



Nitric oxide production by the alveolar compartment of the lungs in cirrhotic patients
- B. Degano 1 ,
- M. Mittaine 2 ,
- P. Hervé 1 , 3 ,
- J. Rami 2 ,
- N. Kamar 4 ,
- B. Suc 4 ,
- D. Rivière 2 and
- L. Rostaing 4
- 1Service de Pneumologie et Réanimation Respiratoire, Centre National de Référence de l'Hypertension Artérielle Pulmonaire, Hôpital Antoine Béclère, Clamart, 2Service d'Exploration Fonctionnelle Respiratoire, CHU Larrey, 4Dept de Néphrologie, Dialyse et Transplantation d'Organes, CHU Rangueil, Toulouse, and 3Centre Chirurgical Marie-Lannelongue, Le Plessis-Robinson, France.
- B. Degano, Service de Pneumologie, Hôpital Antoine Béclère, 157 rue de la Porte de Trivaux, 92141 Clamart, France. E-mail: degano.b{at}gmail.com
Abstract
In cirrhotic patients, alveolar nitric oxide (NO) concentration is increased. This may be secondary to increased output of NO produced by the alveoli (V′A,NO) and/or to decreased lung transfer factor of NO. In advanced liver cirrhosis, NO produced by the alveoli may play a role in abnormalities of pulmonary haemodynamics and gas exchanges. In cirrhotic patients, we aimed to measure V′A,NO and to compare V′A,NO with pulmonary haemodynamics and gas exchange parameters.
Measurements were performed in 22 healthy controls and in 29 cirrhotic patients, of whom eight had hepatopulmonary syndrome. Exhaled NO concentrations were measured at multiple expiratory flow rates to derive alveolar NO concentration. V′A,NO was the product of alveolar NO concentration by single breath lung transfer factor for NO.
V′A,NO was increased in patients (median (range) 260 (177–341) nL·min−1) compared with controls (79 (60–90), p<0.0001). Alveolar–arterial oxygen tension difference failed to correlate with V′A,NO. However, cardiac index correlated positively and systemic vascular resistance correlated negatively with V′A,NO (r = 0.56, p = 0.001 and r = -0.52, p = 0.004, respectively).
In cirrhotic patients, NO was produced in excess by the alveolar compartment of the lungs. Alveolar NO production was associated with hyperdynamic circulatory syndrome but not with arterial oxygenation impairment.
- Exhaled nitric oxide
- hepatopulmonary syndrome
- liver–lung interactions
Patients with advanced liver disease typically present with progressive systemic, splanchnic and pulmonary vasodilatation. This may lead to a hyperdynamic circulatory syndrome, which associates high cardiac index (CI) and fluid expansion in response to excessive vasodilatation 1, 2. Impaired arterial oxygenation, ranging from increased alveolar–arterial oxygen tension difference (PA–a,O2) to severe hypoxaemia, is also commonly present in patients with liver cirrhosis. In the absence of overt mechanical dysfunction of the lung, these oxygenation abnormalities may be a consequence of ventilation/perfusion mismatch and/or intrapulmonary shunting and/or diffusion impairment of oxygen 3. In addition, some patients develop hepatopulmonary syndrome (HPS), which consists of abnormal dilatation of pulmonary pre-capillary and capillary vessels either with or without pulmonary arteriovenous communications, whereas alveolar ventilation is preserved 4–6.
Nitric oxide (NO), a biologically active gas, is the main molecule responsible for the vasodilatation and multiple organ malfunctions that characterise hyperdynamic circulatory syndrome 7. A loss of NO bioavailability in the endothelial cells of the hepatic microcirculation contrasts with an increase in NO production by the endothelial cells in the arteries of the systemic and pulmonary circulatory systems. In animal models of HPS, pulmonary vascular dilatation, gas exchange abnormalities and blunted pulmonary vasopressor response are all linked to increased expression and activity of pulmonary NO synthases 5, 8–10. However, in humans, the role of NO in arterial oxygenation impairment is still under debate 11.
