



Elevation of surfactant protein A in plasma and sputum in cigarette smokers
- W. Mazur***,
- T. Toljamo#**,
- S. Ohlmeier¶,
- K. Vuopala+,
- P. Nieminen§,
- H. Kobayashif and
- V.L. Kinnula*⇓
- *Dept of Medicine, Pulmonary Division, University of Helsinki and Helsinki University Central Hospital, Helsinki
- #Depts of Pulmonary Medicine
- +Pathology, Lapland Central Hospital, Rovaniemi
- §Medical Informatics Group, University of Oulu
- ¶Proteomics Core Facility, Biocenter Oulu, Dept of Biochemistry, University of Oulu, Oulu, Finland
- fDept of Pulmonary Medicine, National Defense Medical College, Tokorozawa, Japan
- **These authors made a similar contribution to the study
- V.L. Kinnula, University of Helsinki and Helsinki University Central Hospital, Dept of Medicine, Pulmonary Division, PL 22 (Haartmaninkatu 4), 00014 Helsinki, Finland. E-mail: vuokko.kinnula{at}helsinki.fi
Abstract
Serum surfactant protein (SP)-A has been postulated to associate with pulmonary fibrosis, but its role in cigarette smoking-related lung diseases is undefined.
SP-A levels in plasma and induced sputum in nonsmokers, smokers with respiratory symptoms (cough and/or phlegm) and symptom-free smokers were assessed using a validated EIA method. A total of 474 current smokers without any diseases or medications were enrolled and followed for 2 yrs with 111 of them succeeding in stopping.
Plasma SP-A level was detectable in all subjects and elevated in smokers independently of the symptoms compared to nonsmokers (p = 0.001). After 2 yrs of follow-up, the SP-A level was higher in those who continued smoking compared to the quitters (p<0.001). Plasma SP-A levels were associated with age, smoking history and lung function. Sputum (n = 109) SP-A was nondetectable in most nonsmokers, whereas smoking and symptoms increased sputum SP-A highly significantly (p = 0.001).
In conclusion, SP-A may be involved in pathogenesis of cigarette smoking-related lung diseases. Further studies are needed to elucidate the role of SP-A in chronic obstructive pulmonary disease.
- Biomarker
- chronic obstructive pulmonary disease
- induced sputum
- screening
- smoking
- surfactant protein A
Pulmonary surfactant, a complex mixture of phospholipids and proteins, forms one of the major defence mechanisms against cigarette smoke. Serum surfactant protein (SP)-A has been extensively investigated, particularly in serum/plasma and bronchoalveolar lavage (BAL) samples in interstitial lung diseases, mostly in idiopathic pulmonary fibrosis [1–6]. However, there is inadequate, even inconsistent, evidence for the significance of circulating SP-A in cigarette smoke-related lung disorders [7–11] and it has not been generally evaluated in induced sputum. This can be considered as an almost noninvasive technique reflecting directly lung inflammation/pathology.
Four SPs, SP-A, SP-B, SP-C and SP-D, are intimately associated with surfactant lipids in the lungs. The hydrophilic SP-A is the major surfactant protein, constituting 3–4% of the total mass of isolated surfactant and 50% of the total SP [12]. In vitro studies and experimental models mostly using SP-A knockout mice have concluded that SP-A, which belongs to the collectin family of proteins, is protective against allergens, viral and bacterial infections and is involved in the maintenance of normal lung architecture [13–17]. SP-A is inducible by cytokines, lipopolysaccharide and drugs with anti-inflammatory properties, including corticosteroids, and possibly cigarette smoke, though there are some conflicting reports [18–22]. The abovementioned variability combined with different ethnic backgrounds and possible polymorphisms in the SP-A genes may explain some of the inconsistent findings. In human studies examining smokers and chronic obstructive pulmonary disease (COPD) sufferers, the patients often exhibit other comorbidities and experience a wide range of exposures, including smoking and medical treatments, which complicates the comparisons with earlier investigations.
