



Reference ranges for interrupter resistance technique: the Asthma UK Initiative
- P.J.F.M. Merkus*#,
- J. Stocks¶,
- N. Beydon+,
- E. Lombardi§,
- M. Jonesf,
- S.A. Mckenzie**,
- J. Kivastik##,
- B.G.M. Arets¶¶ and
- S. Stanojevic¶++
- *Division of Respiratory Medicine, Dept of Paediatrics, Radboud University Medical Centre, Nijmegen Medical Centre, Nijmegen,
- #Erasmus University Medical Centre, Rotterdam
- ¶¶Dept of Paediatric Pulmonology, Wilhelmina Children's Hospital, University Medical Center Utrecht, Utrecht, The Netherlands
- ¶Portex Respiratory Unit, UCL Institute of Child Health,
- ++Medical Research Council, Centre of Epidemiology for Child Health, UCL Institute of Child Health,
- **Dept of Paediatric Respiratory Medicine, Royal London Hospital, London, UK
- +APHP Functional Unit of Paediatric Pulmonology, Robert Debré Hospital, Paris, France
- §Section of Respiratory Medicine, “Anna Meyer” University Hospital for Children, Firenze, Italy
- fDept of Paediatrics, Pontificia Universidade Católica do Rio Grande Sul, Hospital São Lucas, Porto Alegre, Brazil
- ##Dept of Physiology, University of Tartu, Tartu, Estonia
- S. Stanojevic, Portex Respiratory Unit, UCL Institute of Child Health, 20 Guilford Street, London, WC1N 1EH, UK E-mail: s.stanojevic{at}ich.ucl.ac.uk
Abstract
Measuring interrupter resistance (Rint) is an increasingly popular lung function technique and especially suitable for preschool children because it is simple, quick and requires only passive cooperation. A European Respiratory Society (ERS)/American Thoracic Society (ATS) Task Force recently published empirical recommendations related to procedures, limitations and interpretation of the technique. However, for valid interpretation, high-quality reference equations are required and these have been lacking. The aim of the present study was to collate Rint data from healthy children in order to produce more robust reference equations. A further aim was to examine the influence of methodological differences on predicted Rint values.
Rint data from healthy children were collected from published and unpublished sources. Reference equations for expiratory and inspiratory Rint were developed using the LMS (lambda, mu, sigma) method.
Data from 1,090 children (51% males) aged 3–13 yrs were collated to construct sex-specific reference equations for expiratory Rint and data from 629 children (51% males) were collated for inspiratory Rint. Height was the best independent predictor of both expiratory and inspiratory Rint. Differences between centres were clinically irrelevant, and differences between ethnic groups could not be examined.
The availability of a large and generalisable sample and the use of modern statistical techniques enabled the development of more appropriate reference equations for Rint in young children.
- Interrupter technique
- preschool children
- pulmonary function tests
- reference equations
The measurement of airway resistance using the interrupter resistance (Rint) technique has become an increasingly popular lung function test in paediatric respiratory medicine. Since equipment for its measurement is commercially available and requires only passive cooperation, Rint provides a suitable lung function test for young children. The technique is safe, quick, noninvasive, available, inexpensive, applicable in field studies, and delivers results that are clinically relevant 1–12, appear sufficiently valid 13 and which seem suitable for assessing bronchodilator responses 7, 9, 14–16. A European Respiratory Society (ERS)/American Thoracic Society (ATS) consensus statement was published in 2007, largely based on personal experience, in an attempt <~!?show=[to]?>to make the procedure more uniform and facilitate comparisons between centres 17. However, interpretation of Rint remains limited and without a suitable reference population with which to compare results.
Reference equations are essential to express pulmonary function in relation to that which would be expected for healthy children of similar age, sex, body size and ethnic group. The choice of reference equation directly affects the interpretation of paediatric pulmonary function data, and this can have a major impact on patient care and research 18, 19. So far, a clear recommendation regarding the best Rint reference equations has been lacking. Six published studies (reviewed in 20) describing reference equations for Rint may have important limitations, because they are based on relatively small numbers of subjects (with <100 children <5 yrs of age), and it is unclear to what extent these can be generalised to other populations.
It has previously been shown that it is feasible to collate existing reference data to produce generalisable reference equations for spirometry 21. The present study aimed to collate available Rint reference data to produce more robust reference equations in young children. In addition, we examined the influence of methodological differences on predicted Rint values.
