



Oxidative stress in resuscitation and in ventilation of newborns
- 1Institute of Medical Paediatrics, Neonatal Intensive Care Unit, University of Messina, Messina, Italy. 2Dept of Cellular and Structural Biology, The University of Texas Health Science, Center at San Antonio, San Antonio, TX, USA.
- R. J. Reiter, Dept of Cellular and Structural Biology, University of Texas Health Science Center at San Antonio, Mail Code 7762, 7703 Floyd Curl Drive, San Antonio, TX 78229-3900, USA. E-mail: reiter{at}uthscsa.edu
Abstract
The lungs of newborns are especially prone to oxidative damage induced by both reactive oxygen and reactive nitrogen species. Yet, these infants are often 1) exposed to high oxygen concentrations, 2) have infections or inflammation, 3) have reduced antioxidant defense, and 4) have high free iron levels which enhance toxic radical generation. Oxidative stress has been postulated to be implicated in several newborn conditions with the phrase “oxygen radical diseases of neonatology” having been coined. There is, however, reason to believe that oxidative stress is increased more when resuscitation is performed with pure oxygen compared with ambient air and that the most effective ventilatory strategy is the avoidance of mechanical ventilation with the use of nasopharyngeal continuous positive airway pressure whenever possible. Multiple ventilation strategies have been attempted to reduce injury and improve outcomes in newborn infants. In this review, the authors summarise the scientific evidence concerning oxidative stress as it relates to resuscitation in the delivery room and to the various modalities of ventilation.
- Bronchopulmonary dysplasia
- modality of ventilation
- newborn
- oxidative stress
- respiratory distress syndrome
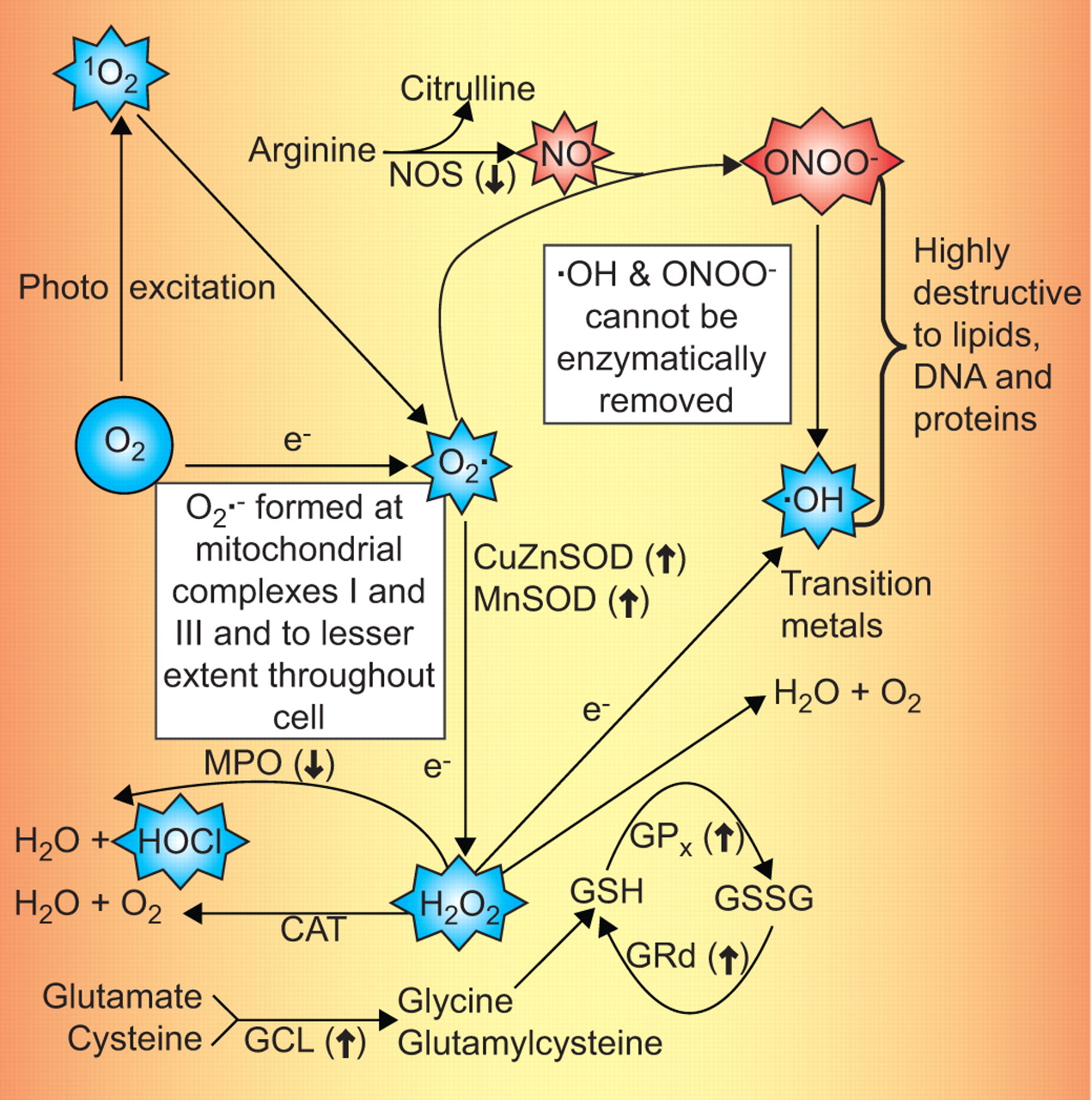
Free radicals are highly reactive molecules containing one or more unpaired electrons. They donate or abstract electrons from other molecules in an attempt to pair their electrons and generate a more stable species. Oxygen-derived reactants collectively termed reactive oxygen species (ROS) as well as reactive nitrogen species (RNS) are normally produced in living organisms. When produced in excess, they are important mediators of cell and tissue injury 1–3. The resulting damage is referred to as oxidative stress. Free radicals are highly unstable and several enzymes and small-molecular-weight molecules with antioxidant capabilities protect against them 4; these protective molecules are part of the anti-oxidative defence system. There is a critical balance between free radical generation and antioxidant defences. Free radical reactions lead to the oxidation of lipids, proteins, polysaccharides and to DNA damage (fragmentation, base modifications and strand breaks); as a consequence, radicals have a wide range of biologically toxic effects 5, 6. The generation of both ROS and RNS are summarised in figure 1⇓.

{kind=link}
Summary of the production of reactive oxygen species (ROS, namely, the superoxide anion radical (O2·-), hydrogen peroxide (H2O2), hydroxyl radical (·OH), singlet oxygen (1O2) and hypochlorous acid (HOCl)) and reactive nitrogen species (RNS, namely, nitric oxide (NO) and the peroxynitrite anion (ONOO-)). The most reactive of these products and, therefore, the most damaging are the ·OH and ONOO-. Since they are not enzymatically removed from the cell, the antioxidative defense system can only prevent the damage they do by scavenging