



Intensity of exposure to pulmonary tuberculosis determines risk of tuberculosis infection and disease
- Carlos Acuña-Villaorduña1⇑,
- Edward C. Jones-López1,
- Geisa Fregona2,
- Patricia Marques-Rodrigues2,
- Mary Gaeddert1,
- Carolina Geadas1,
- David Jamil Hadad2,
- Laura F. White3,
- Lucilia Pereira Dutra Molina2,
- Solange Vinhas4,
- Rodrigo Ribeiro-Rodrigues5,
- Padmini Salgame6,
- Moises Palaci2,
- David Alland6,
- Jerrold J. Ellner1 and
- Reynaldo Dietze2
- 1Section of Infectious Diseases, Dept of Medicine, Boston Medical Center and Boston University School of Medicine, Boston, MA, USA
- 2Núcleo de Doenças Infecciosas, Universidade Federal do Espírito Santo, Vitória, Brazil
- 3Dept of Biostatistics, Boston University School of Public Health, Boston, MA, USA
- 4Mycobacteriology Laboratory, Núcleo de Doenças Infecciosas, Universidade Federal do Espírito Santo, Vitória, Brazil
- 5Cellular and Molecular Immunology Laboratory, Núcleo de Doenças Infecciosas, Universidade Federal do Espírito Santo, Vitória, Brazil
- 6Dept of Medicine, Rutgers New Jersey Medical School, Newark, NJ, USA
- Carlos Acuña-Villaorduña, Section of Infectious Diseases, Boston Medical Center and Boston University School of Medicine, 650 Albany Street, EBRC Suite 625, Boston, MA 02118, USA. E-mail: carlos.acuna-villaorduna{at}bmc.org
Abstract
Household contacts of pulmonary tuberculosis (TB) patients are at increased risk of TB infection and disease. However, their risk in relation to the intensity of exposure remains unknown.
We studied smear-positive TB cases and their household contacts in Vitória, Brazil. We collected clinical, demographic and radiographic information from TB cases, and obtained tuberculin skin test (TST) and QuantiFERON-TB Gold (QFT) results from household contacts. We measured intensity of exposure using a proximity score and sleep location in relation to the TB index case and defined infection by TST ≥10 mm or QFT ≥0.35 UI·mL−1. We ascertained secondary TB cases by reviewing local and nationwide case registries.
We included 160 TB index cases and 894 household contacts. 464 (65%) had TB infection and 23 (2.6%) developed TB disease. Risk of TB infection and disease increased with more intense exposures. In an adjusted analysis, the proximity score was associated with TB disease (OR 1.61, 95% CI 1.25–2.08; p<0.000); however, its diagnostic performance was only moderate.
Intensity of exposure increased risk of TB infection and disease among household contacts; however, its diagnostic performance was still suboptimal. A biomarker to target preventive therapy is urgently needed in this at-risk population.
Abstract
More intense exposures are associated with higher risk of TB infection and disease among close contacts of TB cases http://ow.ly/PnQW30gapxK
Introduction
Close contacts of sputum acid-fast bacilli (AFB) smear-positive tuberculosis (TB) patients are at increased risk of TB infection and disease [1]. In high-incidence settings, 50% of household contacts of TB patients are infected with Mycobacterium tuberculosis and 4% will eventually develop active TB disease within 1 year [2]. It is estimated that interventions targeted at the household level could prevent over a quarter of a million cases of TB per year (especially among children and patients infected with HIV [3–5]) and are therefore an important strategy in controlling TB transmission [6].
The Stop TB Strategy of the World Health Organization recommends household contact investigations for active screening of TB disease among contacts of smear-positive TB cases, as well as isoniazid preventive therapy for children aged <5 years and those with a positive tuberculin skin test (TST) or interferon-γ release assay (IGRA) [5]. However, despite the potential public health benefits, household contact investigations are rarely performed in resource-constrained settings [7]. Absence of data on effectiveness and lack of clear definitions of contacts at highest risk have been suggested as barriers against household contact investigations implementation by national TB control programmes. A strategy that allows national TB control programmes to identify household contacts at highest risk of progression to TB disease would be of great value to optimise resources and prevent unnecessary exposure to potentially toxic drugs.