METHODS
The Asthma UK Collaborative Initiative (www.growinglungs.org.uk) was established to collate lung function data from healthy young children for spirometry, specific airway resistance and the interrupter technique. The present study focussed on expiratory Rint (Rint,exp) and inspiratory Rint (Rint,insp). Initially, the collaborative group was comprised of members of the ATS/ERS Task Force for paediatric pulmonary function testing. Subsequently, collaborators with access to pulmonary function data in healthy preschool children were identified by: systematically searching PubMed; advertising at international respiratory conferences; membership bulletins; word of mouth; and a manual search of relevant respiratory periodicals. Rint data were collected in healthy children aged 3–13 yrs, together with details regarding recruitment, population characteristics, equipment, measurement protocols and quality control. Collaborating centres were visited by one of the authors in order to conduct inter-lab comparisons, compare protocols and discuss methodological differences. All data were anonymised prior to contribution and came from research studies in which full local ethics approval and parental consent had been obtained.
Statistical methods for defining the reference range
The centile charts were constructed as described previously 21–23 using the LMS (lambda, mu, sigma) method 24. This method is an extension of regression analysis, which includes three components: 1) the skewness (lambda), which models the departure of the variables from normality using a Box–Cox transformation; 2) the median (mu); and 3) the coefficient of variation (sigma), which models the spread of values around the median and adjusts for any non-uniform dispersion, hence LMS. The three quantities (LMS) are allowed to change with height and/or age, to reflect changes in the distribution as children grow. We applied the LMS method using the GAMLSS (Generalised Additive Models of Location, Shape and Scale) package in the statistical program R (version 2.6.1, R Foundation; available from www.r-project.org) 25.
During preliminary modelling, sex was independently associated with Rint and significant interactions were observed between sex and height; therefore, sex-specific models were created. According to previous reports, differences between Rint,insp and Rint,exp preclude combination of these data 3, 11, thereby necessitating separate reference equations. Fractional polynomials were used to fit each of the curves and explain the body size-related changes 26. The goodness of fit was assessed using the Schwarz Bayesian Criterion, which compares consecutive models directly whilst adjusting for the increased complexity to determine the simplest model with best fit.
Prediction models
The fitted models provide sex-specific and height-adjusted values for the median, coefficient of variation and skewness. The median (M) is the predicted value for the individual which, together with the coefficient of variation (S) and skewness (L), allows the individual’s Rint measurement to be converted to a z-score: z-scores are normally distributed with mean 0 and sd 1. Alternatively, the % predicted can simply be calculated from the median value, but this method of expressing the data is not recommended as it does not consider the between-subject variability of the measurements 17.
z-scores are normally distributed with mean 0 and sd 1. Alternatively, the % predicted can simply be calculated from the median value, but this method of expressing the data is not recommended as it does not consider the between-subject variability of the measurements 17.
RESULTS
Eight centres with reference Rint data in healthy subjects were identified. Seven of these used the classical interruption technique with similar methodologies and produced similar results. The remaining study used a different measurement technique (the opening technique) 17 and procedure was noted as a clear outlier; this study was subsequently excluded. Data collection in one centre was still ongoing at the time of final data collation for the current initiative; it therefore could not be included. Results from five of the six centres who contributed Rint data have been published previously 3, 27–30. In order to keep centres anonymous, a unique identifier was assigned to each centre and used thereafter. Data from healthy subjects (mean age 6.3 (range 2–13)) yrs, corresponding to a height range of 85–174 cm, with a similar proportion of males and females, were collated. One centre measured Rint in three ethnic groups but found no difference between the groups 29. An additional centre measured Rint in a mixed-ethnic population but could not define ethnicity due to the highly diverse population characteristics 27. All six centres contributed Rint,exp measurements (n = 1,090), with three centres also measuring Rint,insp (n = 629). In all centres, measurements were performed by the child breathing through a mouthpiece with a nose-clip in situ. A brief summary of the six studies is presented in table 1.
Population characteristics
All subjects included in the collated reference population were born at term and were free of chronic respiratory diseases, but the studies differed with respect to other exclusion criteria, such as history of wheeze (table 1). The majority of subjects had height-for-age, weight-for-age (where recorded) and body mass index-for-age z-scores between ±2 sd 31.
Methodological differences
Three of the six centres were visited by one of the authors (P.J.F.M. Merkus). Methodologically, the three centres were similar. The remaining three centres completed a detailed questionnaire about the equipment and protocols.