NO can be easily and noninvasively measured in exhaled air and is thought to reflect a balance between production and catabolism within the respiratory tract 12. Measurement of exhaled NO at multiple controlled expiratory flow rates allows partition into airway and alveolar NO components 13, 14, and the additional measurement of NO lung transfer enables the calculation of output of NO produced by the alveoli (V′A,NO) 15. In cirrhosis, alveolar NO concentration (CA,NO) is increased compared with normal subjects 16, but measurement of V′A,NO has not previously been reported.
In cirrhotic patients awaiting liver transplantation at our institution, we aimed to: 1) measure V′A,NO, and 2) assess the relationships between V′A,NO, oxygenation parameters and pulmonary haemodynamics.
MATERIALS AND METHODS
Study subjects
From November 2006 to October 2007, 29 patients awaiting liver transplantation at Toulouse University Hospital (Toulouse, France) were investigated. All the patients had biopsy-proven liver cirrhosis. Physical examination findings and blood data were analysed to determine the severity of liver disease according to the criteria of Child and Turcotte 17. None of the patients had primary lung disease. Patients were not included if they had primary cardiac disease (including systolic and diastolic left heart disease, and mitral and/or aortic stenosis and/or regurgitation) or portopulmonary hypertension. Subjects with allergy and/or asthma were also excluded. The study was approved by our institutional review board (Toulouse University Hospital) and informed consent was obtained from each patient.
Pulmonary function tests
Measurement of lung volumes and single-breath transfer factor of the lung for carbon monoxide (TL,CO) was performed according to the European Respiratory Society (ERS) guidelines 18, 19.
Arterial blood gases were analysed in patients’ breathing room air in a sitting position. PA–a,O2 was calculated as follows.
PA–a,O2 = PA,O2–Pa,O2 = FI,O2 (Patm–PH2O)–Pa,CO2/RER–Pa,O2
Where PA,O2is alveolar oxygen tension, Pa,O2 is arterial oxygen tension, FI,O2inspiratory oxygen fraction, Patm atmospheric pressure, PH2O water vapour partial pressure (47 mmHg), Pa,CO2 is arterial carbon dioxide tension and RER is respiratory exchange ratio (assumed to be 0.8). The diagnosis of HPS was based on the ERS recommendations 3.
Measurement of NO concentrations in exhaled air
Measurements were performed in the 29 patients and in 22 healthy controls. Control subjects were matched with patients for age and smoking habits. Current smokers were asked not to smoke for 24 h prior to NO measurement. Among subjects who were not current smokers, those who responded “no” to the question “Have you ever smoked for as long as a year?” were classified as nonsmokers, and those who responded “yes” were classified as ex-smokers 20. Patients and controls were asked to abstain from coffee and vegetables during the 24 h prior to NO measurement.
Measurement of exhaled NO fraction (FeNO) was performed as recommended by American Thoracic Society/ERS guidelines 21. Subjects exhaled against a positive pressure of 20 cmH2O and generated expiratory flows of 50, 100 and 200 mL·s−1. NO was detected with a chemiluminescent analyser (EndoNO 8000®; SERES, Aix-en-Provence, France) with a lower limit of detection of 1 ppb and an NO sampling rate of 30 L·h−1. Simultaneous measurements of FeNO and expiratory flow were used to calculate NO output. Three consecutive measurements of FeNO were performed for each expiratory flow and the calculated NO output values were represented as a function of the flow rates. Least-square linear regression over the NO output versus the flow-rate data was performed and the linearity of the relationship was verified, i.e. r2>0.90. CA,NO (ppb) and maximal bronchial output of NO (J'aw,NO; nL·min−1) were estimated according to the model recently described by Condorelli et al. 13, as follows.
CA,NO = S–I ((0.001 s·mL−1)/(0.53))
and
J'aw,NO = (I/0.53) × 0.06
Where S is the slope and I is the y-intercept of the linear regression over the NO output versus the flow rate.