In this study, we report the rates of TB infection and secondary TB disease among household contacts of smear- and culture-positive pulmonary TB cases, in relation to the intensity and location of their exposure. Our findings identify subsets of household contacts at higher risk for M. tuberculosis infection and disease.
Methods
Study population
The study was conducted between February 2008 and October 2013 at the Núcleo de Doenças Infecciosas (NDI) in Vitória, the capital city of the State of Espírito Santo, Brazil. The NDI comprises a network of five laboratories in the metropolitan region of Vitória that serve 16 municipal TB clinics. With approximately 1400 new cases per year, the annual incidence of TB in Espírito Santo is 38 per 100 000 inhabitants. The prevalence of HIV infection is <1% in the general population and 7% in TB cases [8].
Index TB cases
Pulmonary TB patients identified consecutively through the NDI clinic network were eligible to participate if they fulfilled the following inclusion criteria: 1) age ≥18 years, 2) cough ≥3 weeks duration, 3) new TB episode with at least one sputum specimen with AFB smear 2+ or 3+ and positive culture for M. tuberculosis, and 4) living with three or more household contacts. Index cases were excluded if they were HIV infected, refused HIV testing, had a history of TB treatment, or were too ill to consent, unable to understand or to comply with the study protocol.
Household contacts
Household contacts were defined as an individual of any age fulfilling at least one of the following criteria of close contact with the index TB case for ≥3 months before enrolment: 1) sleeping under the same roof ≥5 days per week, 2) sharing meals ≥5 days per week, 3) watching TV together on week nights or weekends and 4) other significant contact (85% of these visited the household ≥18 days per month).
We followed recommendations of the Brazilian TB control programme for household contact investigations [9]. We recorded demographic and clinical characteristics of household contacts, and evaluated them for M. tuberculosis infection with both the TST and IGRA (QuantiFERON-TB Gold (QFT); Qiagen, Germantown, MD, USA). We placed 2 IU of R23 (Statens Serum Institut, Copenhagen, Denmark; provided by the Brazilian Ministry of Health) on the forearm of contacts using the Mantoux method. Induration was measured in millimetres 72 h after placement. Household contacts with TST <10 mm at baseline were retested after 8–12 weeks to identify TST conversion. At 8–12 weeks, blood for IGRA testing was obtained before TST placement to reduce TST-induced IGRA boosting. Household contacts with TST ≥10 mm or QFT ≥0.35 UI·mL−1 were referred to the national TB control programme for evaluation and preventive therapy according to national guidelines [9]. We defined TST positivity as those who had either 1) an initial TST ≥10 mm or 2) TST conversion according to the Brazilian national TB control programme guidelines (increase ≥10 mm between first and second TST).
Intensity of exposure
Study staff visited the participants' dwellings to perform an environmental evaluation, to verify the identity of each contact and to measure individual contact time with the TB index case that included: 1) sleeping proximity (same bed, same room but different bed, same house but different room or different house), 2) biological (father, mother, etc.) or social relationship (spouse), 3) average number of days per month of contact, 4) average number of hours per day nursing the index case and 5) number of meals shared per day.
Proximity score
To quantify M. tuberculosis exposure in a standardised way and to capture the effect of cumulative risk factors of proximity, we used a modified version of the Mandalakas score to measure risk of infection [10]. The score consists of 10 clinical variables that have been shown to correlate with an increased risk of M. tuberculosis infection. Index factors include: presence of cough, pulmonary TB, smear positivity and if the index case was household contact's primary caregiver or mother. Contact factors include: sleep location and living in the same house as the index TB case. Initially developed to measure risk of infection in children, we modified the score for use in household contacts >15 years old. Rather than considering “mother as the index case” a risk category, we considered “spouse as the index case”. We did not collect information on primary caregiver status, instead we used time >6 h of nursing time as a surrogate variable. We chose this value as it represented the upper quartile range of exposure in our population (see supplementary material).