Most studies on SP-A have been conducted in Japanese cohorts and with serum or plasma samples, and these results have not been confirmed in other populations. Induced sputum is virtually a noninvasive, safe and rather reproducible sampling technique, which is in widespread use in studies on chronic airway diseases [23–25], but there is very little data on SP-A levels in induced sputum. Our recent non-hypothesis driven proteomic studies on lung tissues revealed a remarkable elevation of SP-A in the lung tissues of COPD patients, even in the earlier stages of the disease [26]. Based on these observations together with the results from the large study of Kobayashi et al. [9], it was hypothesised that plasma and sputum (a sample that derives directly from the lung), SP-A may be considered as an early marker for lung stress reaction/minimal lung injury in smokers, even before any decline of lung function has occurred.
Due to the controversies in earlier studies, this study was intended to investigate SP-A in a cohort including a carefully selected population of “healthy cigarette smokers” with no confounding factors. The major goal was to investigate if current cigarette smoking can cause SP-A release into the circulating blood in non-Asian (Finnish) “healthy” smokers, and whether smoking cessation has any effects on the plasma levels of SP-A in a longitudinal setting. Further studies were conducted to determine whether SP-A could be detected in the sputum of “healthy” smokers and nonsmokers.
MATERIALS AND METHODS
Study subjects
The details of the project, the inclusion and exclusion criteria have been published elsewhere [27]. In brief, the exclusion criteria consisted of subjects with all lung or other diseases, regular medication, risk factors for other lung diseases (such as allergies, infections and exposures), any previous lung infection, such as diagnosed pneumonia or bronchiectasis, malignancy, or viral infection during the previous 2 months. There was special attention paid to excluding subjects with asthma, since in a detailed questionnaire some of the smokers and nonsmokers reported respiratory symptoms [27]. This study included smokers with at least a 10-yr history of cigarette smoking. At the first visit, a standardised personal history and blood sample were taken, the Fagerström test for nicotine dependence (FTND) [28] was conducted, and symptoms such as chronic cough and sputum production were assessed. Cumulative exposure to cigarette smoke was estimated in pack-years (1 pack-yr was defined as smoking 20 cigarettes a day for 1 yr). The subjects were counselled to quit smoking using the technique of motivational interviewing [29]. At the follow-up visit at 2 yrs, the same procedures and counselling were repeated. Each subject underwent flow–volume spirometry with a bronchodilatation test. Additionally, the same qualified nurse performed the sputum inductions. Given that SP-A has strong interactions with many micro-organisms [17] it is important to note that the sputum specimens included in this study showed no positivity to the major respiratory pathogens in quantitative culture. Finally, the data of 474 smokers (276 males and 198 females) with normal baseline spirometry according to Global Initiative for Obstructive Lung Disease (GOLD) criteria (ratio of forced expiratory volume in 1 s (FEV1) to forced vital capacity (FVC) ≥0.7 after bronchodilatation) [30] and Finnish national criteria for obstruction (FEV1/FVC >88% predicted and FEV1 >80% predicted) [31], and a negative bronchodilatation test (FEV1 and FVC <12% and <200 mL), were included. Nonsmoking control subjects (n = 34), were enrolled if they were >40 yrs of age, healthy and not taking any medications, and exhibited normal lung function according to the GOLD and the national criteria for obstruction (see above).
Collection of blood and induction of sputum samples
Peripheral whole venous blood was collected into EDTA tubes, plasma was prepared by centrifugation for 10–15 min at 1,500×g and stored at -80°C until analysed.