Rint,expversus Rint,insp
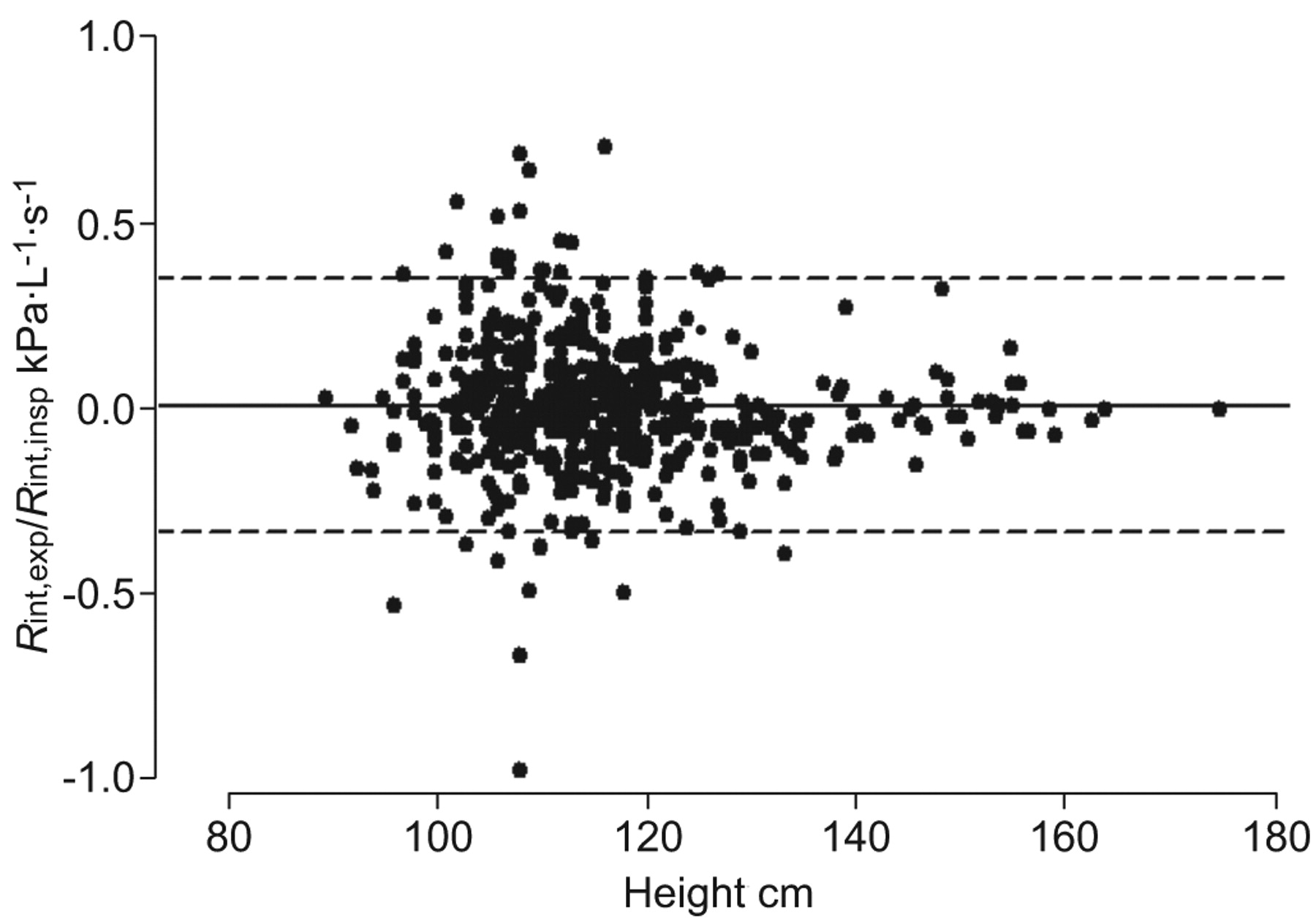
In a subset of 535 subjects with both measurements, a comparison of Rint,insp with Rint,exp found no difference between the two (mean difference -0.001 (95% CI -0.016–0.013, 95% limit of agreement -0.341–0.339) kPa·L−1·s−1). There was no relationship between the observed difference and age, height or weight; however, both the within-subject variability and absolute difference between these two outcomes tended to be slightly greater in younger children (i.e. those <110 cm) (fig. 1).