Secondary cases
In June 2015 (21 months after enrolment conclusion), we searched the Vitória TB control programme records and the nationwide notifiable disease information system (SINAN (Sistema de Informação de Agravos de Notificação)) database for the name, address and date of birth of all household contacts that had been enrolled in the study to identify those that had developed subsequent TB. For those identified as TB cases, information was obtained on diagnosis date, AFB smear-culture results and history of isoniazid preventive therapy. TB cases occurring ≥3 months after the TB index case diagnosis were considered incident or secondary TB cases. For our primary analysis, we included all household contacts with TB diagnosis. We defined microbiologically confirmed TB as household contacts with a positive AFB smear or culture.
Statistical methods
We compared the proportion of TST positivity and IGRA (QFT ≥0.35 UI·L−1) positivity at 8–12 weeks for each level of exposure and biological relationship to the index case. Using the modified Mandalakas score, we calculated the proportion of household contacts with TB infection and secondary TB disease in relation to their score grading. We also calculated the area under the receiver operating characteristic curve (AUC) to evaluate the accuracy of the score in predicting each outcome of interest. We constructed logistic regression models fit using generalised estimating equations to evaluate the association between intensity of exposure and incident TB disease. Variables with p<0.1 and those deemed clinically relevant (bacille Calmette–Guérin (BCG) status of the contact, sputum smear grade and presence of cavitation on chest radiograph of the TB index case) were included in the model. Time to event was measured crudely, so we did not use a time-to-event model. All analyses were performed using Stata version 14.0 (StataCorp, College Station, TX, USA).
Ethics approval
The study was approved by the Comitê de Ética em Pesquisa do Centro de Ciências da Saúde, Universidade Federal do Espírito Santo, the Comissão Nacional de Ética em Pesquisa, and the Institutional Review Board of Boston University Medical Center and Rutgers New Jersey Medical School, Rutgers University (formerly University of Medicine and Dentistry of New Jersey). We obtained written informed consent and assent in Portuguese according to the age-specific guidelines of participating institutions.
Results
We identified 277 potentially eligible index cases through the NDI clinic network. 160 met the inclusion criteria (figure 1). Index cases were mainly male (n=107 (67%)) of middle age (median (interquartile range (IQR)) age 36 (24–45) years), and with advanced TB disease as indicated by smear grade 3+ in 120 (76%) cases and presence of cavities in 126 (80%) cases.

Study profile. TST: tuberculin skin test; IGRA: interferon-γ release assay; TB: tuberculosis; HHC: household contact.
934 household contacts were identified, of which 40 (4.3%) were excluded because of refusal to participate (n=26) or lack of information on intensity of exposure (n=14). The 40 excluded contacts were more likely to be male (60% versus 40%; p=0.05) and older (median age 28 versus 21 years; p=0.03). Household contacts were mostly young (median (IQR) age 27 (12–40) years) females (n=412 (58%)). None of them reported diagnosis of HIV infection, four (0.4%) had cancer, three (0.3%) had renal failure and 20 (2%) had diabetes mellitus.
Intensity of exposure and TB infection
710 household contacts (80%) had complete information on TST and IGRA results. 413 (58%) had initial TST ≥10 mm and 51 (7%) were TST converters, therefore 464 (65%) had TST positivity according to our definition and 418 (59%) had QFT ≥0.35 UI·L−1. Agreement between TST/IGRA was moderate (79.4%, κ=0.56) and did not change significantly when TST/IGRA cut-offs were changed (supplementary table S1). Baseline characteristics of 710 household contacts are shown in table 1.
Baseline characteristics of 710 household contacts with complete tuberculin skin test (TST)/interferon-γ release assay (IGRA) information
TST and IGRA positivity rates were similar among household contacts with intense exposures, such as those who slept in the same bed as the index case (81% versus 77%), slept in the same room (69% versus 67%), spouse of the TB case (77% versus 72%) or shared meals (70% versus 67%). TST positivity was more common than IGRA positivity among household contacts with less intense exposure, such as those living in different household (57% versus 43%) and those without daily contact with the TB case (51% versus 39%).