Sputum was induced from 91 smokers and 18 nonsmokers, as described by the European Respiratory Society task force, with 4.5% physiological saline solution [32, 33] and samples processed as previously described [34]. Briefly, expectorated samples were processed with dithioerythritol (Sigma, Munich, Germany). Suspensions were filtered through 70-μm nylon gauze and centrifuged at 400×g at 4°C for 10 min. For the differential cell count, the sample was smeared over glass slides, fixed and stained with Papanicolau stain. For the evaluation of the sputum specimens, at least 200 cells were counted by an experienced cytotechnologist (CT-IAC) and a pathologist blinded to the patient data. Detailed cell profiles were assessed for all sputum samples. Since SP-A is expressed in alveolar epithelium and bronchial epithelial cells of smokers [26], and in the tracheal epithelial cells [35], all samples, i.e. also those containing epithelial cells, were included in the analyses. The samples were immediately frozen at -80°C.
Measurement of SP-A in plasma and sputum supernatant samples
SP-A levels were assayed using a commercially available EIA kit (SP-A test; Sysmex, Kobe, Japan) [9, 36] for frozen serum and plasma. This test has undergone a thorough detailed evaluation and is approved as a clinically validated assay. The reference value for plasma is ≤43.8 ng·mL−1. Intra-assay coefficients of variation range from 4.5% to 6.15% and interassay coefficients of variation from 4.8% to 7.18% (Sysmex). Five concentration levels were used as standards for the analyses. No drifts of standard curves with time were seen. The method was adapted for the sputum supernatants without any major modifications.
Statistical analysis
Statistical significances of differences in continuous demographical characteristics, lung function variables and SP-A concentrations between the groups of smokers and nonsmokers were evaluated using one-way ANOVA or Kruskal–Wallis test. p-values of pairwise comparisons were adjusted with the Tukey method (ANOVA) or Benjamini–Hochberg procedure (pairwise Mann–Whitney tests after Kruskal–Wallis test). Repeated measures analysis of variance was used to examine the change in plasma SP-A and the interaction between visits and smoking status (smokers versus quitters). Pearson's correlation coefficient and scatter plots were used to evaluate the associations between plasma SP-A concentration and other continuous variables. Statistical analyses were done with SPSS for Windows version 18 software.
RESULTS
Subject characteristics
The characteristics of the subjects are shown in table 1. A total of 474 (93.1%) subjects were current smokers and 35 (6.9%) nonsmokers. In this group, 223 (43.8%) of the participants were female, and 198 (88.7%) were current female smokers. The total number of male smokers was 276 (96.5%). The mean±sd ages of the male and female smokers were 50.4±8.3 and 49.6±8.7 yrs, respectively; the mean ages of male and female nonsmokers were 55.5±8.8 and 52.5±10.4 yrs, respectively. Initially, all smokers considered themselves symptom-free, but after completing a detailed questionnaire, 155 (32.7%) smokers and four (11.4%) of the nonsmokers described the presence of respiratory symptoms such as cough and phlegm (cough or phlegm 39.0% and 52.7%). Based on the presence or absence of the respiratory symptoms, the smokers were divided into two subgroups: healthy (symptom-free, n = 319) and symptomatic smokers (n = 155). Both subpopulations were characterised and analysed separately and results for each compared to nonsmokers and against each other. Although all the participants displayed normal lung function in spirometry, the mean FEV1/FVC ratio and maximal expiratory flow at 50% FVC % predicted were significantly lower in all smokers compared to those of nonsmokers (table 1). In spite of the same cumulative exposure to smoking, symptomatic smokers were more nicotine-dependent than healthy smokers as indicated by the FTND (p<0.01). However, no difference was found between healthy smokers and symptomatic smokers groups with regards to all the demographic and lung function data.