them. These reactants are especially abundantly produced in mitochondria where molecular oxygen (O2) is reduced to O2·- by electrons that escape from the respiratory chain, especially at mitochondrial complexes I and III. There are a number of antioxidative enzymes that convert reactive species to less reactive products. For example, O2·- is dismutated to H2O2 by the cytosolic and mitochondrial superoxide dismutases (CuZnSOD and MnSOD, respectively). Also, H2O2 is converted to innocuous products by glutathione peroxidase (GPx) which results in the oxidation of glutathione (GSH) to form glutathione disulfide (GSSG); this latter molecule is recycled back to GSH by glutathione reductase (GRd). Intracellular GSH levels are maintained by the rate-limiting enzyme in GSH synthesis, glutamylcysteine ligase (GCL). Catalase (CAT), another antioxidative enzyme, also removes H2O2 from cells. In the presence of myloperoxidase (MPO) in leukocytes, H2O2 is converted to HOCl and H2O. The conversion of H2O2 to the highly toxic ·OH in the presence of a transition metal, usually Fe2+, is referred to as the Fenton reaction. The arrows in parenthesis after the enzymes indicate that melatonin (a recently discovered antioxidant) either stimulates (↑) or inhibits (↓) their activity. Melatonin has been shown to reduce the toxicity of ROS/RNS in human newborns. Additionally, melatonin scavenges the most toxic reactants, namely, the ·OH and ONOO- which cannot be enzymatically removed. Nitric oxide synthase (NOS) is often considered a pro-oxidative enzyme and is inhibited by melatonin.
Newborns and especially pre-term infants are probably more prone to oxidative stress than are children and young adults. There are some special reasons for this. These infants very often 1) are exposed to high oxygen concentrations, 2) have infections or inflammation, 3) have reduced antioxidant defence, and 4) have free iron which enhances the Fenton reaction leading to production of highly toxic hydroxyl radicals 7, 8. The Fenton reaction describes the interaction of hydrogen peroxide with a transition metal resulting in the generation of the highly toxic hydroxyl radical. Oxidative stress has been postulated to be implicated in several newborn conditions and, in 1988, Saugstad 9 coined the phrase “oxygen radical diseases of neonatology”. The idea contends that oxidative stress affects different organs, often simultaneously, giving rise to different signs according to the organ most affected. He included bronchopulmonary dysplasia/chronic lung disease, retinopathy of prematurity and necrotising enterocolitis in this category. Later, it became clear that free radicals are also involved in periventricular leukomalacia 10 as well as in regulating the ductus arteriosus and pulmonary circulation 11–13. If the concept of “oxygen radical diseases in neonatology” is correct, it means that the conditions mentioned are not different diseases but belong to the same entity yielding different symptoms according to which organs are mostly affected. In comparison with healthy adults, lower levels of plasma antioxidants including vitamin E, β-carotene, melatonin and sulfhydryl groups, lower concentrations of plasma metal binding proteins such as ceruloplasmin and transferrin, and reduced activity of erythrocyte superoxide dismutase are typical of newborn infants. Furthermore, infants frequently have higher plasma levels of non-transferrin-bound iron and higher erythrocyte free iron than adults 14.