Unlike the model of Tsoukias and George 14, the current model takes into account axial diffusion of NO from the airways that can “contaminate” the alveolar region, and so it is more relevant when estimating CA,NO 13.
Measurement of NO transfer
Transfer factor of the lung for nitric oxide (TL,NO) was measured during a single breath manoeuvre using automated apparatus (Medisoft, Dinant, Belgium). Subjects were in the sitting position and wore a nose clip. They inhaled a mixture containing 14% He, 21% O2 balanced with N2 mixed with an NO/N2 mixture (450 ppm NO/N2; Air Liquide Santé, Paris, France). The final concentration of NO in the mixture was 40 ppm and that of O2 was 19.1%. A breath-hold of 4 s was requested, followed by a rapid expiration. The first 0.9 L of expired gas was rejected and the following 0.9 L was sampled and analysed for NO concentration 22.
According to Perillo et al. 15, V′A,NO (nL·min−1) was calculated as the product of TL,NO (mL·min−1·mmHg−1) and CA,NO (ppb) as follows.
V′A,NO = TL,NO × CA,NO × (Patm–PH2O) × 10−3
Where Patm is atmospheric pressure and PH2O water vapour partial pressure (47 mmHg).
Right heart catheterisation
Right heart catheterisation was performed using a 7F, two-lumen, thermodilution pressure-measuring tipped catheter (Corodyn TD; Braun Medical, Bethlehem, PA, USA). Cardiac output was measured by the thermodilution technique.
Analysis
Data were expressed as median (1st–3rd quartile). Comparisons between more than two groups or subgroups were performed with the Kruskal–Wallis test. Comparisons between two groups or subgroups were performed with the Mann–Whitney U-test. Correlations were made by Spearman's test. A p-value <0.05 was considered as significant. Analysis was performed using Statview, version 5.0 (SAS Institute, Cary, NC, USA).
RESULTS
Demographic characteristics
Demographic and clinical characteristics of patients and controls are shown in table 1⇓. The majority of patients were male and had cirrhosis caused by alcohol abuse. No significant difference was observed in age, smoking habits or spirometric values between patients and controls. Cirrhotic patients with HPS had lower TL,CO than non-HPS and than healthy controls. PA–a,O2was significantly higher in HPS patients than in non-HPS patients. Cirrhotic patients had normal mean pulmonary artery pressure, high CI and low pulmonary vascular resistance.
Demographic, functional and haemodynamic characteristics of cirrhotic patients and healthy volunteers
NO measurements
Table 2⇓ summarises NO measurements in patients and controls. Median CA,NO, V′A,NO and J'aw,NO were significantly increased in cirrhotic patients compared with healthy controls. In cirrhotic patients, CA,NO, V′A,NO and J'aw,NO did not differ between patients without HPS (3.5 (2.9–6.5) ppb, 260 (178–338) nL·min−1 and 74 (56–116) nL·min−1, respectively) and patients with HPS (3.7 (2.5–7.0) ppb, 260 (175–359) nL·min−1 and 74 (58–130) nL·min−1, respectively). Patients and controls were either active smokers or nonsmokers. In healthy smoking controls, J'aw,NO was significantly lower than in nonsmokers but CA,NO and V′A,NO were similar. In cirrhotic patients, smoking habits had no effect on CA,NO, V′A,NO and J'aw,NO.