Plasma SP-A is elevated in smokers and declines after smoking cessation
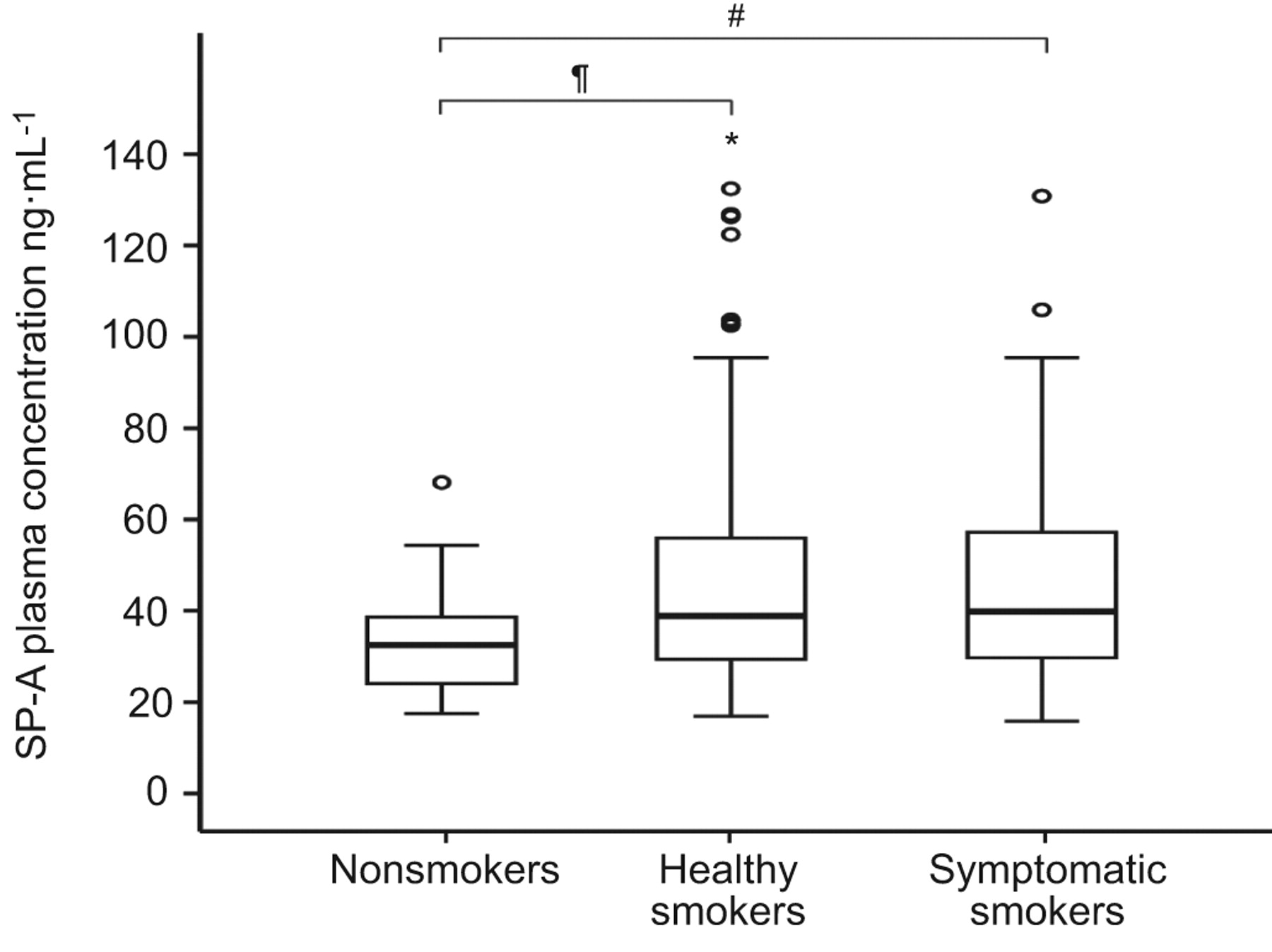
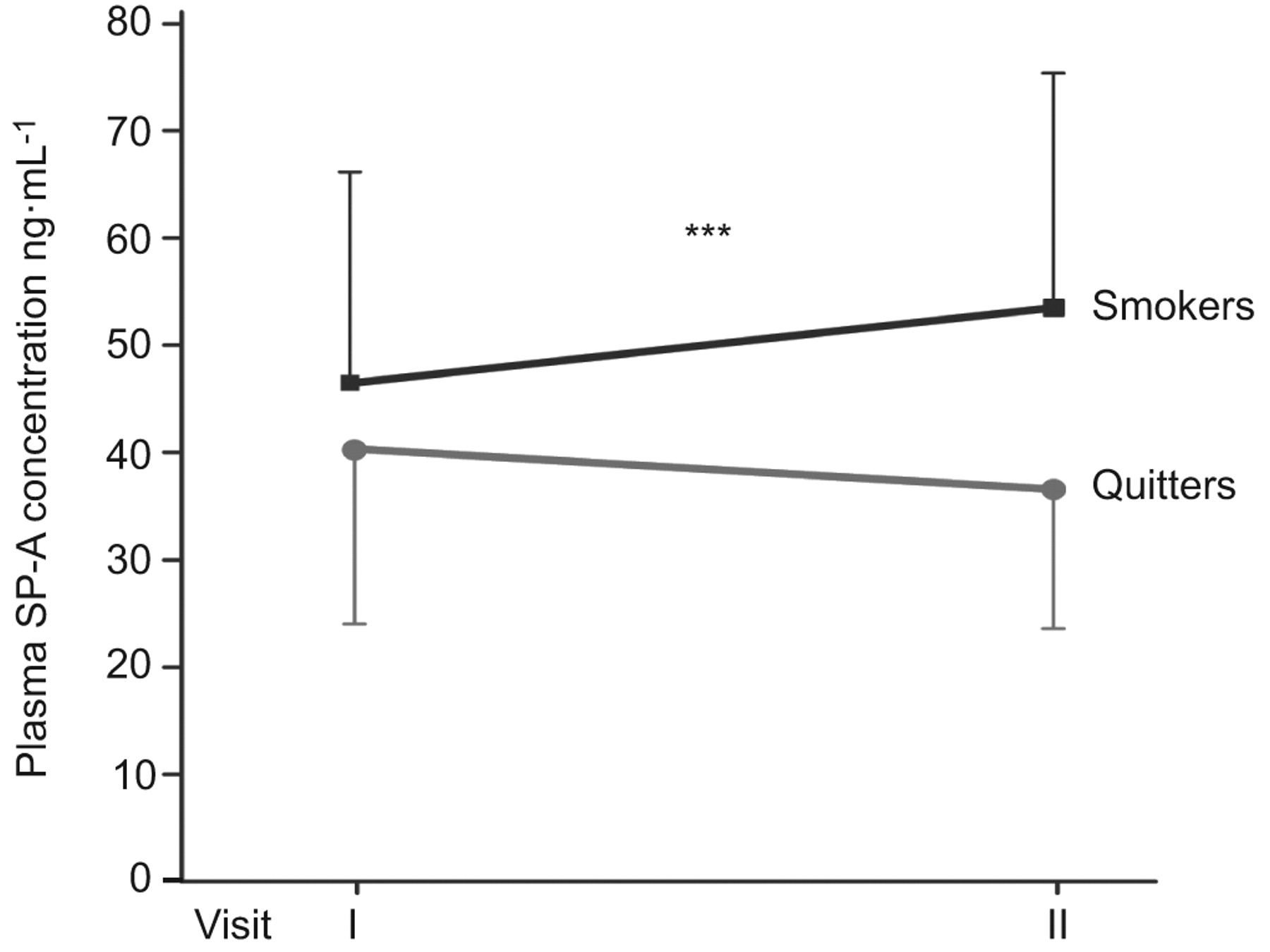
SP-A could be detected in all plasma samples. The mean concentrations of plasma SP-A (fig. 1) were higher in healthy and symptomatic smokers than in nonsmokers (mean±sd; 45.0±20.7, 45.4±20.3 and 32.5±12.3 ng·mL−1; p<0.001, respectively). There was no significant difference in plasma SP-A levels between healthy and symptomatic smokers, or males and females in nonsmokers or all smokers. The correlations between the plasma SP-A levels of all smokers and the baseline demographics, including age and body mass index, smoking history and lung functions are presented in figures 2 and 3. In the prospective follow-up of 2 yrs, 111 of the smokers successfully quitted smoking, which was confirmed by urine cotinine analyses. Their plasma SP-A levels tended to decline, though the difference was not statistically significant (mean±sd first visit 40.4±17.7 and second visit 38.3±15.9 ng·mL−1) compared to those who continued smoking (fig. 4). In the 324 smokers who continued smoking, there was an increasing trend to SP-A elevation. This different trend between the plasma SP-A levels of the smokers and the quitters was statistically significant (p-value of interaction between visits and smoking status being <0.001).