Proximity score and TB infection
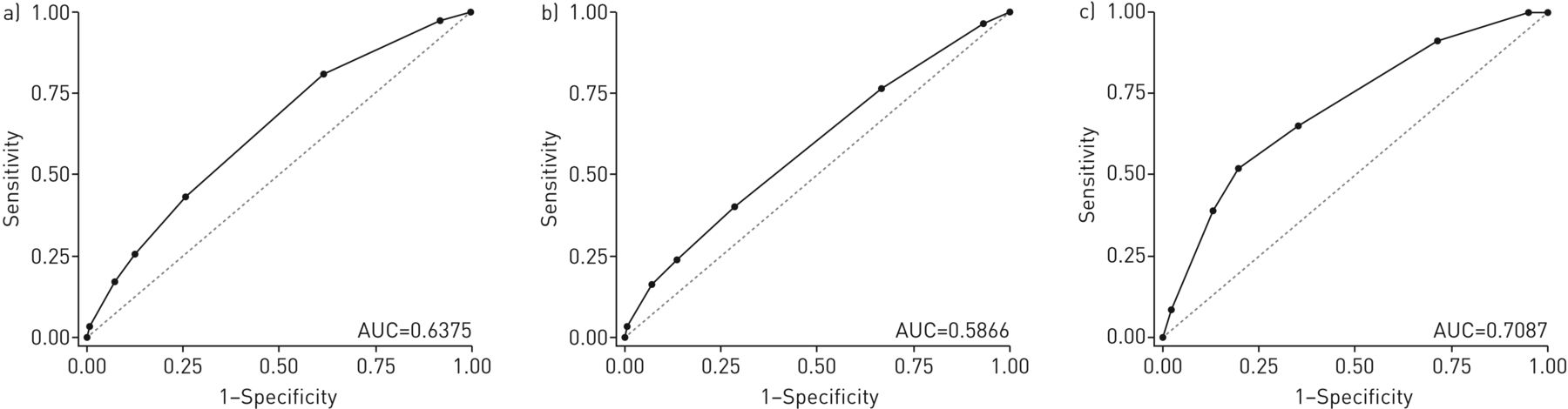
The modified Mandalakas score ranged from 3 to 9 (median (IQR) 5 4–6). The proportion of TST and IGRA positivity, TST induration sizes, and quantitative IGRA readouts increased with higher exposure score values (table 2). Household contacts with less intense exposures (score 3) were 48% TST+ and 30% IGRA+. Household contacts with intense exposures (score 9) were 94% TST+ and 88% IGRA+. The AUC for the proximity score was 0.59 (95% CI 0.54–0.63) to detect TST positivity and 0.64 (95% CI 0.60–0.68) for QFT ≥0.35 UI·L−1 (figure 2).
Modified Mandalakas score, tuberculin skin test (TST)/interferon-γ release assay (IGRA) positivity and secondary tuberculosis (TB) cases among household contacts

Receiver operating characteristic (ROC) curves of proximity score to predict a) interferon-γ release assay positivity, b) tuberculin skin test positivity and c) incident tuberculosis disease among close contacts. AUC: area under the ROC curve.
Intensity of exposure and TST/IGRA discordance
132 (19%) of household contacts had TST/IGRA discordance. 89 (13%) were TST+/IGRA− and 43 (6%) were TST−/IGRA+. In an unadjusted analysis that compared TST+/IGRA− and TST+/IGRA+ contacts, the former was associated with: older contact age (median age 31 versus 21; p=0.008) and lower proximity score (median (IQR) 5 (4–5) and 5 (4–6); p=0.001). In an adjusted analysis, TST+/IGRA− discordance was associated with: older contact age (p=0.02) and lower proximity scores (p=0.001) (supplementary table S2). In a stratified analysis, the proportion of contacts with TST+/IGRA− discordance was similar in BCG-vaccinated and unvaccinated household contacts (supplementary table S3). Importantly, TST+/IGRA− discordance was more common for household contacts sleeping outside the household (17%) compared with those sharing a room (7%) or a bed with the TB index case (11%) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Tuberculin skin test (TST) and interferon-γ release assay (IGRA) discordance among close contacts according to sleeping proximity to the index tuberculosis case. PPD: purified protein derivative.