OXIDATIVE STRESS AT PARTURITION
The transition from fetal to neonatal life at birth involves acute and complex physiological changes. During delivery, the fetus is transferred from an intrauterine hypoxic environment with an oxygen tension (PO2) of 20–25 mmHg to an extrauterine normoxic environment with a PO2 of 100 mmHg. This four- to five-fold increase is believed to induce an elevated production of ROS and RNS 15. In addition, labour and childbirth may induce periods of both hypoxia and oxidative stress for the newborn, while the neonatal plasma has relatively low concentrations of components with antioxidative function to resist oxidative damage.
The relationship between the oxidative state of the mother and the newborn at the moment of birth has been investigated. Argüelles et al. 16 measured oxidative stress markers (carbonyl groups, lipid peroxides and total antioxidant capacity (TAC)) and found a good correlation between the oxidative state of the normal mother and the neonate, with a high level of maternal oxidative stress corresponding to an even higher oxidative stress in newborn umbilical cord blood. They also reported that mothers who smoke and their newborns had higher concentrations of protein carbonyl, lipid peroxides and a depressed TAC 16.
Term labour is associated with oxidative stress for the neonate. Many authors have demonstrated that there is the same degree of fetal oxidative stress in vaginal delivery as that resulting from Caesarean section 17, 18. It is unclear whether oxidative stress is related to delivery itself or whether it reflects a pre-existing fetal level of oxidative status. Laurie et al. 19 demonstrated that distressed fetuses delivered by emergency Caesarean section exhibited increased malondialdehyde (MDA) concentrations, an indicator of lipid oxidative damage, and enhanced glutathione peroxidase (GPX), an antioxidant enzyme, in amniotic fluid and umbilical cord blood compared with nondistressed fetuses delivered by elective Caesarean section. These findings are suggestive of elevated fetal oxidative stress 19.
RESUSCITATION WITH AMBIENT AIR VERSUS PURE OXYGEN
The traditional method of resuscitation of newly born infants is with pure oxygen 20, 21. However, this therapy was introduced without any preceding randomised trials being conducted. It was assumed, without any supporting data, that 100% O2 would be the optimal oxygen concentration 22. There is, however, reason to believe that oxidative stress is elevated when resuscitation is performed with pure oxygen compared with ambient air. For this reason, Saugstad and Aasen 23 warned that the use of high concentrations of supplemental O2 might be detrimental for resuscitation. Several experimental as well as clinical studies seem to confirm this 24–30. In addition to animal studies, clinical trials have importantly shown that ambient air is at least as efficient as pure O2 for resuscitation of the newly born 31–35. In 1993, Ramji et al. 31 published a single-centre study from New Dehli with the aim of investigating the feasibility of using 21% O2 for resuscitation. A total of 42 infants resuscitated with 21% and 42 with 100% O2 were enrolled with the following inclusion criteria: cardiac frequency <80 bpm and or apnoea/poor response. Birthweight <1,000 g and or lethal congenital anomalies were exclusion criteria. Restoration of cardiac frequency, Apgar score, acid base and blood gases were not different between the two groups. A second investigation in this area was the Resair 2 study 32, a multicentre study comprising ∼600 infants from Egypt, Estonia, India, Norway, Philippines and Spain recruited from 10 centres. The study was pseudo-randomised and not blinded. No significant differences in the primary outcome measure, which was early neonatal death and/or hypoxic ischaemic encephalopathy grade 2 or 3, were found. However, there was a statistically insignificant tendency to higher neonatal survival in the infants resuscitated with 21% versus 100% O2. Time to first breath and first cry was significantly delayed in those re-oxygenated with pure oxygen.
Since then, three more studies by Resair 2 collaborators have been published, two from Spain 33, 34 and one from India 35. When the results of these five studies were combined, a significant reduction in neonatal mortality (from 13 to 8%) in those resuscitated with ambient air compared with 100% O2 was found. Most of the 1,737 children were enrolled from developing countries; Saugstad et al. 36, therefore, separately analysed the Spanish babies. In this material, a 3% reduced mortality was found in favour of room-air infants (from 3.5 to 0.5%), indicating that, also in industrialised countries, a significant reduction in neonatal mortality can be achieved by not using pure oxygen for resuscitation. One surprising finding of these studies is that time to first breath and first cry is significantly reduced by 24 s; moreover, the 5-min Apgar score, as well as cardiac frequency at 90 bpm is also significantly higher in room-air-resuscitated infants compared with those resuscitated with pure oxygen.