Bland–Altman plot of the difference between expiratory interrupter resistance (Rint,exp) and inspiratory interrupter resistance (Rint,insp) against height, demonstrating greater variability between measurements at younger ages.
Trace exclusion
All contributors described a procedure to exclude incorrect measurements according to the child's behaviour, including: irregular breathing, vocal cord adduction and leakage around the mouthpiece. Five centres used additional criteria such as tachypnoea and extreme neck flexion/extension. All centres inspected individual mouth pressure–time recordings and discarded those deemed to be technically unacceptable. The criteria for such exclusions were not always clearly described, with most investigators using an “eyeballing technique” to approve or discard pressure tracings 32.
Cheek support
All but one of the centres (F) supported the child's cheeks during Rint data collection. Centre F undertook a within-subject comparison with and without cheek support in 29 children for Rint,insp and 39 children for Rint,exp and did not find a significant difference between the two techniques. The 95% limits of agreement between the measurements with and without cheeks supported were -0.104–0.080 kPa·L−1·s−1 for Rint,insp and -0.094–0.126 kPa·L−1·s−1 for Rint,exp 28.
Filter use
Two centres (C and E) used the same bacterial filter. In both centres, the software took the filter resistance into account prior to reporting results.
Interruption trigger
Interruptions were triggered at peak tidal flow, in all but one of the centres (D), where interruptions occurred between 40–60% of tidal volume.
Method of Rint calculation
Mouth pressure was calculated using the two-points linear back extrapolation to 0 ms (centres A, B, C and E) or 15 ms (centres A, D and F) after the onset of interruption (table 1).
Number of tracings
The minimum number of technically acceptable tracings required per child (five to seven tracings) was similar in all centres. Data from children with fewer than five acceptable traces were excluded.
Mean or median
Four centres reported mean results, whereas two only reported the median. In the two centres in which Rint,exp was reported both as mean and median (C and F, total 390 subjects), no difference was observed (mean 0.00 (95% CI -0.005–0.006, 95% limit of agreement -0.1–0.1) kPa·L−1·s−1). As these were interchangeable, data from centres that reported median results were combined with the other four centres.
Reference equations
The sex-specific reference equations for Rint,exp and Rint,insp are presented in table 2; Rint,exp equations with 95% prediction limits are illustrated in figure 2. There were significant sex differences during preliminary modelling, with males having slightly lower Rint,exp values; therefore, sex-specific equations were constructed. Using univariable analysis, height and age were both predictors of Rint,exp; using multivariable analysis, only height was independently associated with Rint,exp. Height was the only significant and independent predictor of Rint,insp. After adjustment for height, weight was not associated with either outcome and was not included in the final models. To avoid edge effects due to limited sample size at the extremes of the height range, we recommend that these equations are not extrapolated to children who are <90 cm or >160 cm in height.

Sex-specific reference equations for expiratory interrupter resistance (Rint,exp; —) and 95% prediction limits (- - -) for a) males and b) females.
The variability of measurements around the prediction equation was constant around the mean, and there was evidence of left skewness for both outcomes. Both of these observations have implications for defining the 97.5th percentile, the ULN. The estimates of the between-subject variability (S) and skewness (L) are presented in table 2; these, along with the median predicted value (M), can be combined algebraically to calculate a z-score. For example, the Rint,exp z-score and ULN for a male can be calculated using the following equation:
z-score = ((Observed Rint,exp)/(0.1337+7631.3*Height−2)0.4213− 1)/(0.24*0.4213)
ULN = (0.1337+(7631.3*Height−2))*(1.96*0.24*0.4213+1)1/0.4213Rint,exp is expressed as kPa·L-1·s-1 and height is expressed as cm.
