



Molecular evidence for the role of mycobacteria in sarcoidosis: a meta-analysis
- D. Gupta,
- R. Agarwal,
- A. N. Aggarwal and
- S. K. Jindal
- Dept of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
- D. Gupta, Dept of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research, Sector-12, Chandigarh -160012, India. Fax: 91 1722748215. E-mail: dheeraj{at}indiachest.org
Abstract
The aetiology of sarcoidosis is currently unknown. Due to the clinical and histological similarities between sarcoidosis and tuberculosis, the role of mycobacteria has been repeatedly investigated as an aetiological agent for sarcoidosis. The current meta-analysis aimed to evaluate the available molecular evidence on the possible role of mycobacteria in the development of sarcoidosis.
The MEDLINE, EMBASE, CINAHL, DARE and CENTRAL databases were searched for relevant studies published from 1980 to 2006, and studies evaluating the presence of mycobacteria using molecular techniques in biological samples of patients with sarcoidosis were included in the current analysis. The 95% confidence intervals (CI) were calculated for the expected proportion (of individual studies); the data was then pooled to obtain a summary success rate with 95% CI. The odds ratio (95% CI) was also calculated in order to assess the presence of mycobacteria in samples of patients with sarcoidosis versus those from nonsarcoidosis control samples.
The database search yielded 31 studies. All studies used polymerase chain reaction for nucleic acid amplification followed by identification of nucleic acid sequences specific for different types of mycobacteria. Overall, 231 out of the 874 patients were positive for mycobacteria with a positive signal rate of 26.4 (23.6–29.5%), and the odds of finding mycobacteria in samples of patients with sarcoidosis versus controls were 9.67 (4.56–20.5%) using the random effects model and 19.49 (11.21–35.54%) using the exact method. There was methodological and statistical heterogeneity and evidence of publication bias.
The results of the current study illustrate a demonstrable mycobacterial presence in sarcoidosis lesions suggesting an association between mycobacteria and some cases of sarcoidosis. To avoid methodological diversity, larger multicentre trials with a central laboratory for sample testing should be designed.
- Mycobacteria
- polymerase chain reaction
- sarcoidosis
- tuberculosis
Sarcoidosis is a granulomatous disease of unknown aetiology characterised by noncaseating granulomas involving the lung, lymph nodes and other organs 1. It is believed that granulomatous diseases may be the result of continued presentation of a poorly degradable antigen 2. In the case of sarcoidosis, this agent remains unclear. Numerous aetiological agents have been incriminated, both infective and noninfective 3. Noninfective agents have been implicated because of their epidemiological association 4, but these implications have not stood the test of time 5. Currently, the focus is on infective agents, and the two strongest contenders are Propionibacterium and Mycobacterium 6. A recent study of culture and PCR analysis of Propionibacterium species from lung tissues and lymph nodes from subjects with and without sarcoidosis, showed Propionibacterium acnes to be a common commensal bacteria in peripheral lung tissues and mediastinal lymph nodes, suggesting that it is less likely to be the trigger for sarcoidosis 7.
Since sarcoidosis was first described, there has always been a belief that the disease is in some way related to tuberculosis 8. However, the inability to identify mycobacteria by histological staining or culture from pathological tissues continues to be one of the strongest arguments against a potential role for mycobacteria. Of late, molecular analysis (such as polymerase chain reaction (PCR) techniques) for nucleic acids of putative agents serves as an alternative method for isolating fastidious organisms. This method has been used successfully in identifying Tropheryma whippelii as a causative agent for Whipple's disease 9 and coronaviruses 10 as an agent for severe acute respiratory syndrome.
Several studies have been carried out using molecular techniques to study the presence of mycobacteria in sarcoidosis patients 5. The aim of the current study was to systematically analyse the available literature on this issue.
