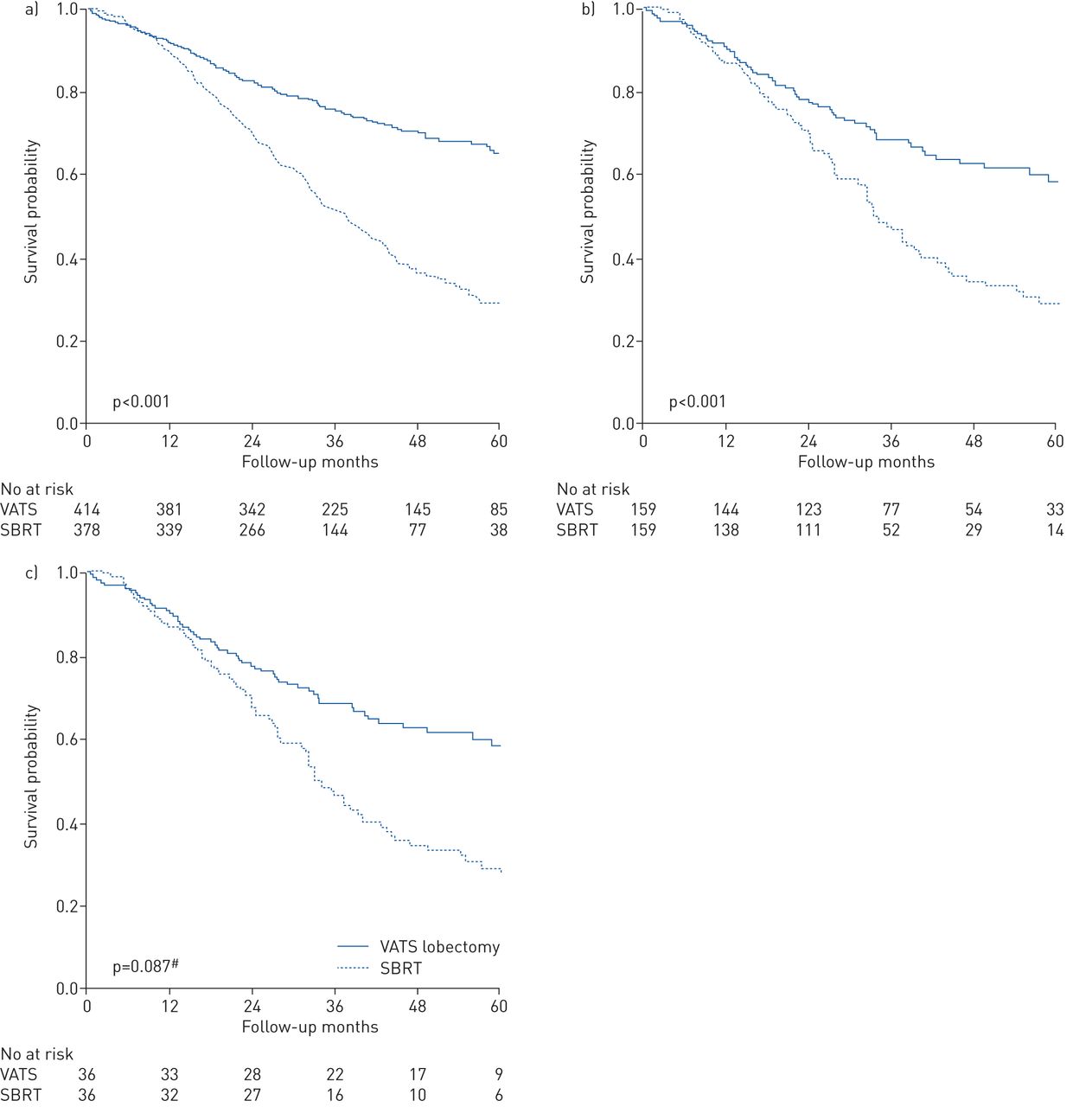
The median follow-up for all patients was 34 months; for patients undergoing intended VATS lobectomy it was 38 months, and for those undergoing SBRT it was 32 months. The estimated median OS time for all patients was 56 months (95% CI 49–62 months); for patients undergoing intended VATS lobectomy it was 77 months (95% CI 72 months–not available (NA), the upper limit of the 95% confidence band around the survival curve did not drop below 0.50), and for patients undergoing SBRT it was 38 months (95% CI 34–42 months, p<0.001). The 1-, 3- and 5-year OS rates for patients undergoing intended VATS lobectomy were 92%, 76% and 65%, and for patients undergoing SBRT were 90%, 52% and 29% (logrank p<0.001, figure 1a). Patients undergoing intended VATS lobectomy had an OS advantage in both the first 15 months (HR 0.66, 95% CI 0.44–0.99) and after 15 months (HR 0.33, 95% CI 0.26–0.43, table 3) of follow-up. For patients undergoing intended VATS lobectomy, age was the only clinical characteristic associated with OS after 15 months of follow-up (HR 1.07, 95% CI 1.02–1.12, p=0.004). The 5-year OS rate was 52% for upstaged patients receiving adjuvant treatment and 39% for those not receiving adjuvant treatment. Patients who were not upstaged had a 5-year OS rate of 70%.

