



Cellular analysis in bronchoalveolar lavage: inherent limitations of current standard procedure
- Benjamin-Alexander Bollmann1,
- Benjamin Seeliger1,
- Nora Drick1,
- Tobias Welte1,2,
- Jens T. Gottlieb1,2 and
- Mark Greer1,2⇑
- 1Dept of Respiratory Medicine, Hannover Medical School, Hannover, Germany
- 2Biomedical Research in End-Stage and Obstructive Lung Disease (BREATH), German Centre for Lung Research (DZL), Hannover, Germany
- M. Greer, Dept of Respiratory Medicine, Hannover Medical School, Carl-Neuberg-Straße 1, 30625 Hannover, Germany. E-mail: greer.mark{at}mh-hannover.de
Abstract
The “dead-space” concept: bronchoscope size and instillation protocol significantly alter BAL cellular composition http://ow.ly/ZEaj30be7HV
Bronchoalveolar lavage (BAL) is an established procedure for diagnosing respiratory infections and characterising non-infective lung diseases [1]. Increasingly, emphasis has been placed on BAL cellular composition in the diagnostic algorithms for interstitial lung disease [2] and chronic lung allograft dysfunction following lung transplantation [3].
Despite its widespread use and the broad consensus arising on basic principles, several known sampling problems undermine the comparability of BAL results. The composition of the alveolar lining fluid (ELF) is influenced by the effects of lung permeability on BAL recovery, contamination by bronchial fluid, as well as dilution factors related to the BAL technique. Current recommendations include reporting differential proportions for cellular components and using a standard number of four aliquots and ≥100 mL instillation volumes [1]. Given the open interpretability of these recommendations, great variations in local procedure are known to occur [2].
This study examines further the influences of aliquot number and bronchoscope lumen diameter in a fixed-volume protocol as potential dilution factors in BAL analysis.
Lung transplant (LTx) recipients attending our centre for outpatient bronchoscopy were prospectively evaluated. All attendees were invited to participate, with those enrolled providing written informed consent. The local ethics committee approved the study (no. 3068-2016). Samples with ≥4% epithelial cells were considered contaminated and excluded.
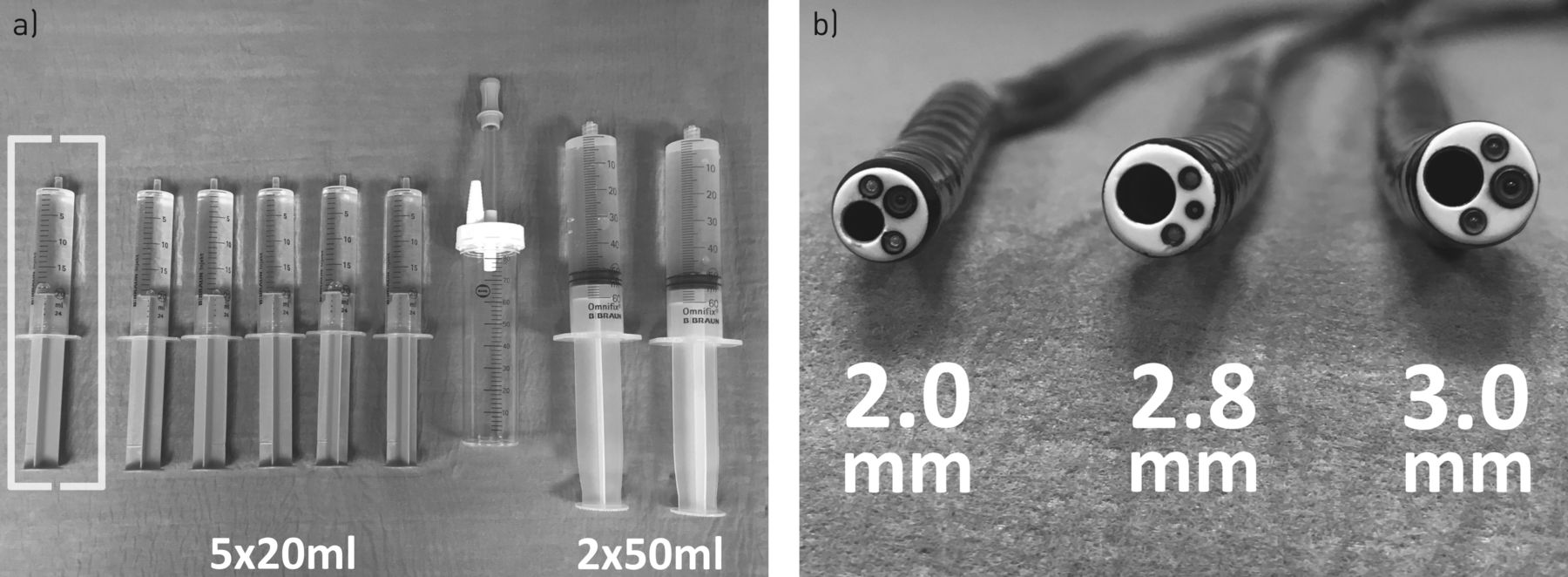