MATERIAL AND METHODS
Search strategy and selection criteria
To identify the studies for inclusion in this review, all authors independently searched the National Library of Medicine's MEDLINE, EMBASE, CINAHL, DARE and CENTRAL databases for relevant studies published from 1980–2006 using the terms: sarcoidosis AND mycobacteria; sarcoidosis AND mycobacterium; sarcoidosis AND Mycobacterium tuberculosis; and sarcoidosis AND tuberculosis. Bibliographies of all selected articles and review articles that included information on the relationship between sarcoidosis and mycobacteria were reviewed. In addition, the current authors' studies were also reviewed. All the studies irrespective of language were identified.
Data abstraction
The abstracts of the studies were independently reviewed by two authors (R. Agarwal and D. Gupta), who were not blind to study details. Any disagreement was resolved by discussion between the authors. Included studies were those that evaluated the presence of mycobacteria using molecular techniques in samples (both histological and cellular) of patients with sarcoidosis. Data was recorded on a standard data extraction form. The following items were extracted. 1) Publication details including title, author(s) and other citation details. 2) The number of patients with sarcoidosis and the number and type (tissue or cellular samples) of samples used for analysis. 3) Details of the molecular test used to evaluate the presence of mycobacteria in samples. 4) The type of mycobacteria (tuberculous versus nontuberculous). 5) Percentage of the samples positive for mycobacteria in patients with sarcoidosis versus the percentage of positive control samples.
Determination of the pooled treatment effect
To calculate the percentage of mycobacteria-positive sarcoid samples, binomial proportions were used in which the numerator was success in isolation of mycobacteria and the denominator was the total study sample. The expected proportion was the success rate of each study included and 95% confidence intervals (CIs) were calculated for the expected proportion using the Newcombe–Wilson method 11, 12. Data from individual studies was then pooled and a summary success rate with 95% CI was calculated by summing up the rate of mycobacteria-positive samples as the numerator and the total number of samples evaluated as the denominator 13.
The odds ratio (OR) and 95% CI were also calculated to assess the presence of mycobacteria in sarcoisosis samples versus controls. The results from individual studies were pooled using the random effects model of DerSimonian and Laird 14 and the exact method with conditional maximal likelihood as described by Martin and Austin 15.
Assessment of heterogeneity
The extent of heterogeneity was assessed by the Cochran Q-statistic (weighted sum of squared differences between individual study effects and the pooled effect across studies, with the weights being those used in the pooling method). The level at which heterogeneity should be diagnosed is unclear, given that the Q-statistic has low power, and Fleiss 16 recommended a p-value of >0.1.
The impact of heterogeneity upon the pooled estimates of the individual outcomes of the meta-analysis was assessed using the Chi-squared test and/or the I2 tests (this measures the extent of inconsistency among the studies' results and is interpreted as approximately the proportion of total variation in study estimates that is due to heterogeneity rather than sampling error). An I2 value >40% indicates significant heterogeneity. As the Chi-squared test has a low sensitivity for detecting heterogeneity, a p-value <0.1 was considered significant for the presence of statistical heterogeneity 17.