{kind=link}
Kaplan–Meier curves for patients aged ≥65 years undergoing video-assisted thoracic surgery (VATS) lobectomy and stereotactic body radiotherapy (SBRT) for clinical stage I nonsmall cell lung cancer in the full cohort (a), primary analysis (b) and secondary analysis (c). #: p=0.034 when adjusted for cT1a, histology and pathological confirmation.
Overall survival of patients aged ≥65 years after intended VATS lobectomy and SBRT for clinical stage I nonsmall cell lung cancer for the first 15 months and after 15 months of follow-up
Primary analysis: intended VATS lobectomy versus SBRT for the full cohort of patients
After matching, the cohort consisted of 159 patients in each treatment arm (table 4). Balance was assessed; differences between patients in both groups were minimal or absent. Interestingly, the most compromised intended VATS lobectomy patients were matched, i.e. those with higher age and greater comorbidity burden and CCI score than unmatched patients.
Characteristics of matched patients aged ≥65 years undergoing intended VATS lobectomy and SBRT for clinical stage I nonsmall cell lung cancer
The median follow-up for all matched patients was 33 months; for patients undergoing intended VATS lobectomy it was 35 months, and for those undergoing SBRT it was 32 months. The estimated median OS for patients undergoing intended VATS was 77 months (95% CI 59 months–NA, the upper limit of the 95% confidence band around the survival curve did not drop below 0.50) and for those undergoing SBRT it was 33 months (95% CI 30–37 months, p<0.001). The 1-, 3- and 5-year OS rates for patients undergoing intended VATS were 91%, 68% and 58%, and for patients undergoing SBRT were 87%, 46% and 29% (p<0.001, figure 1b). There was no difference in OS between the groups in the first 15 months of follow-up (HR 0.87, 95% CI 0.49–1.55). After 15 months, OS significantly favoured intended VATS lobectomy (HR 0.38, 95% CI 0.26–0.56, table 3).
Secondary analysis: intended VATS lobectomy versus SBRT for the subgroup of patients with data available on pulmonary function
After matching, the cohort consisted of 36 patients in each treatment arm (table 4). Balance was assessed; tumour stage cT1a and the non-matched variables histology and pathological confirmation were not well balanced (standardised differences ranging from 0.26 to 1.68). Interestingly, less compromised SBRT patients were matched, i.e. those with lower age, better pulmonary function, and a lower comorbidity burden and CCI score than unmatched patients.
The median follow-up for all matched patients was 38 months; for patients undergoing intended VATS lobectomy it was 42 months, and for those undergoing SBRT it was 33 months. The estimated median OS for patients undergoing intended VATS was 77 months (95% CI 68–86 months) and for those undergoing SBRT was 51 months (95% CI 26–76 months, p=0.087). The 1-, 3- and 5-year OS rates for patients undergoing intended VATS were 92%, 72% and 65%, and those for patients undergoing SBRT were 89%, 63% and 49% (p=0.087; adjusted for cT1a, histology and pathological confirmation p=0.034, figure 1c). There was no difference in OS between the groups in the first 15 months of follow-up (HR 1.23, 95% CI 0.38–4.03; adjusted for cT1a, histology and pathological confirmation HR 0.67, 95% CI 0.17–2.69). After 15 months, OS significantly favoured intended VATS lobectomy (HR 0.36, 95% CI 0.15–0.86; adjusted for cT1a, histology and pathological confirmation HR 0.30, 95% CI 0.11–0.81; table 3).