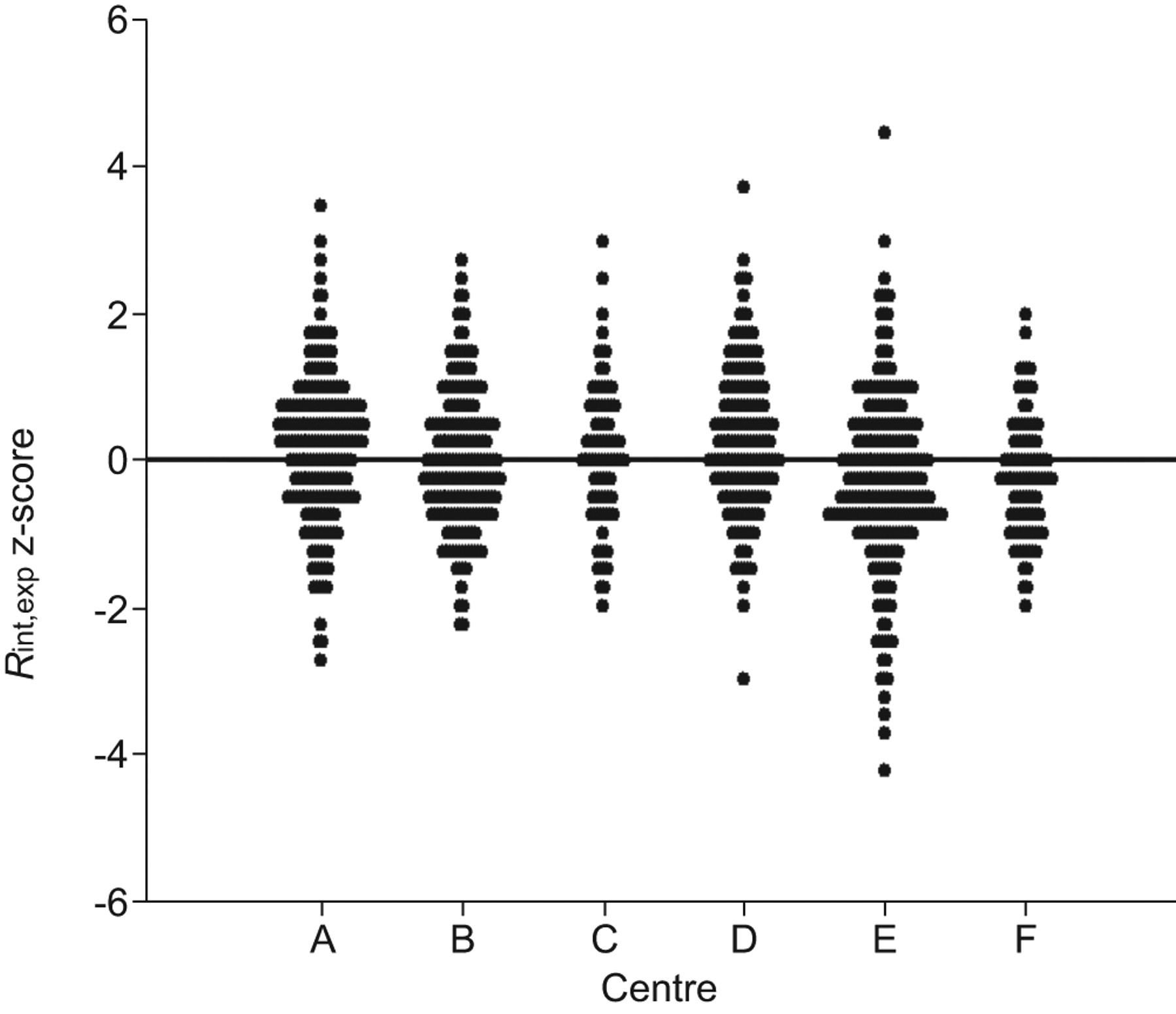
Between-centre differences
There was remarkable agreement between the centres and while on average some centres had z-scores that were above zero, and others where it was below zero, the magnitude of the offset was small (maximum 0.3 z-scores) and unlikely to affect clinical interpretation of results (fig. 3). The percentages of healthy children above the ULN in each centre were: A 2.5%; B 4.5%; C 3.3%; D 4.1%; E 4.7%; and F 0.1%.
{kind=link}
{kind=link}
{kind=link}
Centre-specific z-scores for expiratory interrupter resistance (Rint,exp) demonstrated good agreement between the six centres, despite some offset. Mean (95% CI) z-scores in each centre: A 0.15 (0.02–0.27); B -0.03 (-0.15–0.09); C -0.27 (-0.41− -0.11); D 0.05 (-0.15–0.24); E 0.25 (0.11–0.39); F -0.29 (-0.42− -0.16).
DISCUSSION
The present study provides paediatric reference equations for Rint,exp (n = 1,090) and Rint,insp (n = 629) measurements from healthy children of 90–160 cm. The equations may facilitate more accurate interpretation of Rint results. By combining normative data from published and unpublished studies, the collated dataset describes a generalisable population, making the reference applicable across a variety of populations. In addition, the larger sample size allowed investigation of the distributional characteristics of the data, and exploration of various demographic variables. The use of the LMS method allowed for a more accurate definition of the ULN, which may improve the technique’s discrimination between health and disease. Further work is needed to validate the ULN in different disease groups, particularly those for which Rint is most useful clinically.
