



The potential impact of azithromycin in idiopathic pulmonary fibrosis
- Claudio Macaluso1,3,
- Joaquín Maritano Furcada1,3,
- Omamah Alzaher1,
- Ritesh Chaube1,
- Felix Chua1,
- Athol U. Wells1,
- Toby M. Maher1,2,
- Peter M. George1,
- Elizabeth A. Renzoni1 and
- Philip L. Molyneaux1,2
- 1Interstitial Lung Disease Unit, Royal Brompton Hospital, London, UK
- 2Fibrosis Research Group, National Heart and Lung Institute, Imperial College, London, UK
- 3These authors contributed equally to the study
- Philip L. Molyneaux, Fibrosis Research Group, National Heart and Lung Institute, Sir Alexander Fleming Building, Imperial College, London, SW7 2AZ, UK. E-mail: p.molyneaux{at}imperial.ac.uk
Abstract
Prophylactic azithromycin is a safe and well tolerated therapy in patients with IPF and may reduce hospital admissions. Prospective mechanistic studies are urgently needed. http://ow.ly/oBOn30mDaaL
To the Editor:
There is growing evidence of the role of infection in the pathogenesis and progression of idiopathic pulmonary fibrosis (IPF) [1–4]. Over a third of patients with IPF will be hospitalised, at least once, during the course of their disease [5]. These events not only carry a significant morbidity and mortality, but also a healthcare cost and burden [6]. Indeed, there is a growing recognition of these events as a potential marker for disease progression, reflected in the growing consensus to include such events as outcomes in future clinical trials [7]. Therefore, treatments that reduce the risk of hospitalisation could have a major impact. While recent evidence suggests that macrolide antibiotics may improve survival in acute exacerbations of IPF [8], to date there has been no study examining the potential role of prophylactic macrolides on reducing these emergency admissions or disease progression. This retrospective, observational study aimed to evaluate the impact of long-term azithromycin treatment in reducing hospitalisation rates in IPF patients.
We retrospectively identified all IPF patients receiving a prophylactic prescription of azithromycin 250 mg three times a week (Monday, Wednesday and Friday) between 2013 and 2016. The primary end-point was reduction in hospitalisations, with secondary end-points of use of rescue antibiotics, tolerability and side-effect profile. Prophylactic azithromycin was instigated by the treating clinician when patients reported three or more lower respiratory tract infections (or courses of antibiotics) in the preceding 12 months. The number of all-cause nonelective hospitalisation events and prescribed antibiotic courses were recorded for a period of 12 months before and after the commencement of therapy. A diagnosis of IPF was made following multidisciplinary discussion according to current international guidelines [9]. Patients with extensive radiological emphysema, an immunodeficiency, those receiving immunosuppressive therapy or using other prophylactic antibiotics were excluded. Approval for this study was obtained from the Institutional Ethics Committee of the Royal Brompton Hospital (London, UK). Continuous variables were assessed for normality and are presented as mean±sd, and categorical variables as proportions. Pulmonary function trends are expressed as percentage change from the start of therapy and changes were analysed using a paired T-Test or Wilcoxon signed-rank test.