Comparison of plasma surfactant protein (SP)-A concentration in nonsmokers (n = 35), healthy (symptom-free) smokers (n = 319) and symptomatic smokers (n = 155) at baseline (visit 1). Data are expressed as medians with interquartile range (box) and overall range (whiskers). *: extreme value of a healthy smoker. #: p = 0.001; ¶: p = 0.002.

Relationship between plasma surfactant protein (SP)-A levels and demographic parameters and smoking history in all smokers (n = 446): a) age, b) body mass index (BMI), c) smoking history (pack-years) and d) Fagerström test for nicotine dependence (FTND).

Relationship between plasma surfactant protein (SP)-A levels and the lung function values a) post-bronchodilation forced expiratory volume in 1 s (FEV1) and b) FEV1/forced vital capacity (FVC) % predicted, in all smokers (n = 474).

The effect of smoking cessation on plasma surfactant protein (SP)-A levels during the 2 yrs of follow-up. Both SP-A measurements were available for 435 out of 474 smokers at visit I; at visit II 324 subjects had quit smoking while 111 were still smokers. Data are presented as mean±sd. ***: p<0.001 for interaction between visits and smoking status.
Sputum SP-A is highly elevated in symptomatic smokers compared to nonsmokers
Induced sputum was collected from 109 subjects, 18 nonsmokers and 91 smokers (table 2). A total of 31 (symptomatic smokers, 34%) of the smokers presented with symptoms such as cough or phlegm, or both. However, as it is difficult to obtain sputum from nonsmokers [23, 24], and we were successful in only a few of the cases, the number of nonsmokers remained low. Although no difference was found between the three groups with respect to demographics and physiological outcomes, symptomatic smokers again revealed more severe nicotine dependence compared to healthy smokers, as judged by higher FTND score (p = 0.03). The cell profile of the induced sputum samples (fig. 5) revealed significantly higher numbers of neutrophils in both groups of smokers than in nonsmokers (p = 0.04 for both). Nonsmokers exhibited a higher total number of lymphocytes and squamous epithelial cells (p = 0.02 and p = 0.03) than healthy and symptomatic smokers, respectively. There were no significant differences in cell counts between healthy and symptomatic smokers.

Cell differential counts of induced sputum specimens from 18 nonsmokers, 31 healthy (symptom-free) smokers and 60 symptomatic smokers. Both groups of smokers had significantly higher total number of neutrophils than nonsmokers. There were no significant differences in cell counts between healthy and symptomatic smokers. *: p<0.05.
Since there was a high variability in the sputum SP-A levels, the results were evaluated as medians (interquartile range). In those estimations (fig. 6), SP-A levels were significantly higher (p = 0.001) in symptomatic smokers (66.8 (10.4–365) ng·mL−1) compared to nonsmokers (4.9 (nondetectable to 18.5) ng·mL−1). The median sputum SP-A level in healthy smokers (16.4 (1.2–98.3) ng·mL−1) did not differ significantly from the level of nonsmokers, though there was an increasing trend (p = 0.06). The SP-A levels between healthy and symptomatic smokers did not differ significantly (p = 0.2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of sputum surfactant protein (SP)-A concentration in nonsmokers (n = 18), healthy (symptom-free) smokers (n = 60) and symptomatic smokers (n = 31). Data are expressed as medians with interquartile range (box) and range (whiskers). One extreme SP-A value of a symptomatic smoker (7,010 ng·mL−1) is not included in the figure. *: extreme values of healthy and symptomatic smokers. #: p = 0.001.