For babies born at term, the Guidelines recommend use of 100% supplemental O2 when a baby is cyanotic or when positive pressure ventilation (PPV) is required during neonatal resuscitation. However, research suggests that resuscitation with <100% may be just as successful. If resuscitation is started with <100% oxygen, supplemental oxygen up to 100% should be administered if there is no appreciable improvement within 90 s following birth. If supplemental oxygen is unavailable, the use of room air to deliver PPV is suggested. To reduce excessive tissue oxygenation in a very pre-term baby (less than ∼32 weeks), use of an oxygen blender and pulse oximeter during resuscitation is recommended; in this case, begin PPV with an oxygen concentration between room air and 100%. No studies justify starting at any particular concentration. Adjust O2 concentration up or down to achieve an oxyhaemoglobin concentration that gradually increases toward 90%, and reduce the oxygen concentration as saturations rise over 95%. If the cardiac frequency does not respond by increasing rapidly to >100 bpm, correct any ventilation problem and use 100% oxygen. If the facility does not have use of an oxygen blender and pulse oximeter in the delivery room, and there is insufficient time to transfer the mother to another facility, the resources and oxygen management described for a term baby are appropriate. There is no convincing evidence that a brief period of 100% oxygen during resuscitation is detrimental to the pre-term infant.
In 2007, a summary of the results of three systematic reviews 36–38 of five trials and seven individual studies, including up to 2,011 newborn infants, indicated that neonatal mortality was reduced by 30–40% if resuscitation is carried out with 21% instead of 100% O2 39. Room-air resuscitation also leads to faster early recovery and a shorter duration of resuscitation. To date, there are sufficient data available to recommend that newborn resuscitation should generally not be carried out using 100% O2. In extremely low-birth-weight (ELBW) infants, arterial oxygen saturation (Sa,O2) levels should be kept between 85 and 93% or possibly between 88 and 95%, but should definitely not exceed 95%. Fluctuations should be avoided 39.
A recent prospective, randomised, clinical trial included infants of ≤28 weeks of gestation who required active resuscitation and were randomly assigned to a low-oxygen group (fraction of inspired oxygen: 30%) or a high-oxygen group (fraction of inspired oxygen: 90%) 40. The fraction of inspired oxygen in the low-oxygen group was increased stepwise to 45% and that in the high-oxygen group was reduced to 45% to reach a stable pulse oxygen saturation of approximately 85% at 5–7 mins in both groups. No differences in oxygen saturation in minute-to-minute registers were found, independent of the initial fraction of inspired oxygen used 4 mins after cord clamping. Likewise, no differences in mortality rates in the early neonatal period were detected. The authors concluded that resuscitation can be safely initiated for ELBW neonates with a low fraction of inspired oxygen (∼30%), which then should be adjusted to the infant's needs, reducing the oxygen load to the neonate 41.
OXIDATIVE INJURY: AMBIENT AIR VERSUS PURE OXYGEN
In reference to the degree of oxidative stress and later injury, Vento et al. 28 showed that resuscitation with 100% O2 triggers long-term elevation of oxidative damage in the newborn since elevated oxidative stress was found at least 28 days after birth in those given oxygen but not in those provided room air. It is known that oxidative stress influences cell death and cell growth and, therefore, might influence long-term outcome 37. This could explain why there is an association between delivery room oxygen exposure and later childhood lymphatic leukaemia; the elevated DNA damage associated with elevated O2 exposure may increase the likelihood of leukaemia 42 since oxygen derivatives are capable of damaging DNA, often a prelude to cancer.
Tan et al. 37 showed that a reduction in mortality is seen in infants resuscitated with room air, and no evidence of harm has been demonstrated. However, the small number of identified studies and their methodological limitations dictate caution in interpreting and applying these results. Therefore, on the basis of currently available evidence, if one chooses room air as the initial gas for resuscitation, supplementary oxygen should continue to be made available.
MORTALITY: AMBIENT AIR VERSUS PURE OXYGEN
Bajaj et al. 43 showed that resuscitation of a newborn baby with room air instead of the current practice of 100% O2 does not confer benefits in terms of reduced hypoxic–ischaemic encephalopathy (HIE) and/or mortality. Significantly, there is no increase in adverse outcome with the use of room air, which can be recommended for resuscitation if oxygen is not available.
A meta-analysis by Raby et al. 38 supports the hypothesis that room air is superior to 100% O2 as the initial choice for resuscitating clinically depressed newborns as it may result in a lower mortality rate; however, adequately powered studies of long-term neurodevelopmental outcomes are not yet available. The Summary of Major Changes to the 2005, as defined by the AAP/AHA Emergency Cardiovascular Care Guidelines for Neonatal Resuscitation 44 related to the use of oxygen during neonatal resuscitation, affirms that the current evidence is insufficient to resolve all questions regarding supplemental oxygen use during neonatal resuscitation.