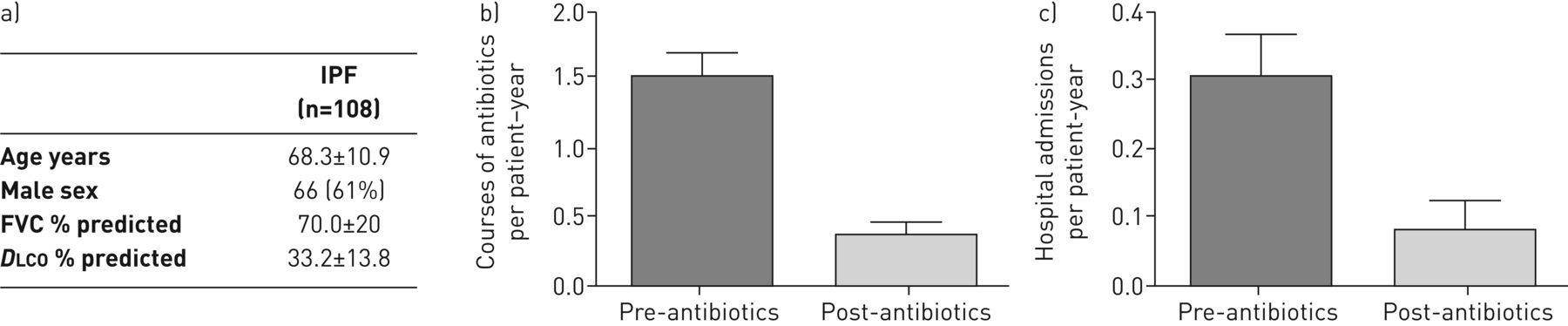
126 patients with IPF receiving prophylactic azithromycin were identified. 13 patients on concomitant immunosuppressive therapy and five receiving other prophylactic antibiotics were excluded. The remaining 108 IPF subjects had a mean age of 68.3±10.9 years, and were predominantly male (61%) with moderately severe disease (diffusing capacity of the lung for carbon monoxide (DLCO) 33.2±13.8% predicted; forced vital capacity (FVC) 70.0±20% predicted) (figure 1a). The median survival in the cohort was 29 months.
{kind=link}
a) Characteristics of the idiopathic pulmonary fibrosis (IPF) subjects. Comparison of b) courses of antibiotics (p=0.0086) and c) hospital admissions (p<0.0001) before and after the use of azithromycin per patient years. FVC: forced vital capacity; DLCO: diffusing capacity of the lung for carbon monoxide.
The majority of IPF patients tolerated azithromycin (93%) while only eight discontinued therapy due to side-effects (tinnitus (n=1) and gastrointestinal intolerance (n=7)) in the first 12 months. One patient stopped following lung transplant and four had therapy discontinued at the discretion of the prescribing clinician who felt there had been no subjective improvement (although these individuals were not excluded from the analysis). The cohort of patients on azithromycin tended to be younger (OR −0.96, p=0.006) and have a lower DLCO (OR −0.91, p=0.01) when compared to patients with IPF not prescribed prophylactic antibiotics. The strongest predictor, however, was previous number of antibiotics prescriptions (OR 3.2, p=1.77×10−6).
In the pre-treatment 12-month period, a total of 31 hospital admissions (0.29±0.62 per patient-year) and 176 courses of antibiotics (1.65±1.70 per patient-year) were recorded. In the same cohort a year after commencing prophylactic azithromycin, there were only seven hospital admissions (0.08±0.3 per patient-year) and 40 therapeutic antibiotic courses prescribed (0.44±0.8 per patient years) (figure 1b and c). This conferred a relative risk reduction in all-cause nonelective hospitalisation rates of 0.72 (0.67–0.88, p<0.001). The mortality in the 12 months following instigation of therapy was 16% (18 out of 108 patients). 10 patients died on a palliative pathway. A sensitivity analysis was performed reclassifying these deaths as either an admission or antibiotic course. This did not alter the relationship between azithromycin use and outcome. In the 12 months prior to azithromycin prophylaxis treatment, there was a median decline in FVC of −4.6% (−11.6–0.2%) and DLCO of −7.4% (−13.0–4.1%) predicted. The introduction of therapy did not have any significant impact on rate of decline in lung function, with a median decline in FVC of −2.5% (−13.2–4.4%) and DLCO of −8.4% (−18.75–5.5%) predicted in the following 12 months on therapy.