Nitric oxide(NO) measurements in control subjects and patients with liver cirrhosis
Relationship between NO measurements and gas exchange parameters
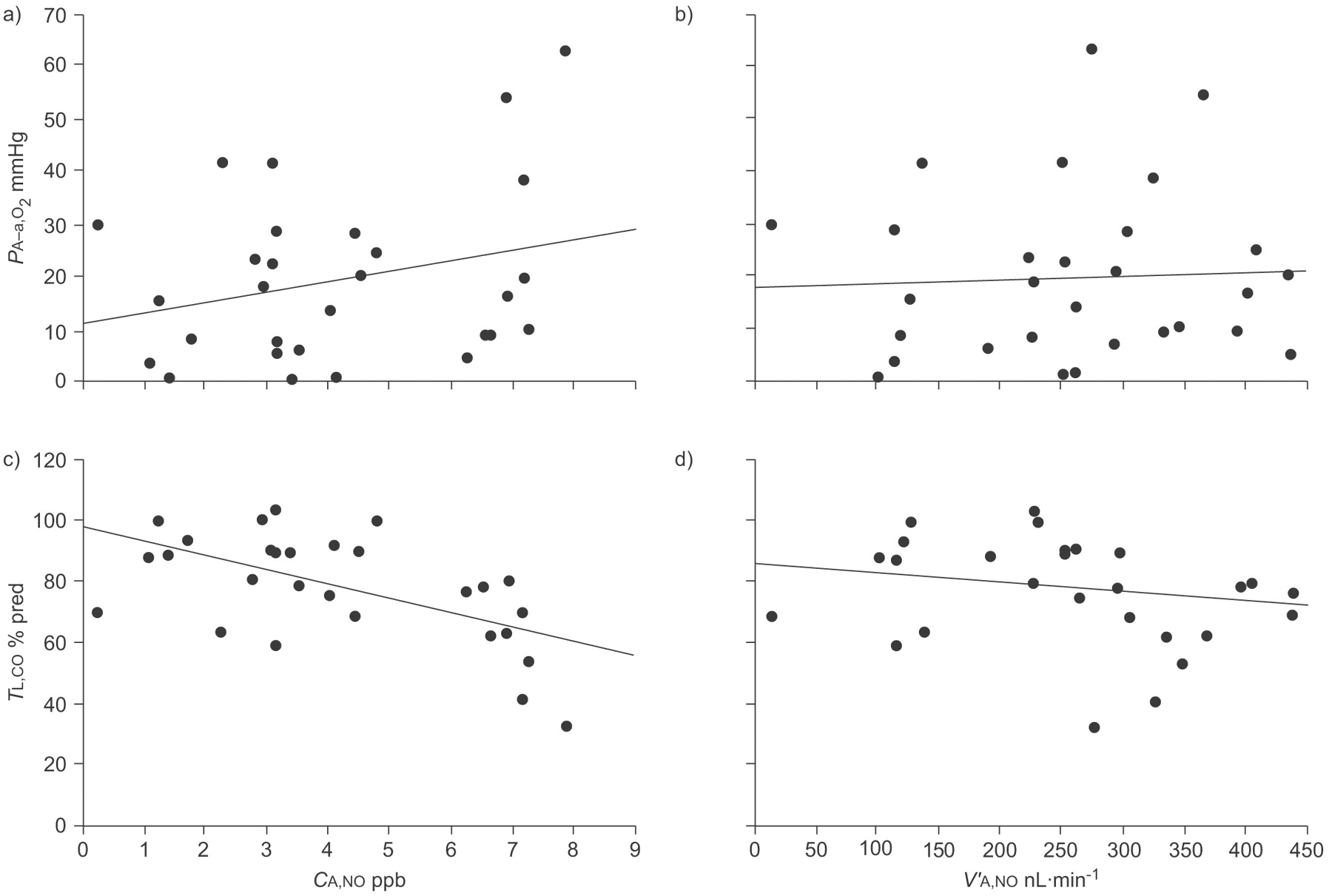
We failed to find any correlation between PA–a,O2and CA,NO or between PA–a,O2 and V′A,NO (fig. 1⇓). There was significant correlation between TL,CO and CA,NO. However, there was no correlation between TL,CO and V′A,NO (fig. 1⇓). J'aw,NO was not correlated either with PA–a,O2or with TL,CO (data not shown).