There was no correlation between the sputum SP-A levels and demographics, smoking history or lung function values (not shown). Furthermore, no correlation between the SP-A levels (high, 598–7,010 ng·mL−1 (n = 11) or low, <3.2 ng·mL−1 (n = 23)) and the sputum cell profile could be seen (i.e. for the “high levels” SP-A versus lymphocytes, neutrophils, macrophages and the total cell count, the Pearson correlations were as follows: r = 0.56, p = 0.09; r = -0.24, p = 0.50; r = -0.14, p = 0.69 and r = -0.03, p = 0.95, respectively).
DISCUSSION
This study on a large non-Asian population confirmed the elevation of plasma SP-A in current smokers, which is in agreement with the earlier corresponding study conducted in Japanese smokers [9]. This study also reveals that plasma levels of SP-A are higher in individuals who continue to smoke compared to those who give up smoking. The elevation of SP-A in plasma of smokers occurred irrespective of the presence of respiratory symptoms, such as cough and phlegm. This is the first study on plasma and sputum SP-A from the same subjects showing also that SP-A is highly elevated in the induced sputum of cigarette smokers compared to nonsmokers. Our findings support the hypothesis that cigarette smoking causes an exogenous stress reaction and possibly an early injury to the airways that is reflected by elevated levels of SP-A, both in plasma and sputum supernatants in cigarette smokers.
Previous studies have been inconsistent in reporting either elevated or lowered plasma or serum SP-A in smokers. Serum SP-A levels did not differ between nonsmokers and smokers in two European studies [11, 37]. In contrast, two studies conducted on Japanese subjects indicated that circulating SP-A levels were elevated in smokers [8, 10] and an additional large Japanese study concluded that the serum SP-A concentration is elevated in smokers, patients with COPD and also in some other lung disorders, such as pulmonary thromboembolism [9]. The variability in different studies may be partly due to genetic heterogeneity, ethnicity, environment, sex or age. The presence or absence of respiratory symptoms such as cough and phlegm does not seem to be a contributory factor as shown in the present study. Other reasons explaining the variability include different patient cohorts with variable comorbidities, possible infections and patients with drug therapies. In our study, all diseases have been excluded and none of the subjects were taking any regular medications.
SP-A, as a lectin, contributes to surfactant homeostasis and pulmonary immunity [13, 16, 38]. In normal conditions, SP-A is generally beneficial in protecting the lungs from oxidant, inflammatory and infectious stress [12]. However, the host defence functions of surfactant may be impaired in chronic smokers, and this may play a crucial role in the development of COPD [39]. Vlachaki et al. [40] have shown that the altered SP-A expression in COPD patients correlated with airway obstruction, and in the present study SP-A was found to associate both with smoking history and obstruction. Plasma/serum levels of SP-A have also been postulated to reflect increased permeability of the lung epithelium due to cigarette smoke [41–43], a result that is in full agreement with our observations.