Flexible video bronchoscopy (Olympus Corp., Japan) was performed via nasal intubation using topical anaesthesia in conscious patients as described previously [4]. The standardised BAL technique involved bronchoscope wedging at the segmental level. The BAL site was based on same-day chest radiography, with normal images resulting in choosing either the middle lobe or lingula. Fluid instillation consisted of either six aliquots of 20 mL 0.9% saline, with the first being discarded (5×20 mL), or two aliquots of 50 mL saline without initial discarding (2×50 mL), via the instrument channel (figure 1a). Alternate-day use of protocols served as the randomisation procedure. Sample recovery was identical in both protocols, and utilised a Medela Basic 30 suction pump (Medela AG, Baar, Switzerland) set at −100 mmHg and standard 80 mL plastic BAL canisters (Mucous Specimen Trap, C.R. Bard Inc., Crawley, UK) connected to the suction port. Specimens were transferred directly from the bronchoscopy suite to our adjacent BAL cytology laboratory for immediate processing. Samples were filtered prior to centrifugation at 1100 rpm for 10 min and the resulting pellet was added to 1 mL phosphate-buffered saline. Staining with 90 µL of Türk's solution (Sigma–Aldrich GmbH, Munich, Germany) containing gentian violet and 1% acetic acid and 10 µL cell suspension was performed prior to plating for manual microscopy.

{kind=link}
a) Pre-filled syringes as used in both protocols, together with the canister used to collect the recovered bronchoalveolar lavage (BAL). Discard syringe is shown in square parentheses. b) The differences in cross-sectional diameter of the various instrument channels used in the study.
All samples underwent additional microbiological analysis, with virology only being performed when clinically suspected.
Lower airway colonisation was considered present if previous BAL cultures had yielded ≥103 colony-forming units in the absence of clinical evidence for infection. Microorganisms were classified in accordance with previous studies as either pathogenic, having been recognised as causing respiratory infections, or normal commensals of the oropharyngeal or gastrointestinal flora [5]. Chronic lung allograft dysfunction was staged using current International Society for Heart and Lung Transplantation criteria [6].
Statistical analysis was performed using SPSS 24 (IBM Corp., Armonk, NY, USA). Non-parametric distributions were assumed, with continuous variables being expressed as median (interquartile range) and were analysed using the Mann–Whitney U test or Kruskal–Wallis H test. The Fisher exact test was used for categorical variables. Calculated p-values are two-tailed, with p<0.05 considered significant.
In total, 100 patients were enrolled between February 10, 2016 and March 24, 2016, the majority (65%) being in the 2×50 mL group. No difference in patient demographics was evident between groups. Emphysema was the leading diagnosis in both groups and 95 (95%) had received bilateral grafts. Five patients (5%) had undergone re-do transplantation.