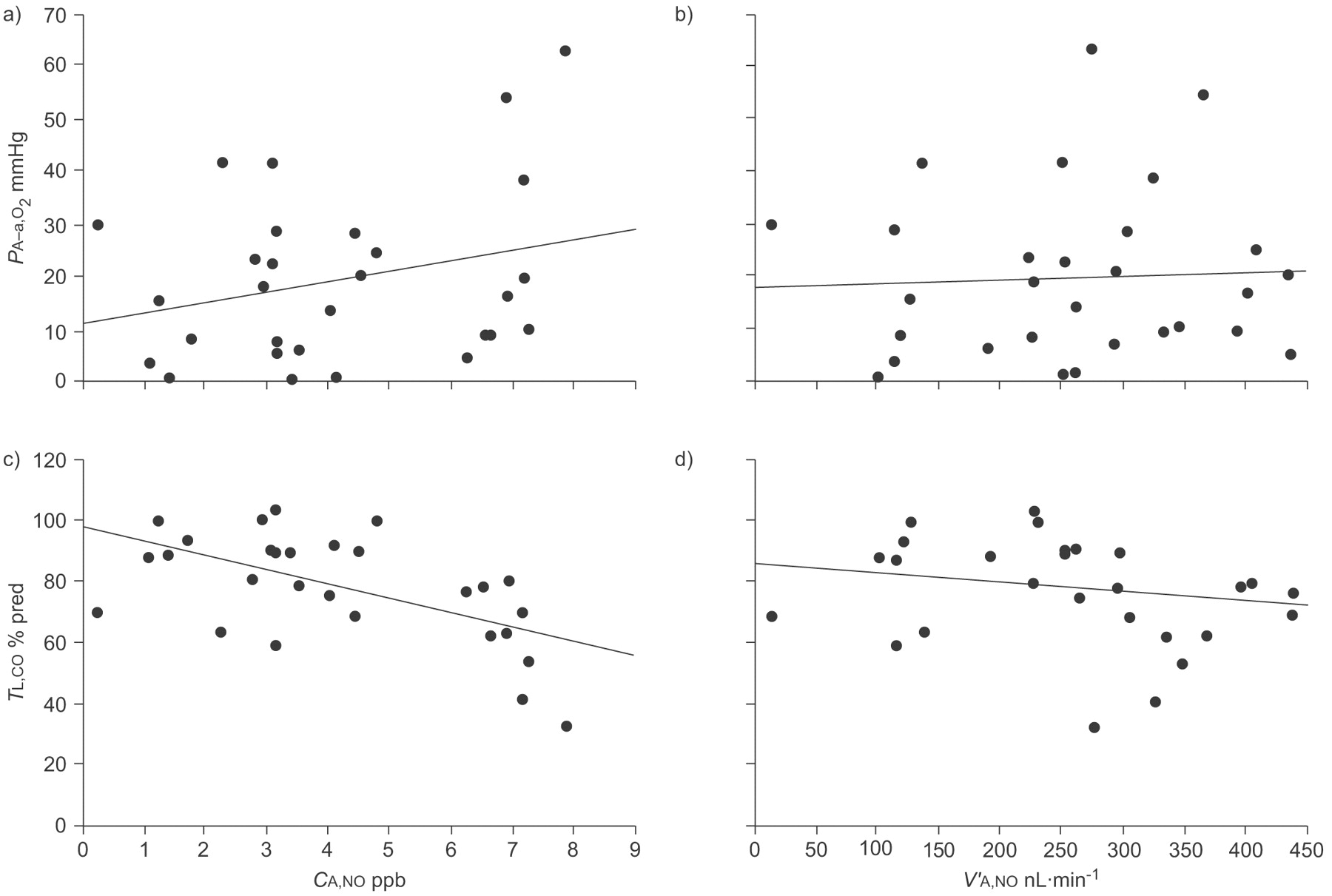
The relationship between alveolar nitric oxide concentration (CA,NO) and oxygenation parameters in 29 cirrhotic patients. a, b) There was no correlation between CA,NO and alveolar–arterial oxygen tension difference (PA–a,O2), or between alveolar nitric oxide output (V′A,NO) and PA–a,O2. c, d) There was a weak but significant correlation between CA,NO and transfer factor of the lung for carbon monoxide (TL,CO), but no correlation between V′A,NO and TL,CO. a) r = 0.18, p = 0.33. b) r = 0.09, p = 0.62. c) r = -0.57, p = 0.001. d) r = -0.17, p = 0.33.