Discussion
This study demonstrates survival outcomes for patients aged ≥65 years with clinical stage I NSCLC diagnosed between 2010 and 2015 and treated with intended VATS lobectomy or SBRT. In unmatched and propensity score-matched primary analysis, median OS as well as 1-, 3- and 5-year OS was significantly better for those treated with intended VATS lobectomy than for those treated with SBRT. In the secondary analysis, in which pulmonary function was taken into account, the survival advantage related to intended VATS lobectomy persisted after adjusting for non-matched variables. This is in line with a number of previous studies comparing surgery with SBRT [14–16, 22], and studies specifically comparing VATS lobectomy with SBRT [23, 25].
Nevertheless, some studies reported no difference in survival between surgery and SBRT [9, 10, 12, 13, 18], even in patients with operable disease [11, 20, 30, 31]. Indeed, Lagerwaard et al. [20] reported 3- and 5-year OS rates of 85% and 51%, respectively, for patients with operable disease with stage I NSCLC treated with SBRT, which were similar to rates for surgery. A pooled analysis of the STARS and ROSEL trials suggests that both treatments are equally effective and the authors conclude that SBRT can be considered a treatment option in patients with operable disease who need a lobectomy [11]. A note of caution must be sounded because the STARS and ROSEL trials had different inclusion criteria, the analysis was underpowered due to a low number of patients and the trials had a short follow-up.
In both the primary and secondary analyses, there was no difference in OS between intended VATS lobectomy and SBRT in the first 15 months of follow-up. This could be explained by higher 30- and 90-day mortality after surgery compared to SBRT [32]. Mortality among surgical patients decreases after 90 days while it increases among patients undergoing SBRT. This might also explain why studies with a short follow-up do not find differences in OS between surgery and SBRT.
In the present study, intended VATS lobectomy patients with pathological stage I NSCLC had an excellent 5-year OS rate of 70%. Patients receiving SBRT had a significant survival disadvantage irrespective of matching. The higher OS after intended VATS lobectomy may be related to more complete tumour staging because a definite histological diagnosis is obtained. Pathological proof of malignancy was not obtained in 48% of patients receiving SBRT, which has been associated with inferior OS [3, 33]. Compromised pulmonary function and poor performance status may be reasons for deciding not to obtain pathological proof of malignancy and they are also associated with inferior OS [5, 34]. Higher OS after intended VATS lobectomy is probably not caused by selecting easy cases for VATS because almost two-thirds of surgically treated patients underwent VATS and one-third underwent thoracotomy between 2010 and 2015. After surgery, 22% of patients were upstaged: 52% of them received adjuvant treatment resulting in a 5-year OS of 52% compared to 39% among those not receiving adjuvant treatment. The higher OS for patients undergoing intended VATS lobectomy might in part be explained by the increased survival following adjuvant treatment. Previous studies investigating the effect of adjuvant chemotherapy endorse this finding; an absolute increase in 5-year OS of 4% was reported in a meta-analysis by Burdett et al. [35], and a 5-year OS gain of 15% has also been described [36]. Adjuvant treatment could be offered earlier to patients undergoing SBRT once pretreatment staging has been improved to enable accurate identification of nodal disease.