RESPIRATORY DISTRESS SYNDROME AND OXIDATIVE STRESS
When born too early, infants are delivered with a very immature stage of lung development: the late canalicular stage for infants born at 24–26 weeks (i.e. for ELBW infants), and early or mild saccular stage for those born after 26 but before 32 weeks of gestation (in part ELBW and all very low birth weight (VLBW) infants) 45. Pre-term birth occurring during the late canalicular or early saccular stage is very likely to lead to severe respiratory distress syndrome (RDS). The poorly developed peripheral airways and immaturity of cells important for lung maturation are the major causes of poor surfactant production by type II cells and inadequate antioxidant responses to increased ambient oxygen. For example, the superoxide dismutase (SOD) activity appears in the developing lungs concomitantly with the surfactant synthesis by type II pneumocytes 46.
Hyperoxic exposure itself, although essential for survival of RDS infants, probably induces excessive production of ROS/RNS in the respiratory system. There exist, however, several potential causes of intra- and extracellular oxidant stress in the pre-term newborns with RDS. The high inspiratory concentrations of oxygen required to achieve adequate arterial oxygenation, pro-oxidant drugs and infections or extrapulmonary inflammation can all promote ROS accumulation and the utilisation and depletion of antioxidative factors 46.
In experimental models of respiratory distress it has been observed that the specific targets of a hyperoxic insult to the lung are the vascular endothelial cells and the epithelial cells of the alveoli. ROS/RNS induce ultrastructural changes in the cytoplasm of pulmonary capillary endothelial cells and cause focal hypertrophy and altered metabolic activity. Thus, increased oxidative stress accompanied by reduced endogenous antioxidant defenses may play a role in the pathogenesis of a number of inflammatory pulmonary diseases including respiratory distress in the newborn 47, 48. A deficit in the precise balance between exposure to oxidants and endogenous antioxidants results obviously leads to elevated oxidative damage. The molecular damage caused by oxidative stress appears to be involved in the pathogenesis of a growing number of diseases, including RDS of the newborn 49, 50.
When phagocytes such as neutrophils are stimulated by micro-organisms or other means, they become activated and increase their oxidative metabolism; as a result, toxic oxygen and nitrogen derivatives, i.e. ROS/RNS, are formed (fig. 1⇑). If these toxic products are not inactivated, their high chemical reactivity leads to damage to a variety of cellular macromolecules including proteins, carbohydrates, lipids and nucleic acid. This results in cell injury and may induce respiratory cell death 51. Under these conditions, a surfactant deficiency may be aggravated by inactivation of the small amount of endogenous surfactant that is produced 52. Furthermore, if exogenous surfactant is given this may also be destroyed 48, 50.
ROS/RNS also have been implicated in the molecular damage seen in the bronchoalveolar lavage (BAL) fluid of patients with RDS 53, 54. This assertion is supported by several findings: hydrogen peroxide (H2O2) is detected in the expired air of RDS patients, and myeloperoxidase and oxidised-1-antitrypsin have been found in BAL fluid. Moreover, increased plasma lipid peroxidation has been recorded in critically ill patients and in patients with sepsis and at risk of developing RDS. Also, evidence of augmented levels of oxidised lipids and proteins have been found in the plasma of patients with RDS. Increased levels of ROS have also been implicated in the molecular damage seen in the BAL fluid of patients with RDS. BAL fluid normally contains a large amount of the antioxidant glutathione; but in patients with RDS this is mostly in the oxidised form 55.
Consistent with this, oxidative inactivation of 1-antiprotease also has been observed in RDS. Elevated concentrations of xanthine and hypoxanthine are present in the plasma and BAL fluid of patients with RDS and are a potential source of ROS in the presence of exogenously added xanthine oxidase. Also, elevated concentrations of orthotyrosine and metatyrosine in BAL fluid protein imply the formation of the damaging OH· in the lungs of these patients, since orthotyrosine and metatyrosine are isomers of tyrosine thought to be formed exclusively by aromatic hydroxylation of phenylalanine by OH· 56. Chlorotyrosine and nitrotyrosine also have been found in BAL fluid from patients with RDS. Increased concentrations of chlorotyrosine residues in BAL fluid proteins from patients with RDS indicate hypochlorous acid (HClO) production by activated inflammatory cells in the lungs of these patients. Chlorotyrosine is formed by HClO-dependent chlorination of paratyrosine. HClO is a damaging oxidant formed from H2O2 and chloride ions by the enzyme myeloperoxidase (fig. 1⇑), present in activated inflammatory cells. HClO has been implicated as the major damaging species produced by activated neutrophils. HClO itself is a destructive oxidant but it also may interact with low molecular mass iron or superoxide anion radicals to produce the OH·.