Relationship between NO measurements and haemodynamics
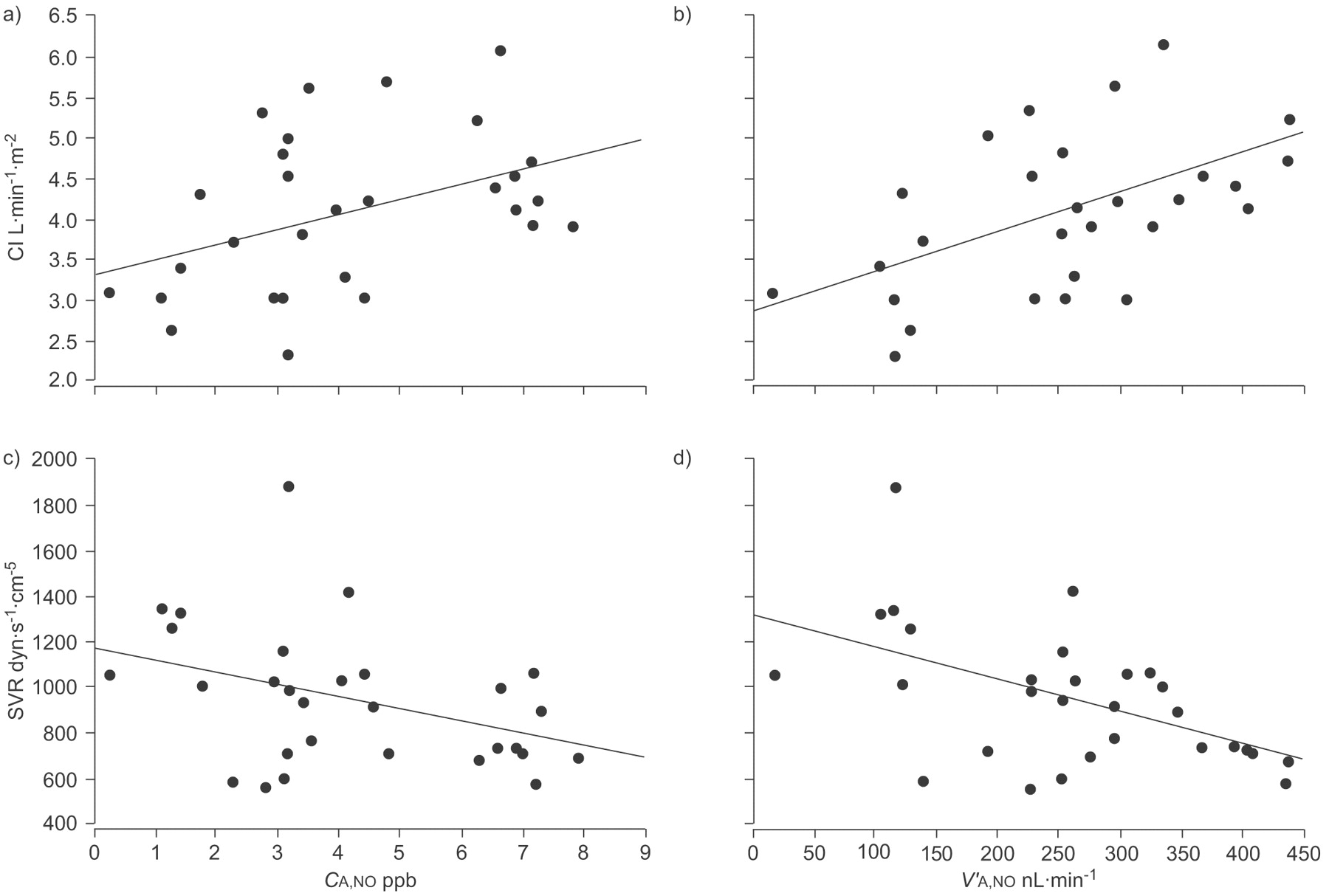
CI correlated positively with CA,NO (r = 0.41, p = 0.03) and V′A,NO (r = 0.56, p = 0.001) (fig. 2⇓). Systemic vascular resistance (SVR) correlated negatively with CA,NO (r = -0.39, p = 0.04) and with V′A,NO (r = -0.52, p = 0.004) (fig. 2⇓). J'aw,NO was not correlated either with CI or with SVR (data not shown).