Most procedures (62%) were performed on stable patients undergoing routine surveillance or follow-up control (table 1). The remaining 38 procedures were performed due to deteriorating graft function with or without symptoms of infection, with rates being similar in both protocols.
Summarising bronchoscopy features and outcomes between groups. The 2×50 mL protocol demonstrated lower yields in bronchoalveolar lavage (BAL) recovery but higher levels of cellularity.
No difference in physician experience existed between protocols (p=0.84), and the choice of BAL site was similar in both groups, with the majority being performed in the middle lobe (71 versus 60%; p=0.35). The median duration of bronchoscopy was marginally shorter in the 2×50 mL group (10 versus 12 min; p=0.12). Safety profiles were similar in both groups. Two patients were admitted following bronchoscopy, but neither because of the procedure. One required intravenous antibiotics and the other urgent investigation of a suspected tumour.
Instrument channel diameter in the bronchoscope varied between 2.0 and 3.0 mm (figure 1b). All were of identical length (600 mm), resulting in an instrument channel volume of between 1.88 and 4.24 mL. The impact of this is worth considering, because 3.8–21.2 mL of BAL fluid recovered was airway naive, having never left the bronchoscope. No differences in scope selection were seen between protocols (p=0.53).
Concerning BAL recovery, significantly larger volumes were returned in the 5×20 mL protocol (64 versus 44 mL; p<0.001). Conversely cellular concentration was lower in this group (89 versus 127 cells·µL−1; p=0.02). Higher proportions of neutrophilia (p=0.03) and lymphocytosis (p=0.04) were evident in the 2×50 mL group. Correcting for “bronchoscope dead-space”, differences in both BAL recovery (38.6 versus 46.7 mL; p=0.001) and aspirate cellularity (154 versus 117 cells·µL−1; p=0.03) were maintained. Sub-analysis correcting for lumen size continued to demonstrate higher BAL return in the 5×20 mL protocol (3.0 mm: 34 versus 61 mL, p=0.017; 2.8 mm: 43 versus 64 mL, p<0.001; 2.0 mm: 47 versus 61 mL, p<0.001). Compensating again for dead-space, differences only remained significant for the two smaller lumen sizes. Similarly, although median cell counts were consistently higher in the 2×50 mL group for all scope sizes, only the smallest 2.0 mm instrument channel proved significant (249 versus 123 cells·µL−1; p=0.03).
To exclude any differences in BAL cellular vitality between protocols, Tryptan blue staining was performed on a further 14 samples obtained using each protocol. Median cell vitality was similar in both groups (93% 2×50 mL versus 94% 5×20 mL; p=0.49).
In terms of their influence on clinical outcomes, no practicable difference was evident between protocols within the cohort (p=0.51). Neither protocol proved superior in detecting viral, bacterial or fungal infections. Most infections in both groups were viral, with the most common pathogens being respiratory syncytial virus (RSV, n=8) and influenza (n=6). Rates of detection of pathogenic bacteria (p=0.97) and culture counts (p=0.566) were similar with both protocols.
Despite its prospective nature, there are several notable limitations in study design, most notably its observational nature and the small number of participants. Patient inclusion was a priori within a busy LTx follow-up programme and the randomisation procedure, although not ideal, reflected this. No differences in attendance patterns were observed over the study period compared to the remainder of 2016 (1081 bronchoscopies, p=0.46).
In conclusion, although the selected BAL protocols had minimal impact on daily decision-making, this small study addresses some of the shortcomings of current BAL guidelines regarding certain dilution factors. Given an increasing emphasis on BAL cytology in disease classification, refinement of current recommendations to compensate for both instillation protocol and scope size may be appropriate. A clear and precise consensus on BAL protocol or at least standardised reporting of results appears essential to improve the comparability of results.
Disclosures
Supplementary Material
J. T. Gottlieb ERJ-01844-2016_Gottlieb
Footnotes
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
- Received September 19, 2016.
- Accepted February 28, 2017.
- Copyright ©ERS 2017