Intensity of exposure and secondary TB cases
Of 894 household contacts, 140 (16%) had received isoniazid preventive therapy. Household contacts <15 years of age were more likely to receive isoniazid preventive therapy compared with contacts ≥15 years of age (26% versus 10%; p=0.001). After a median follow-up of 5.1 years, 36 (4.1%) TB cases were identified. 23 (2.6%) were secondary TB cases and 13 (1.5%) were coprevalent TB cases according to our definition. 18 (78%) TB cases were microbiologically confirmed. The proportion of secondary TB cases increased with higher exposure scores (table 2). Similarly, TB incidence was higher among household contacts sharing a bed and room with the index TB case compared with those sleeping in a different room or outside the household (table 3). In an adjusted analysis, the exposure proximity score (OR 1.61, 95% CI 1.25–2.08; p<0.000) and age >15 years (OR 5.33, 95% CI 1.24–23.01; p=0.03) were associated with an increased risk of secondary TB disease (table 4). The AUC for the proximity score to predict TB disease was 0.71 (95% CI 0.60–0.82). In an analysis that included only the microbiologically confirmed TB cases, the proximity score was also associated with microbiologically confirmed TB disease (OR 1.36, 95% CI 1.02–1.82; p=0.04) (supplementary table S4).
Secondary tuberculosis (TB) among household contacts by location of exposure
Factors associated with incident tuberculosis (TB) disease among household contacts of smear-positive TB patients
Discussion
In this household contact study of smear-positive culture-proven pulmonary TB cases conducted in a setting with moderate incidence of TB, we found a direct relationship between intensity of exposure, measured by a proximity score and sleep location in relation to the TB index case, and TST/IGRA responses and secondary TB disease among household contacts. The association between intensity of exposure and risk of TB infection/disease was independent of other known factors that increase the risk of TB infection among household contacts, such as presence of cavities or smear status of the index case.
There is marked variability in infection rates among close contacts of TB patients [11, 12]. Efforts to explain this variability have focused on index factors (cough strength) [13], genetic predisposition of the contact and, more recently, bacterial factors [14]. However, close contact to an infectious TB case is known to be the strongest predictor for M. tuberculosis infection and the second strongest after HIV infection for TB disease [15]. Proximity can be considered a surrogate marker for the infectious dose, and thus household contacts with more intense contact such as those sharing the same room/bed with the TB index case were more likely to have larger and more constant exposures to infectious M. tuberculosis aerosols, leading to stronger TST/IGRA responses and subsequently to more risk of progression to TB disease. The concept that the size of the infectious inoculum modulates the risk of infection and disease has been well documented in other infectious pathogens [16], and is supported by several animal models where a dose relationship is observed between the infectious aerosol M. tuberculosis inoculum and the risk and severity of TB disease [17, 18].
The association between proximity and risk of TB infection has been reported in high-incidence settings [19, 20]. Nevertheless, in the absence of a refined marker of infectiousness, it is not possible to determine whether household contacts with high-intensity exposures were more likely to be exposed to repetitive doses of the same inoculum or to a single larger infectious inoculum. The seminal pathological observation that a single focus leads to primary TB infection supports the concept that a single infectious unit is enough to initiate the infection and probably confer some degree of protection against repetitive infections [21]; this is highlighted by a recent outbreak in children <5 years of age where a short contact (<15 min) with an infectious case was enough to produce TB infection and disease [22]. In addition, during a TB outbreak in Canada, TB disease was associated with the number of times the contact was exposed to a TB case, suggesting a role for multiple exposures in progression to TB disease [23]. At present, the effect of repetitive low-dose or single high-dose infectious inoculum of M. tuberculosis in granuloma formation or if a threshold effect exists for the risk of progression to TB disease remain unknown.
Despite the increased risk of TB infection and disease with more intense exposures, the Mandalakas score performed rather poorly in predicting TB infection and only moderately predicted TB disease as measured by the AUC. If national TB programmes decide to focus investigations on contacts that sleep in the same room as the index TB case, this would decrease the burden of contact investigation by 76%; however, opportunities for preventive therapy will be missed for eight out of 23 secondary TB cases (sensitivity 65% and specificity 77%). Several biomarkers have been proposed for risk stratification of latent TB infection outcome, including nonspecific inflammatory proteins and imaging studies [21]. A newly developed gene signature obtained from blood samples achieved 62% sensitivity and 80% specificity to predict TB disease among high-risk patients in South Africa [24]. The question whether national TB programmes should target isoniazid preventive therapy based on proximity or by implementing blood-based biomarkers is an important area for further research.