{kind=link}
{kind=link}
The relationship between alveolar nitric oxide concentration (CA,NO) and haemodynamic parameters in 29 cirrhotic patients. a, b) Cardiac index (CI) correlated positively with CA,NO and with alveolar nitric oxide output (V′A,NO). c, d) Systemic vascular resistance (SVR) correlated negatively with CA,NO and with V′A,NO. a) r = 0.41, p = 0.03. b) r = 0.56, p = 0.001. c) r = -0.39, p = 0.04. d) r = -0.52, p = 0.004.
DISCUSSION
Our main findings are that in cirrhotic patients: 1) V′A,NO was increased compared with healthy volunteers; and 2) V′A,NO failed to correlate with PA–a,O2 but correlated positively with CI.
An increase in FENO in cirrhotic patients was first reported >10 yrs ago. Cremona et al. 23 and Rolla et al. 24 showed that NO concentrations measured in exhaled air from patients with advanced liver cirrhosis were increased compared with controls. It must be stressed that the technique used to collect exhaled air in these studies was markedly different from the current recommendations 21. Exhalations were performed without closure of the soft palate and patients wore a nose clip, two conditions which are now known to considerably increase the nasal contribution of NO measured in exhaled air 21. Moreover, expiratory flow rates were not recorded, and it has been clearly demonstrated that NO concentration in exhaled air is inversely dependent on expiratory flow rate 14. By measuring exhaled NO at multiple controlled expiratory flow rates and applying the two-compartment model of Tsoukias and George 14, Delclaux et al. 16 showed that CA,NO was increased in cirrhotic patients. However, this two-compartment model neglected the axial diffusion of NO from the airway tree, which can contaminate the alveolar region and so lead to a falsely elevated estimate of CA,NO. Therefore, we used the model recently described by Condorelli et al. 13, which takes axial diffusion of NO into account when estimating CA,NO. This model was initially tested in a limited number of healthy subjects and CA,NO was found to be near zero 13. By contrast, in our series of cirrhotic patients we found that CA,NO estimated with this model was significantly higher than in controls, indicating that “contamination” of the alveolar compartment by NO from the airways did not account for increased values of CA,NO in liver cirrhosis.
Increased CA,NO may suggest either an increase of V′A,NO and/or a reduction of the transfer of NO from the alveolar compartment to the vascular compartment of the lungs (TL,NO) 14. In patients with systemic sclerosis, Girgis et al. 25 concluded that the most likely cause of increased CA,NO was decreased transfer of alveolar NO to the lung vessels, but TL,NO was not measured.
To the best of our knowledge, alveolar NO production has not previously been studied in cirrhotic patients. In our study, measurement of TL,NO in addition to estimation of CA,NO enabled us to demonstrate that the most likely cause for increased CA,NO in cirrhotic patients was an increase of alveolar NO production. However, CA,NO and V′A,NO are not strictly equivalent in these patients, as highlighted by the correlation between CA,NO and TL,CO, which contrasts with the absence of correlation between V′A,NO and TL,CO.