Assessment of publication bias
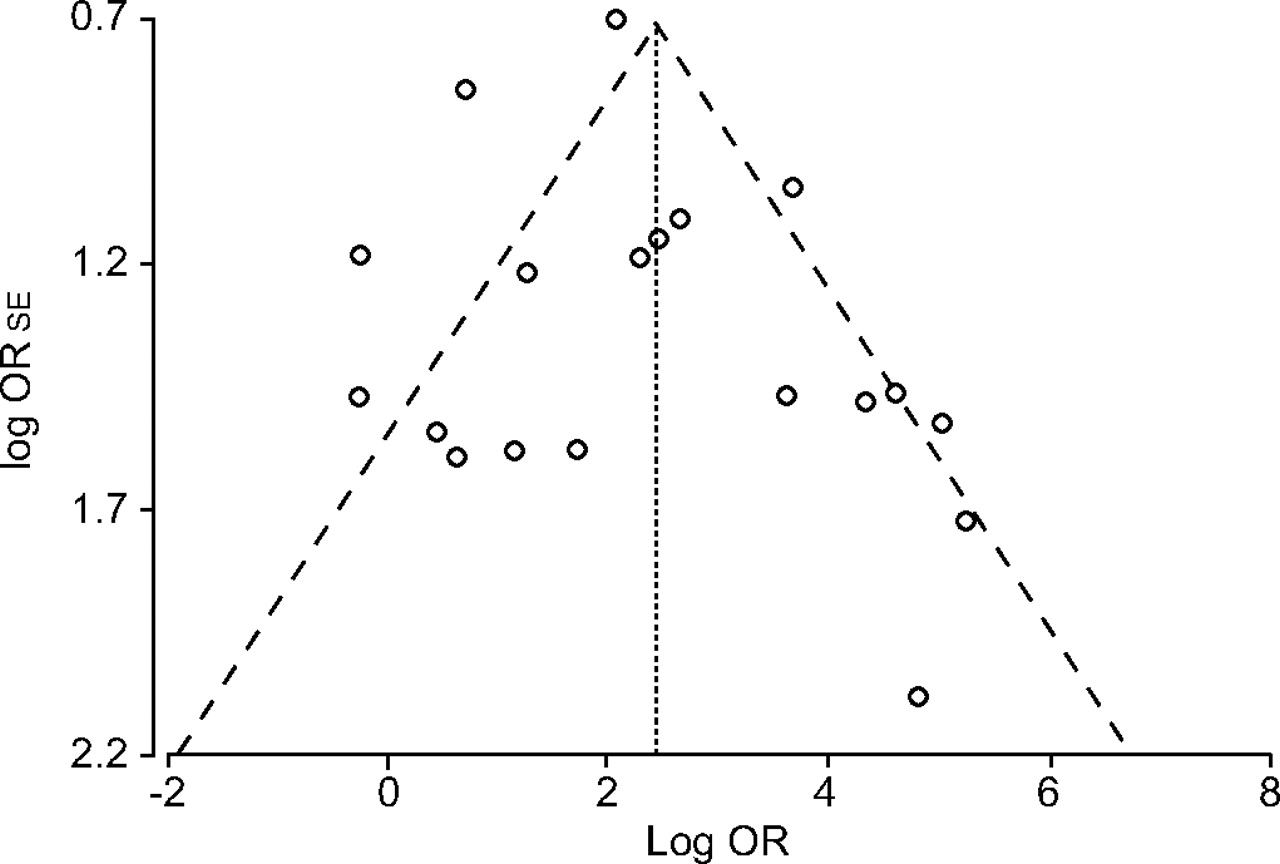
The presence of a small study effect was examined by means of funnel plots 18. The funnel plot is a measure of the log of the OR (in the X-axis; a measure of diagnostic accuracy) against the standard error of the log of the OR (in the Y-axis; an indicator of sample size). Each point represents each study in the meta-analysis. The central line indicates the summary OR with other lines indicating the 95% CI. In the absence of publication bias, the OR estimates from smaller studies are expected to be scattered above and below the summary estimate, producing a triangular or funnel shape.
Institutional review board clearance was not required for this study as this was a meta-analysis of published studies.
RESULTS
The initial data search yielded a total of 1,718 citations (fig. 1⇓). On review of the title and abstract, 1,679 articles were excluded as they did not meet the inclusion criteria. A total of 40 studies were identified that used nucleic acid amplification techniques to identify mycobacterial nucleic acid sequences. Of these 40 studies, nine were further excluded; seven were single patient case reports 19–25, one study analysed mycobacterial DNA in nonsarcoid granulomatous disease 26 and one study had re-analysed the Mycobacterium tuberculosis-positive samples of sarcoid patients using a different technique to further clarify the type of M. tuberculosis 27. Therefore, 31 articles were selected for analysis (table 1⇓) 28–58.

Flow diagram of the current trial selection.