Interestingly, TST−/IGRA+ discordance was uncommon and not related to intensity of exposure, an effect that might be due to internal variability in IGRA results or idiosyncratic immune responses in the exposed contact [25]. However, we found 13% TST+/IGRA− discordance, which was more pronounced with less intense exposures. Our findings are consistent with previous reports from Korea and South Africa [26, 27], where QFT correlated better with the degree of exposure than TST among low-risk (nonexposed) and high-risk (close contacts) individuals, and confirm that even among household contacts of smear-positive TB cases, the infectious dose appears to modulate TST/IGRA response, with faster and stronger readouts following more intense exposures (an effect that is independent of the BCG status of the contact). Taken together, these data suggest that TST could be more sensitive than QFT to detect lower intensity exposures or that QFT is a better marker of bacterial replication. Recently, a new QFT formulation (QuantiFERON-TB Gold Plus), which includes an additional tube to detect CD8 T-cell cytokine production, showed stronger association with measures of exposure than QFT, with a possible 17% increased sensitivity for low-intensity exposures [28]. The role of CD8 T-cell responses as a marker of bacterial load and recent TB infection is an area of current research. Likewise, future studies should address the role of qualitative differences in TB infection [29], a concept that is supported by reports showing that TST+/IGRA+ individuals are at higher risk of progression to TB disease compared with those with discordant results [30–31].
Our study has limitations. First, we were unable to obtain information on TST/IGRA for 224 household contacts. Selection bias could have occurred if the excluded population had a different level of exposure with regard to TST/IGRA responses and secondary TB disease compared with the study population. Second, our definition of secondary TB cases was based on the review of two databases, which account for all TB diagnosis reported in the community; however, it is possible that some TB cases may have been missed, especially those with clinically diagnosed TB, leading to outcome misclassification. Third, the proximity score was developed for children at South Africa and has not been validated in other settings. Furthermore, household contacts were mainly young with low rates of comorbidities and, therefore, our results may not be applicable to settings with higher rates of comorbidities, especially HIV infection. Finally, we did not have access to genotypic testing to confirm that secondary TB cases originated from the index TB case in the household; however, Vitória is a setting with moderate TB incidence and thus we expect that most of the secondary TB cases originated from the household TB index case.
Conclusions
We found that among close contacts of pulmonary TB cases, more intense exposures are associated with increased risk of TB infection, improved TST+/IGRA+ concordance and higher risk of progression to TB disease; however, the diagnostic accuracy to predict each outcome is limited. A biomarker with moderate accuracy to predict TB disease is urgently needed to guide targeted isoniazid preventive therapy in this at-risk population.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Mandalakas score components, and supplementary tables ERJ-01578-2017_Supplementary_material
Disclosures
Acknowledgements
Author contributions: Conception and design: C. Acuña-Villaorduña, E.C. Jones-López, R. Ribeiro-Rodrigues, M. Palaci, D. Alland, J.J. Ellner and R. Dietze. Acquisition of data: E.C. Jones-López, G. Fregona, P. Marques-Rodrigues, D.J. Hadad, M. Gaeddert, L. Pereira Dutra Molina, S. Vinhas and R. Dietze. Analysis and interpretation: C. Acuña-Villaorduña, E.C. Jones-López, M. Gaeddert, L.F. White, C. Geadas, J.J. Ellner and R. Dietze. All authors contributed to either drafting or revising the manuscript and gave final approval. C. Acuña-Villaorduña had full access to all the data in the study, and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Support statement: This work was supported by the National Institute of Allergy and Infectious Diseases at the National Institutes of Health (NIH) awards U01AI065663-01 (International Collaboration in Infectious Diseases Research) and U19AI111276 (TB Research Unit Network); funds from the Section of Infectious Diseases at Boston Medical Center and Núcleo de Doenças Infecciosas, Universidade Federal do Espírito Santo. The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript. The content is the sole responsibility of the authors and does not necessarily represent the official views of the NIH. Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
- Received August 2, 2017.
- Accepted October 20, 2017.
- Copyright ©ERS 2018