Nitrotyrosine concentrations also are significantly elevated in the BAL fluid protein of patients with RDS 57. Nitration of tyrosine residues is an in vivo marker of the formation of peroxynitrite (ONOO-). ONOO- is a nitrogen-based reactant formed when nitric oxide (NO) couples with O2·- (fig. 1⇑). Earlier studies report increased nitrotyrosine concentrations in the lungs of patients with RDS. ONOO- is capable of damaging lipids, proteins and DNA. Additionally, under acidic conditions, it can decompose to form a powerful oxidant with properties similar to OH·. There is, however, another possible explanation for the formation of nitrotyrosine. Recent work shows that nitrotyrosine can arise from the reaction of tyrosine with nitroxyl chloride, an intermediate formed by the interaction of nitrite (the auto-oxidation product of nitric oxide) with HClO. Interestingly, nitrotyrosine concentrations in BAL fluid protein from patients with RDS treated with NO were elevated compared with those found in lung-injured patients not receiving this therapy 58.
Increased nitrotyrosine concentrations may reflect augmented ONOO- formation in the patients receiving NO. Since the patients receiving inhaled NO are no sicker, in terms of Acute Physiology and Chronic Health Evaluation II score or inspiratory oxygen fraction (FI,O2) requirements, than those patients not receiving this therapy, it implies that inhaled NO may react with O2·- in these circumstances to form the nitrating agent 59. Finally, myeloperoxidase concentrations are significantly elevated in the BAL fluid from patients with RDS, indicating lung neutrophil recruitment and activation 60. Collectively, the data are compelling that RDS is associated with elevated ROS/RNS generation and the consequential increased oxidative damage to the respiratory tree.
OXIDATIVE STRESS AND CHRONIC LUNG DISEASE
Chronic lung disease (CLD) of the newborn is one of the definitive factors influencing the mortality and morbidity of VLBW infants 53. The aetiology of CLD is unknown, but many investigators have suggested that free radicals may have a key role in its development. The exposure of immature lungs to prolonged periods of high levels of inspired oxygen is accepted as an important contributor to the development of CLD through both free radical effects on endothelial and epithelial cell barriers that induce pulmonary oedema and trigger mechanisms that lead to activation and accumulation of inflammatory cells 61. Unfortunately, CLD still develops in extremely premature infants that do not have significant ventilatory or supplemental oxygen needs in the acute course of prematurity. A new form of CLD is less fibrotic than its earlier counterpart, and there is a significant component of delayed alveolar development and perhaps permanent alveolar underdevelopment 62, 63.
Currently, the mechanisms for the development of the new form of CLD have not been fully elucidated and the contribution of oxygen toxicity is debatable. The fact that premature infants develop CLD without being exposed to high concentrations of supplemental oxygen raises the question as to whether oxidative stress in fact contributes to the development of CLD. It is plausible, however, that even low concentrations of supplemental oxygen in premature patients with developmentally poorly prepared antioxidant defense mechanisms may generate significant oxidant stresses and lung injury secondary to oxidation of specific macromolecules 64. In addition, inflammatory cell accumulation and activation in the lung may generate oxidants and oxidant stresses that also oxidise macromolecules which leads to CLD 64. The literature provides evidence that premature infants who develop CLD have both qualitative and quantitative differences in oxidation of lipids and proteins when compared with infants who do not develop CLD. Such differences in oxidation patterns are the most obvious in the first few days of life 65.
In a study by Ogihara et al. 66, plasma levels of lipid aldehydes were measured in the first week of life in premature infants. Plasma concentrations of heptanal, 2-nonenal and 4 hydroxynonenal were higher in the first 24 h of life in infants who develop CLD than in those that did not. In another study, elevated exhaled pentane levels were strongly associated with several adverse outcomes in premature infants. In fact, infants who developed CLD had higher exhaled pentane on the first day of life than did patients who did not develop CLD 67. Protein oxidation was also previously assessed in premature infants and correlated with the development of CLD. There is also an association between higher protein carbonyl contents in tracheal aspirates in the first week of life and the development of CLD 68. Moreover, Ramsay et al. 69 demonstrated that there were no differences in oxygen requirements of tracheal aspirate contents of total 2,4-dinitrophenylhydrazine reactive proteins between premature infants who did or did not develop CLD; however, infants who developed CLD did have more frequent oxidation of specific proteins than did infants who did not develop CLD. These results suggest that identifying specific proteins that are more frequently oxidised in infants who develop CLD may be important in determining specific mechanisms for the development of CLD.
Other pathways of ROS generation include metabolism of catecholamines, the arachidonic acid cascade, and mitochondrial metabolism 70. However, the main source of free radicals in the lungs seems to be phagocyte activation 71, 72. The increase in phagocyte number and interleukin concentrations in BAL fluid obtained from premature infants with CLD indicates that oxygen toxicity and inflammation are involved in the development of lung injury 73.