This study is the first to report that prophylactic antibiotics may be of benefit in reducing the burden of unplanned hospitalisations in patients with IPF. Whether these events act as a surrogate for acute exacerbations of IPF or are clinically important in their own right remains unclear. However, they appear fundamentally important to the natural history of IPF from the perspective of morbidity and mortality [7, 10]. The introduction of prophylactic antibiotics was well tolerated, associated with minimal side-effects and reduced the unplanned hospitalisation rate by over two thirds in this cohort. This reduction in admissions was achieved without impacting upon other well-established markers of disease progression including lung function. Whilst it is tempting to conclude that it is the antibacterial properties of azithromycin conferring this benefit, rather than the anti-inflammatory activity shown to be beneficial in animal models of lung fibrosis, this study does not allow us to definitively draw such conclusions.
Due to the retrospective nature of this work we could not accurately subclassify the cause of admissions (respiratory versus nonrespiratory) and therefore these events were left undifferentiated. The rates of all cause nonelective admissions across the CAPACITY and ASCEND trials was 18% [10, 11]. This is slightly lower than the rate observed in our cohort, which will have been enriched for those individuals prone to recurrent infections and therefore having higher numbers of admissions and antibiotic courses in the preceding year. These findings may not be generalisable to the IPF population as a whole and could reflect regression towards the mean. However, in patients with IPF prescribed multiple courses of antibiotics in the preceding 12 months this therapy was well tolerated and had a potentially clinically significant impact. Extensive microbiological data is not available and therefore not reported; however, any prospective studies must include robust microbiological sampling and analysis. The retrospective nature also means that some antibiotic courses will not have been captured, and explains the discrepancy in patient-reported and objective evidence of prescribed courses of antibiotics or lower respiratory tract infections.
This study clearly demonstrates that prophylactic azithromycin is a safe and well-tolerated therapy in individuals with IPF. In patients whose disease course is punctuated with multiple infective episodes, prophylactic antibiotic therapy may provide a beneficial effect with a decrease in both hospital admissions and rescue antibiotic usage. Prospective randomised placebo-controlled studies are needed to support and confirm our findings, while further mechanistic work is needed to delineate the exact pathways by which macrolides confer this benefit.
Footnotes
Author contributions: P.L. Molyneaux and E.A. Renzoni planned the project; P.L. Molyneaux analysed the data and wrote the manuscript; C. Macaluso, J. Maritano Furcada, O. Alzaher and R. Chaube collected data, performed statistical analyses, interpreted the results and helped write the manuscript; and F. Chua, A.U. Wells, T.M. Maher and P.M. George analysed the data and helped write the manuscript. All authors reviewed, revised and approved the manuscript for submission.
Conflict of interest: C. Macaluso has nothing to disclose.
Conflict of interest: J. Maritano Furcada has nothing to disclose.
Conflict of interest: O. Alzaher has nothing to disclose.
Conflict of interest: R. Chaube has nothing to disclose.
Conflict of interest: F. Chua has nothing to disclose.
Conflict of interest: A.U. Wells reports speaker's and consultancy fees from Intermune Roche, Boehringer Ingelheim and Bayer.
Conflict of interest: T.M. Maher has, via his institution, received industry-academic funding from GlaxoSmithKline R&D and UCB, and has received consultancy or speaker's fees from Apellis, AstraZeneca, aTyr Pharma, Bayer, Biogen Idec, Boehringer Ingelheim, Galapagos, GlaxoSmithKline R&D, ProMetic, Roche, Sanumed and UCB.
Conflict of interest: P.M. George reports receiving honoraria and speaker's fees from Roche Pharmaceuticals and Boehringer Ingelheim, outside the submitted work.
Conflict of interest: E.A. Renzoni has received speaker's fees from Boehringer Ingelheim, Roche and Mundipharma.
Conflict of interest: P.L. Molyneaux has nothing to disclose.
Support statement: T.M. Maher is supported by an National Institute for Health Research (NIHR) Clinician Scientist Fellowship (NIHR ref. CS-2013-13-017) and a British Lung Foundation Chair in Respiratory Research (C17-3). The project was supported by the NIHR Respiratory Disease Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
- Received April 5, 2018.
- Accepted October 27, 2018.
- Copyright ©ERS 2019