There are potential biases influencing outcomes in many previous studies even after propensity score matching. Often no distinction is made between patients treated by thoracotomy or VATS [9–17]. All patients with clinical stage I NSCLC who are ineligible for surgery can undergo VATS, i.e. this is independent of pulmonary function or comorbidities. VATS mitigates the risk of post-operative morbidity and mortality [5, 37], and could be useful in patients who cannot tolerate thoracotomy owing to compromised pulmonary function or multiple comorbidities [38, 39]. Many studies included mixed extents of resection [10, 13, 16–18], which precludes comparison because the extent of resection is related to the prognosis of NSCLC [40]. In addition, elderly patients with multiple comorbidities often cannot tolerate resection more extensive than lobectomy [5, 14, 22]. We argue that studies comparing surgery with SBRT do not provide a reliable answer to the question of which treatment strategy will result in better OS. An ongoing randomised study, NCT02357992, assesses the effectiveness of SBRT in patients with operable disease. Other randomised studies, including NCT01753414 and NCT00499330, are underway to examine the effectiveness of surgery versus SBRT and different types of surgical resection. The present study could form the basis of future trials comparing one type of minimally invasive surgical resection with SBRT.
The results of this study must be seen in the context of its strengths and limitations. One of the strengths is the availability of information on comorbidities, which is often lacking or not used for matching in other studies [10, 13, 16]. Furthermore, the patient population truly reflected clinical practice; in many clinical trials the population consists of selected, relatively fit patients. Our results are therefore more generalisable than reports from single centres. In addition, clinical staging was used for both patients undergoing intended VATS lobectomy and patients undergoing SBRT. Analyses from the Surveillance, Epidemiology and End Results (SEER) database use clinical stage for patients undergoing SBRT and pathological staging for patients undergoing surgery, which limits the generalisability of the results [22]. Limitations of this study include its retrospective study design and all limitations associated with propensity score matching, which does not ensure that all SBRT patients are good surgical candidates, and cannot account for unmeasured or unselected confounders [17]. In addition, the 68 patients in whom a conversion was recorded were analysed as having undergone VATS lobectomy. This could have influenced the outcomes, although differences in patient characteristics remained the same when the 68 patients with a conversion were excluded. We did not exclude these patients because this truly reflects daily clinical practice. Whether VATS lobectomy provides better long-term survival than thoracotomy is unclear. A recent study reported better long-term survival after VATS lobectomy [41] while another recent study did not find a significant difference [42]. Disease-free survival and cancer-specific survival are not recorded in the NCR, although these are important parameters in the long-term follow-up of elderly patients with early-stage NSCLC. Furthermore, the absence of data on performance status and paucity of data on pulmonary function limits the present study. Incomplete data on pulmonary function excluded the majority of patients for matching, resulting in a small group of matched patients for the secondary analysis. Another reason for this small group of matched patients was that the groups were different by nature; e.g. there were significant differences in age and number of comorbidities in the unmatched patients. Despite this limitation, every effort was made to reduce imbalance. Matching was done on many covariates and the small standardised differences obtained suggested adequate balance, which minimises the confounding effect [26, 27]. To account for the small but existing unbalance in the secondary analysis, we distinguished between matching on the selected variables with and without adjustment for the unbalanced variables. The caliper used eliminates at least 98% of the bias in the crude estimator [21]. Larger calipers used in other studies are likely to increase imbalance between subgroups, which favours surgery [17]. Despite matching as accurately as possible, selection bias was not completely nullified.
In conclusion, this analysis suggests that patients aged ≥65 years with clinical stage I NSCLC undergoing intended VATS lobectomy might have better OS than patients undergoing SBRT, irrespective of matching. This could be clinically important in decision-making, especially in elderly patients who can tolerate surgical resection. Despite matching, there are limitations to this observational analysis and randomised trials remain necessary before widespread implementation of SBRT in the treatment of patients with operable NSCLC.
Acknowledgements
The authors thank all registrars that registered the patients in the database, as well as the Netherlands Cancer Registry. They thank Winfried W.C. Gieskes (University of Groningen, the Netherlands) for revising earlier versions of the manuscript.
Footnotes
Conflict of interest: D.D.E.M.A. Detillon has nothing to disclose.
Conflict of interest: M.J. Aarts has nothing to disclose.
Conflict of interest: K. De Jaeger has nothing to disclose.
Conflict of interest: C.H.J. Van Eijck has nothing to disclose.
Conflict of interest: E.J. Veen has nothing to disclose.
- Received August 16, 2018.
- Accepted March 18, 2019.
- Copyright ©ERS 2019