Infants destined to develop CLD have increased pro-inflammatory cytokine levels in airway samples 74, 75; however, there is little information on when the pro-inflammatory indicators appear or how they progress in the pre-term lung subjected to mechanical ventilation. Moreover, in those infants, a large number of activated neutrophils are found in the air spaces within hours after birth 76.
The contribution of airway inflammation to the development of CLD of prematurity has been extensively studied 77–81. There is a dynamic and complex balance between pro- and anti-inflammatory cytokines in the human immune system. Previous studies on premature infants have shown that an increase of tumour necrosis factor (TNF)-α in tracheal secretions, among other pro-inflammatory cytokines, was associated with the duration of mechanical ventilation 82 and the development of CLD 83–85. The role of the anti-inflammatory cytokines is less clear. Recent studies have demonstrated that pre-term infants with respiratory distress do produce significant amounts of IL-10 in the lower airways and the presence of this anti-inflammatory cytokine prevents the development of CLD of prematurity 86. Jones et al. 87 were unable to detect interleukin (IL)-10 in most of the airway samples from pre-term infants. This observation agrees with a study showing that the control of airway inflammation by this cytokine is limited in infants 88.
Of interest is that Saugstad 89 claims that these changes are seen very early and are present only a few hours or days after birth in those infants who go on to develop CLD. This may support the suggestion that pre-natal factors, such as inflammation, are important for its development and that the changes leading to CLD are triggered before birth. If this is the case, it holds important implications for future therapeutic approaches 89.
OXIDATIVE STRESS AND MODALITY OF VENTILATION
The most common reason for neonates requiring respiratory support is RDS. In this disease, the pathophysiology is one of progressive loss of lung volume, intrapulmonary shunt and deflation instability. Animal and human models of RDS have clearly shown that ventilator strategies alter the clinical and pathological evolution of RDS. In addition, it is claimed that neonates with RDS are susceptible to lung injury and the subsequent development of related conditions. It is being increasingly realised that modes of mechanical ventilation that result in end-inspiratory alveolar over-stretching and/or repeated alveolar collapse and re-expansion disturb the normal fluid balance across the alveolo-capillary membrane. The effects of this include disturbance in the integrity of the endothelium and epithelium and impairment of the surfactant system; these changes are similar to those seen in acute RDS. Mechanical ventilation can injure pre-term lungs and multiple ventilation strategies have been attempted to reduce injury and improve outcomes.
In 1999, Clark et al. 90 proclaimed that, “the concept of ventilator-induced lung injury has come of age”. There are many data which suggest that ventilation can cause biotrauma associated with a “mediator storm” (perhaps cytokines) and that it is responsible for distal organ dysfunction, subsequent multiorgan failure and death. Although it has been shown that pulmonary cytokine levels also appear to be elevated in some neonates on assisted ventilation, the exact relationship to neonatal lung injury has yet to be defined. Pro-inflammatory mediators may be elevated because of fetal exposure to maternal inflammatory mediators, post-natal infections or due to release of mediators from the pre-term lung attributable to ventilator-induced injury.
The pre-term lung is susceptible to injury with the initiation of ventilation because potential lung volumes are small, surfactant may be deficient, the lung matrix is not fully developed and the air spaces contain residual fetal lung fluid. Tidal volume (VT) during the resuscitation of pre-term infants is not monitored, and easily visible chest movements will result in VT in excess of that routinely needed to ventilate infants 91. Pre-term infants are often hyperventilated and low carbon dioxide tension (PCO2) values after birth correlate with an increased incidence of CLD 92. The most effective strategy is the avoidance of mechanical ventilation with the use of nasopharyngeal continuous positive airway pressure whenever possible. Barotrauma, volutrauma and oxygen toxicity, during intermittent positive pressure ventilation, are assumed to be important factors in the pathogenesis of CLD as they cause pulmonary damage, resulting in a release of multiple pro-inflammatory cytokines and production of extracellular matrix components and growth factors 93.
MECHANICAL VENTILATION AND LUNG INJURY
The current orientation in the clinical practice is to emphasise the potential importance of reducing mechanical insults on acutely diseased lungs by using special modes of ventilation, e.g. high frequency oscillatory ventilation (HFOV), that limit the pressure and volume of gas delivered to the lungs 94. HFOV may reduce volutrauma by using a small tidal volume (VT), maintaining almost constant alveolar pressure, and optimising lung volume through the regulation of mean airway pressure 95, 96. Reducing volutrauma is important since damaged tissue generates free radicals and may become inflamed, a process that further contributes to the production of toxic oxygen derivatives.