These equations are appropriate when: 1) the classic interrupter technique is performed using commercially available equipment; 2) children are seated, wearing nose-clips and using a mouthpiece; 3) children have their cheeks supported; and 4) children are ≥90 cm and ≤160 cm tall.
For the first time, separate equations are presented for males and females. The larger sample allowed detection of statistically significant differences between the sexes; however, the observed differences were small (table 3) and unlikely to affect clinical interpretation of results. While we would expect to observe age-dependent sex differences, reflecting the differential development of the airways between females and males during growth 33, we found that females had higher resistance at all ages. While this was unexpected, it may reflect the fact that Rint probably measures central airway function, whereas the enhanced airway function reported in females prior to puberty is most noticeable in indices that reflect more peripheral airway calibre, such as forced expired flows 21, 34.
We present reference equations for both Rint,exp and Rint,insp as previous studies have shown that these two outcomes are not interchangeable 3, 11. In a subset of 535 children, with both outcomes we found minimal differences between these two. The increased within-subject variability between Rint,insp and Rint,exp in younger children could either reflect higher airway compliance during tidal breathing and/or slightly less consistent measurement technique in this age group, as observed for spirometry 21.
The retrospective nature of the data collection meant there were differences in population characteristics (exclusion criteria) between the six centres. For instance, whereas all centres excluded preterm children, not all excluded children with a history of wheeze or passive smoke exposure. The collated population therefore lies somewhere between a reference and an ideal population, and reflects a typical testing population, which may be more generalisable across different populations. The dataset was also limited in that we could not investigate ethnic differences. It is likely that the current study, as well as available literature, is underpowered to detect such differences. A recently published study describing reference equations for a Chinese population noted reference values similar to other published studies in Caucasian children >110 cm; however, the differences observed in shorter children may reflect the limited number of subjects <110 cm 35.
The retrospective nature of the study also limited our ability to separate methodological differences from population differences. While methodologically the centres were similar with respect to equipment used and measurement techniques, subtle methodological differences may explain some of the observed differences in the measured values. In a subset of subjects, we were able to demonstrate that results summarised as mean were interchangeable with results presented as the median. A similar conclusion was reached when direct within-subject comparisons were investigated in a group of 40 healthy children 36. Slightly lower predicted values and somewhat larger between-subject variability were found in centre F (fig. 2), where cheeks were not supported during the measurements. However, we consider it unlikely that cheek support played a relevant role in this study as all the children were healthy and had no signs of airway obstruction. As suggested in the recent ERS/ATS guidelines 17, we recommend that in future studies cheeks should be supported during measurement as this decreases variability and increases accuracy of measurement in children with airway obstruction. Most centres used eyeballing to determine quality of the measurement 32. Although one could argue that eyeballing as a quality control measure is somewhat subjective, a previous study found clinical interpretation of the measurement was not affected, and that fewer curves were rejected compared to using objective quality criteria 32.
It is important to note that the entire collated dataset of the present study was based on cross-sectional measurements, which may not be appropriate for interpreting longitudinal changes. Nonetheless, these reference equations should be valid for interpreting cross-sectional data, as long as measurements are similar to those used in the current study. If equipment or measurement techniques change, or other ethnic groups are investigated, these reference equations will need to be updated.
Conclusions
These collated reference equations provide a step towards improved interpretation of Rint measurements in young children. We recommend that manufacturers of Rint equipment incorporate these reference equations into their software, so that those using the same techniques, and conducting measurements in similar populations according to the same international guidelines 17, can optimise interpretation of results. These equations should also facilitate more meaningful comparisons between centres. This may create new opportunities for future multicentre studies in young children with respiratory disease, in which Rint is the selected outcome.
Footnotes
Earn CME accreditation by answering questions about this article. You will find these at the back of the printed copy of this issue or online at www.erj.ersjournals.com/misc/cmeinfo.dtl
Support Statement
This study was funded by Asthma UK. J. Kivastik was funded by the Estonian Science Foundation (grant no. 7322).
Statement of Interest
A statement of interest for S.A. McKenzie can be found at www.erj.ersjournals.com/misc/statements.dtl
- Received August 5, 2009.
- Accepted November 27, 2009.
- ©ERS 2010