In animal models of cirrhosis and portal hypertension, enhanced pulmonary production of NO has been clearly implicated in the development of hypoxaemia and hyperdynamic syndrome 8, 9, 26, 27. In cirrhotic patients, the relationships between pulmonary alveolar NO production, hyperdynamic circulation and gas exchange abnormalities remain uncertain. We found no correlation between alveolar NO (CA,NO and V′A,NO) and PA–a,O2. In contrast, Rolla et al. 24 reported a strong correlation between PA–a,O2and exhaled NO concentration, but the technique of exhaled air collection differed greatly from the methods currently recommended. Delclaux et al. 16 found a correlation between CA,NO and PA–a,O2 16. The differences with our results may be due to: 1) differences in study population, as in the study by Delclaux et al. 16 patients had more severe HPS; and 2) a different mathematical model used to estimate CA,NO 16. Interestingly, the absence of correlation between V′A,NO and PA–a,O2 may explain, at least in part, the results of Gomez et al. 11, who reported that acute inhibition of pulmonary NO-synthase activity (and thus acute inhibition of pulmonary NO production) by nebulised NG-nitro-l-arginine methyl ester (l-NAME) had no effect on PA–a,O2. We also found that alveolar NO (CA,NO and V′A,NO) correlated positively with CI. Increased cardiac output in response to excessive vasodilatation is a hallmark of hyperdynamic circulatory syndrome 3, 6. A possible interpretation of our finding is that NO production may be similarly increased in both the pulmonary and the systemic vessels in cirrhotic patients. In accordance with this interpretation, Gomez et al. 11 showed that nebulised l-NAME decreased CI and increased both pulmonary and systemic vascular resistances in patients with hepatopulmonary syndrome.
We aimed to minimise factors confounding the measurement of FeNO. We verified that patients had neither allergy nor asthma because exhaled NO concentrations may be increased in these diseases 28. Patients were also asked not to drink coffee on the day of measurement because caffeine has been shown to briefly reduce FeNO (for ≤4 h) 29. As nitrate-rich nutrition is presumed to increase exhaled NO concentration 30, patients were given a vegetable-free hospital diet during the 24 h prior to the NO measurements. However, 14 out of the 29 patients were regular smokers. This could be considered a bias because smoking decreases FeNO, especially at relatively low expiratory flow rates (i.e. under 100 mL·s−1) 31, 32. The smoking habits of the controls are not detailed because if exhaled NO concentrations are measured according to the current recommendations, no dose–response relationship between the number of cigarettes smoked and the levels of exhaled NO has been found in healthy subjects 20. In accordance with previous results on the effects of tobacco smoking on exhaled NO, we found that smokers without cirrhosis (controls) had lower NO airway production than nonsmokers. Smoking habits had no significant influence on CA,NO and V′A,NO in control subjects. Moreover, our results in cirrhotic patients are in accordance with the findings of Delclaux et al. 16, who found no significant difference in CA,NO or bronchial and alveolar NO outputs between smoking and nonsmoking cirrhotic patients.
We acknowledge some limitations in this study. First, we studied a small series of patients. Secondly, we included a large majority of patients without HPS or with mild-to-moderate HPS. Therefore, caution is required in extending our results to patients with severe or very severe HPS.
In summary, our results indicate that NO is produced in excess by the alveolar compartment of the lungs in advanced liver cirrhosis. In our study, alveolar NO production was associated with hyperdynamic circulatory syndrome but not with arterial oxygenation, suggesting that acute inhibition of alveolar NO production may decrease cardiac output without altering gas exchanges. Further measurements of alveolar NO output, pulmonary haemodynamics and gas exchanges following long-term NO-synthase inhibition or liver transplantation may help to understand the role of alveolar NO synthesis in advanced liver diseases.
Statement of interest
None declared.
- Received September 28, 2008.
- Accepted December 14, 2008.
- © ERS Journals Ltd