The results of randomised trials to date, conducted on human neonates comparing HFOV with conventional mechanical ventilation (CMV), have been inconclusive and the results are conflicting. Therefore, it remains an open question whether HFOV is more beneficial in preventing CLD than a high-rate, minimal-pressure, low VT, CMV strategy 97. Also, in the Cochrane Database of 2007, the authors conclude that there is no clear evidence that elective HFOV offers important advantages over CMV when used as the initial ventilation strategy to treat pre-term infants with acute pulmonary dysfunction. There may be a small reduction in the rate of CLD with HFOV use, but the evidence is weakened by the inconsistency of this effect across trials and the overall borderline significance 98.
To develop less traumatic mechanical ventilation, with the aim of limiting lung volutrauma, guaranteed volume (GV) integrates various modalities to trigger ventilation with pressure control including assisted/controlled (A/C), synchronised intermittent mandatory ventilation (SIMV) and pressure-support ventilation (PSV). GV is an uncommon ventilation method which controls pressure but provides a fixed current volume according to compliance variations, to resistance and to spontaneous activity. The ventilator corrects inspiratory pressure giving a current volume that tends to be the same as the set volume. The gradual improvement in compliance of a pulmonary pathology ventilated with GV follows a reduction of peak inspiratory pressure 99, 100.
Lista et al. 101 evaluated the lung inflammatory response in pre-term infants with RDS mechanically ventilated with or without GV, by measuring pro-inflammatory cytokines (IL-6, IL-8, and TNF-α) in tracheobronchial aspirate (TA) fluid. Their data suggest that a volume-targeted ventilatory strategy may play a role in reducing the acute inflammatory response, and thereby also limiting oxidative stress in pre-term infants with RDS. The outcome of this clinical trial shows that there are lower pro-inflammatory cytokine levels (IL-6, IL-8, and TNF-a) in BAL of infants with severe RDS supported with PSV with GV compared with PSV only. The study of Dani et al. 102 was the first clinical trial demonstrating that the early treatment of RDS with HFOV is associated with the reduction of pulmonary inflammatory reaction in pre-term infants in comparison with the early application of another potentially lung-protective ventilations strategy such as PSV plus GV.
While there are obviously conflicting findings in this field, it is generally accepted that antecedent lung inflammation or injury makes the lungs more susceptible to volutrauma and oxidant-induced injury by the reactive species shown in figure 1⇑. The resulting damage promotes inflammation that is not limited to the lung but that may also affect distant organs, and oxygen, when used at high concentration, can be toxic.
Although there are a variety of modalities of ventilation that are noninvasive, each ventilatory strategy has a potentially negative consequence in terms of tissue damage resulting from the production of both ROS and RNS. Small VT ventilation is associated with progressive low volume and surfactant dysfunction. Limiting VT requires higher levels of end-expiratory pressure and/or FI,O2 to maintain adequate oxygenation. Higher levels of FI,O2 can contribute to oxidant-induced lung injury. Thus, the use of lung protective strategies in the neonate requires proactive decisions that must be specific for disease pathophysiology and lung maturity, and that involve compromises between gas exchange goals and potential toxicities of the treatments.
Besides the ventilatory strategies in common use to treat brochopulmonary dysfunction in newborns and because optimal oxygen saturation for use in these cases is difficult to achieve, other treatments have also been attempted. For example, inhalation of nitric oxide, administration of caffeine or surfactant and intramuscular injection of high doses of vitamin A have been used in infants with the hope of improving pulmonary physiology. Additionally, the utility of two antioxidants, i.e. N-acetylcysteine and superoxide dismutase, have been tested. None of these extra-ventilatory procedures has generally provided substantial benefit 103.
CONCLUDING REMARKS
Toxic derivatives of oxygen are referred to as free radicals and are either oxygen (ROS) or nitrogen-based (RNS) reactants. ROS/RNS are destructive to all key molecules, i.e. lipids, proteins and DNA, within all cells. Since the lungs of newborn infants are highly susceptible to oxidative damage by ROS/RNS, care should be taken in the use of pure oxygen during resuscitation of infants. Also, avoidance of mechanical ventilation with the use of nasopharyngeal continuous positive air pressure may reduce respiratory tissue damage resulting from ROS/RNS.
Oxygen, which is obviously vital to survival, can obviously be highly damaging to tissues such as the lungs of newborns which are known to be poorly equipped to neutralise its toxic derivatives. Thus, the exposure of the newly born infant respiratory tree to oxygen at a higher percentage than exists in normal ambient air, i.e. 20%, or at a positive pressure should be performed with caution especially since it may be minimally or no better than using ambient air.
Also, the use of antioxidants to quell molecular damage by ROS/RNS could be considered in situations in which pure oxygen or positive pressure are used. One antioxidant that may be useful in these situations is melatonin (fig. 1⇑); this indoleamine has been shown to be useful to combat oxygen toxic in newborns 104.
Statement of interest
None declared.
- Received February 25, 2009.
- Accepted June 12, 2009.
- © ERS Journals Ltd