



Nocturnal release of leukocyte-derived microparticles in males with obstructive sleep apnoea
- W. Trzepizur*#,
- P. Priou*#,
- A. Paris*,
- J. Nardi*,
- S. Tual-Chalot#,
- N. Meslier*#,
- T. Urban*,
- R. Andriantsitohaina#,
- M.C. Martinez# and
- F. Gagnadoux*#
- *Département de Pneumologie, Centre Hospitalier Universitaire
- #INSERM, U694, Université d'Angers, Faculté de Médecine, Angers, France
- F. Gagnadoux, Département de Pneumologie, CHU, 4 rue Larrey, 49933 Angers Cedex 9, France. E-mail: frgagnadoux{at}chu-angers.fr
To the Editors:
Multiple pathophysiological mechanisms have been proposed to contribute to the increased cardiovascular morbidity in obstructive sleep apnoea (OSA), including autonomic dysfunction, inflammation, oxidative stress and endothelial dysfunction 1. Microparticles (MPs) are small membrane vesicles that are shed from circulating cells or from the components of the vessel wall in response to activation and apoptosis. There is growing evidence in support of a potential role of MPs in the field of cardiovascular diseases. Increased levels of MPs derived from various cell types are found in patients at risk of cardiovascular diseases 2. By modulating inflammation, coagulation, vasomotor reactivity and angiogenesis, MPs might directly contribute to cardiovascular diseases 2. Recent case–control studies suggest a potential involvement of MPs in OSA-associated cardiovascular morbidity 3–6. An increase in morning levels of MPs derived from activated leukocytes has been demonstrated in otherwise healthy male OSA patients with marked nocturnal desaturations 5. In vitro, nitric oxide (NO) production by endothelial cells incubated with MPs from OSA patients correlates negatively with circulating levels of activated leukocyte-derived MPs 5. Ex vivo, mice previously injected with MPs from OSA patients display endothelial dysfunction, reduced endothelial NO release and increased adhesion molecule expression 5.
A decrease in endothelial function from evening to morning has previously been demonstrated in patients with OSA and found to correlate with the severity of sleep-disordered breathing 7. Since recent data suggest a potential role MPs in endothelial dysfunction 5, we aimed to study evening-to-morning change in activated leukocyte-derived MPs levels in otherwise healthy patients with OSA.
The study included 38 consecutive male patients (18–70 yrs of age) investigated by polysomnography (n = 25) or respiratory recording (n = 13) in the Sleep Unit of the Dept of Respiratory Medicine, Angers University (Angers, France) for suspected OSA. Exclusion criteria were previous treatment for OSA, body mass index (BMI) ≥35 kg·m−2, history of coronary artery disease, heart failure, stroke, hypertension, diabetes mellitus, dyslipidaemia and patients receiving any drug known to affect endothelial function. Patients with an apnoea–hypopnoea index (AHI) of ≥5 events·h−1 were included in the OSA group. Patients with an AHI <5 events·h−1 were included in the control group. The study was approved by the University of Angers ethics committee and patients gave their informed consent.
MP characterisation was performed as described previously 5 in the evening before the night recording, at approximately 18:00–19:00 h, before dinner, and after waking up in the morning following sleep recording, at approximately 07:00–08:00 h, before breakfast. Routine laboratory tests, including glucose, glycated haemoglobin, triglycerides, total cholesterol, high- and low-density lipoprotein cholesterol, and blood cell counts, were also performed on a morning blood sample. For MP isolation, evening and morning blood samples were drawn and collected in EDTA tubes (Vacutainers; Becton Dickinson, Le Pont de Claix, France) from a peripheral vein using a 21-gauge needle to minimise platelet activation, and were processed for assay within 2 h, as previously described 5. Samples were centrifuged for 20 min at 270×g, and plasma was then harvested and centrifuged for 20 min at 1,500×g to obtain platelet-free plasma (PFP). 200 μL PFP were frozen and stored at -80°C until use. MPs derived from activated l-selectin-positive leukocytes were identified by flow cytometry using anti-CD62L antibody. Irrelevant human immunoglobulin G was used as an isotype-matched negative control for each sample. To determine the MP concentration, 10 μL PFP were incubated with 5 μL specific antibody (Beckman Coulter, Villepinte, France). After 45 min incubation, samples were diluted in 300 μL 0.9% NaCl saline solution or annexin V labelling buffer. Equal volumes of sample and Flowcount beads were then added to calculate the MP concentration, and samples were analysed in a 500 MPL System flow cytometer (Beckman Coulter). Regions corresponding to MPs were identified in forward and side-angle light scatter intensity dot plot representations set at logarithmic gain, depending on their diameter (0.1–1 μm). Sample analysis was stopped after counting 10,000 events. MP analysis was performed without knowledge of the time the blood sample was taken (i.e. evening or morning) and whether it belonged to the OSA or the control group.