A recent study in our laboratory found that SP-A is expressed not only in the alveolar epithelium in nonsmokers, but also in the bronchial epithelium in smokers and patients with COPD [26]. This difference in location between nonsmokers and smokers/COPD is important, since it can contribute to the SP-A levels in sputum specimens. Another recent study on male smokers and patients with COPD [40] yielded inconclusive complex results, but the study examined SP-A expression in total lung homogenate by Western blotting techniques. Homogenate contains all the constituents of the lung and thus may underestimate protein expression in one individual cell type. Another method used in that study was immunohistochemistry [40]. Those results contrast with our recent study, which used two-dimensional gel electrophoresis, mass spectrometry, Western blot and quantitative digital image analysis, in which highly elevated expression of SP-A was detected in the COPD lung [26]. Other studies which have evaluated SP-A in the BAL fluid have concluded that levels of SP-A are lower in smokers/COPD compared to nonsmokers [39, 44, 45]. The distal alveolar damage, however, in COPD may cause problems in the assessment of SP-A, and bronchofibreoscopy is difficult to perform in patients with COPD due to the collapse of the airways. One further problem in assessing SP-A from BAL fluid samples in general is its invasiveness, and therefore this technique cannot be used in early disease evaluation. As far as we are aware, in none of these studies has SP-A been measured from the same subjects, and at the same time in their BAL fluid and serum, and SP-A has not been evaluated from induced sputum specimens.
Sputum SP-A has not been previously studied in smokers, with the emphasis being placed on respiratory symptoms. In the present study, sputum SP-A levels were significantly higher in smokers than in nonsmokers, though there was a high variability. The absence or presence of respiratory symptoms in smokers had a significant effect on the sputum SP-A concentration, since in this group only the difference between nonsmokers and symptomatic smokers was statistically significant. There was, however, a trend for SP-A elevation in healthy smokers compared to nonsmokers (p = 0.06), while the difference between healthy and symptomatic smokers was far from significant (p = 0.2). Interestingly, also spontaneous sputum samples of smokers showed SP-A positivity (not shown). Generally sputum SP-A was not detectable or the levels were very low in nonsmokers. The reason for the variability remained unclear. The SP-A method has been tested and validated, and the samples were measured in duplicate. One explanation could be the nature of induced sputum: generally these secretions are derived mainly from the large, more proximal airways and this leads to some problems in the reproducibility of these samples [23, 24]. All sputum samples were included because SP-A is mainly expressed in epithelial cells, not only in the distal airways but also in trachea, sinus [46] and even middle ear epithelium [35, 47]. The exact quantification of SP-A in the sputum supernatant is also somewhat problematic since sputum is not homogenous and both the induction and isolation process may vary between laboratories. In spite of these problems, a highly elevated sputum SP-A level seems to represent a novel and promising early stress marker related to smoking, but further prospective studies will be necessary to elucidate the role of SP-A in COPD.
There are two SP-A isoforms, SP-A1 and SP-A2 [48]. It remains unclear whether these SP-A subtypes can explain a part of these observations. Our recent study [26] suggested that, in particular, SP-A2 is associated with smoking and COPD. Commercial antibodies, as well as the EIA analysis, detect both SP-A subtypes. Further studies are needed to assess the various roles of the SP-A subtypes and the effects of possible polymorphisms of SPA in smoking related lung diseases.
In conclusion, the levels of SP-A are elevated in the circulating blood in a large population of Finnish smokers and the SP-A concentration is highly significantly elevated in the induced sputum supernatants of smokers with respiratory symptoms. The prospective follow-up of these same subjects is now ongoing. The present and another Finnish cohort on patients with chronic airway diseases [49] will be monitored and analysed at regular intervals for SP-A.
Acknowledgments
T. Marjomaa (University of Helsinki and Helsinki University Central Hospital, Helsinki, Finland), M. Kaukonen (Dept of Pulmonary Medicine, Lapland Central Hospital, Rovaniemi, Finland) and P. Sortti (Dept of Pathology, Lapland Central Hospital) are acknowledged for their excellent technical assistance. This project was partly funded by the Research Program for the Intelligent Monitoring Health and Well-being, the Finnish Antituberculosis Association Foundation, a special governmental grant for health sciences research of Helsinki University Central Hospital (HUCH-EVO) and Lapland Central Hospital, Ida Montin Foundation, and Yrjö Jahnsson Foundation.
Footnotes
A press release for this article is available from www.erj.ersjournals.com/site/misc/presspack.xhtml
Statement of Interest
None declared.
- Received July 14, 2010.
- Accepted January 9, 2011.
- ©ERS 2011