Mean±sem AHI was 1.9±0.4 events·h−1 in the control group (n = 15) and 16.2±2.4 events·h−1 in the OSA group (n = 23). There was no statistically significant difference between OSA and control patients for age, BMI, Epworth sleepiness scale, arterial blood pressure, lipid metabolism, glucose metabolism or percentage of smokers (see online supplementary material for detailed data).
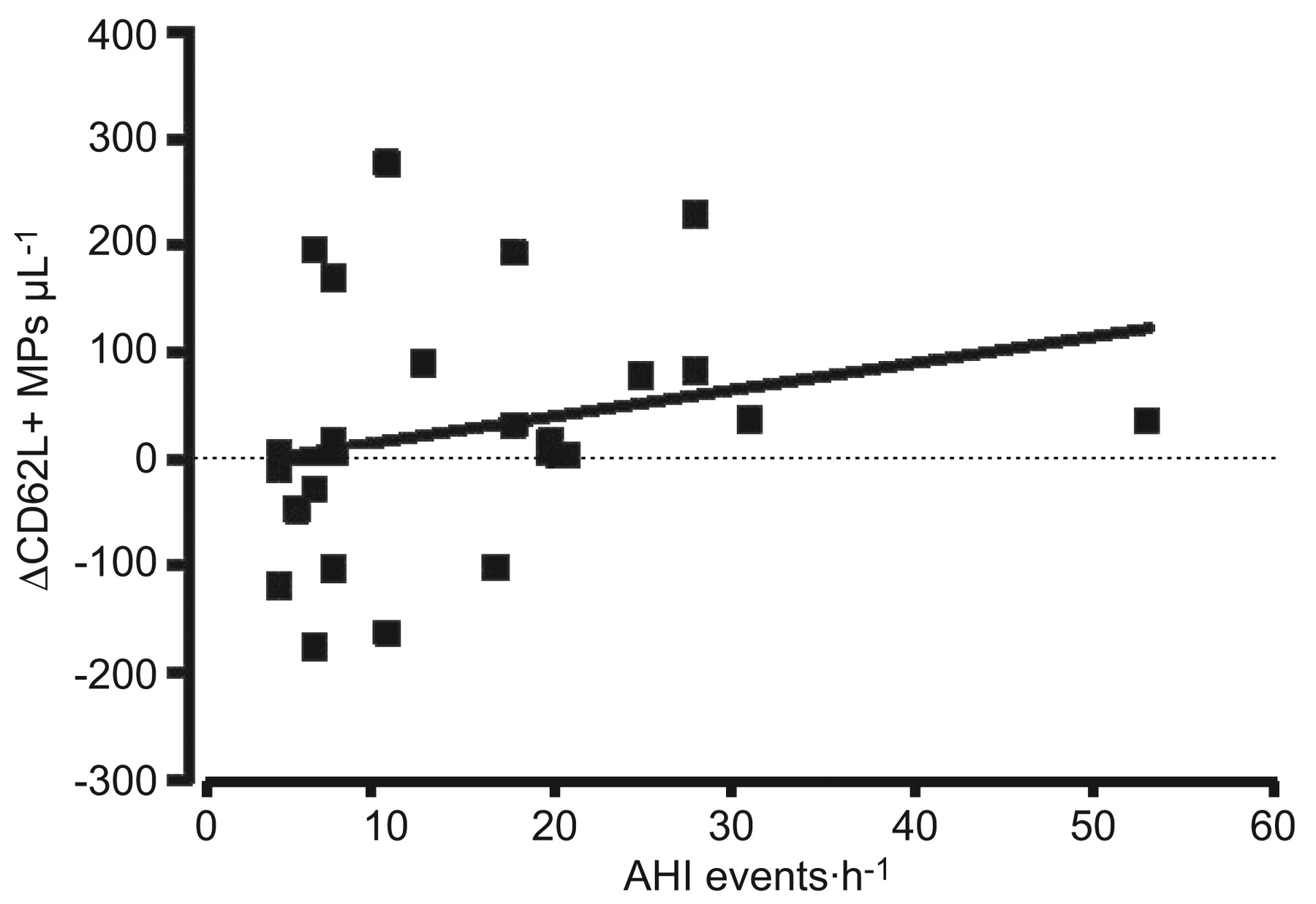
Figure 1 shows the comparison between evening and morning levels of CD62L+ MPs in the control group, the overall OSA group and patients with moderate-to-severe OSA (AHI ≥15 events·h−1; n = 10). A significant decrease in CD62L+ MPs from mean±sem 261.9±32.2 MPs per μL plasma in the evening to 196.8±36.9 MPs per μL plasma in the morning (p = 0.036) was observed in the control group. A trend toward an increase from 230.9±25.3 MPs per μL plasma in the evening to 259.8±28.5 MPs per μL plasma in the morning (nonsignificant) was observed in the OSA group. In patients with moderate-to-severe OSA, CD62L+ MPs increased significantly (p = 0.047) from evening (253.1±29.5 MPs per μL plasma) to morning (311.7±35.4 MPs per μL plasma). As shown in figure 2, a significant correlation was observed in the OSA group between AHI and the morning–evening difference in CD62L+ MPs (r = 0.45; p = 0.03). In the OSA group, the morning level of CD62L+ MPs was positively correlated with the AHI (r = 0.55; p = 0.006) and the 4% oxygen (r = 0.55; p = 0.006). No correlation was observed between morning CD62L+ MPs and any other clinical or laboratory parameters.

Comparison of mean±sem evening and morning plasma levels of activated leukocyte-derived microparticles (CD62L+ MPs) in controls (n = 15), all obstructive sleep apnoea (OSA) cases (n = 23) and those with moderate-to-severe OSA (n = 10). *: p<0.05 by Wilcoxon signed-rank test.

{kind=link}
{kind=link}
Scatter plot showing the relationship in the obstructive sleep apnoea group (n = 23) between apnoea–hypopnoea index (AHI) and the morning–evening difference in plasma levels of activated leukocyte-derived microparticles (δCD62L+ MPs). r = 0.45; p = 0.03.
Accumulation of leukocytes and their adhesion to the endothelium play a central role in the formation of atherosclerotic plaques. In asymptomatic subjects, circulating levels of leukocyte-derived MPs predict subclinical atherosclerosis burden 8. Leukocyte-derived MPs were demonstrated to be competent inflammatory mediators able to induce endothelial cell activation and IL-6 release 9. Systemic inflammation is considered as a key factor in the pathogenesis of cardiovascular complication in OSA 1. Previous studies have highlighted the roles of leukocytes in endothelial cell injury in OSA with decreased apoptosis and increased expression of l-selectin adhesion molecule 10. An increase in leukocyte-derived MPs has recently been described in OSA 3, 5. In accordance with these previous results, the present study underscores a positive correlation between morning CD62L+ MPs and the severity of sleep-disordered breathing. The finding that the evening-to-morning change in CD62L+ MPs correlates with the AHI in otherwise healthy patients provides evidence in support of a direct link between sleep-disordered breathing and leukocyte-derived MPs release. Evidence of the pathophysiological relevance of MPs in OSA was recently provided ex vivo by their ability to impair endothelium-dependent relaxation in response to acetylcholine and the endothelial response to flow when injected i.v. into mice 5. It can be hypothesised that nocturnal release of leukocyte-derived MPs could be involved in the early morning attenuation of endothelial function 7 and contribute to the increased rate of cardiovascular events during the first hours after waking from sleep.
However, randomised controlled trials including vascular reactivity assessment are still warranted to establish a causal link between circulating MPs and OSA, and the role of MPs, particularly leukocyte-derived MPs, in OSA-associated endothelial dysfunction.
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Statement of Interest
None declared.
- ©2011 ERS