Studies evaluating the role of mycobacteria in sarcoidosis using molecular techniques
All studies provided detailed methodology and the meta-analysis included studies from around the world (table 1⇑). In total, the studies involved 882 samples (711 tissue samples and 71 fluid samples from which cells were isolated and further analysed) from 874 patients with proven sarcoidosis and 611 samples from 600 controls (lung cancer, bronchiectasis and other lung disorders). All but six studies 36, 37, 46, 49, 54, 55 were case–control studies where the cases and controls have been randomly sampled; all cases who have clinically confirmed sarcoidosis have been included. All but five 28, 30, 32, 54, 55 studies used positive control samples of patients with proven mycobacterial infections. The details regarding the sites of biopsy were not provided by all studies but from the available data, lymph node samples (n = 356) were used in most studies, followed by the lung (n = 146) and others (bronchial fluid (n = 70), skin (n = 56), others (lacrimal gland, pituitary; n = 12), cerebrospinal fluid (n = 1)). All studies used PCR for nucleic acid amplification followed by identification of nucleic acid sequences specific for different types of mycobacteria (table 1⇑). Most studies used primers to detect the presence of M. tuberculosis complex (MTC) and nontuberculous mycobacteria (NTM); however, some studies detected only M. tuberculosis 30, 39, 40, 43–45, 47, 54, 55, 57, 58 and some atypical mycobacterial species alone 34, 37. As there were more samples than patients, which can lead to both over- and under-estimation bias, further patient samples were excluded (eight samples excluded: six negative and two positive) and only 874 patients with 874 samples were included. Similarly, 600 controls had 611 samples evaluated, therefore 11 samples were excluded (two positive and nine negative).
Of the 874 samples, 187 were positive for MTC and 43 samples were positive for NTM; one sample was found to have a nucleic acid sequence for both types of mycobacteria (table 1⇑). In total, 231 samples from 874 patients were positive for mycobacteria with a positive signal rate of 26.4 (23.6–29.5%; fig. 2⇓). Seven studies found a positive signal rate >50%, eight studies had a rate between 20–50%, nine studies found a positive signal in <20% and seven studies did not find any evidence of mycobacteria in the analysis (fig. 2⇓).

Forest plot of the mycobacterial DNA prevalence rate in samples of patients with sarcoidosis. CI: confidence interval.
Of the 31 studies, six had no control arm and were excluded for the calculation of OR and 95% CI. Five studies specifically reported on the detection of NTM (104 cases and 145 controls), and the odds of finding NTM was 19.63 (2.74–140.64) and 30.72 (8.32–177.18) by the random effects model and exact method, respectively (fig. 3⇓, table 2⇓). The odds of finding both MTC and NTM (680 cases and 600 controls) in samples of patients with sarcoidosis versus controls were 9.67 (4.56–20.5) using the random effects model (fig. 3⇓, table 2⇓) and 19.49 (10.86–37.1) using the exact method.

Forest plot showing the presence of mycobacteria in samples from sarcoidosis patients versus control samples. ▪: odds ratio (OR); ––––: 95% confidence interval, random effects model. NTM: nontuberculous mycobacterium.
Forest plot data of the presence of mycobacteria in samples from sarcoidosis patientsversus control samples
There was methodological (table 1⇑) and statistical heterogeneity (Cochran Q-statistic 30.31, p = 0.034; I2 40.6 (8.2–73.1%); Chi-squared 35.02, p<0.0001). The funnel plot also showed evidence of publication bias (fig. 4⇓).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot comparing log odds ratio (OR) versus the standard error (se) of log OR. ○: trials included in the meta-analysis; ·····: summary log OR; – – – : 95% confidence intervals. Asymmetry about the pooled OR line is consistent with the presence of publication bias.
DISCUSSION
Meta-analysis is a statistical procedure that integrates the results of several relevant independent studies and allows a common conclusion to be drawn from an entire body of research. It provides a more precise estimate of a treatment effect, and may explain heterogeneity between the results of individual studies. The results of the present meta-analysis indicate that almost 30% of patients with sarcoidosis have the presence of mycobacterial nucleic acids within the lesions and there are significant odds of finding mycobacteria in samples from sarcoidosis patients (OR = 9.67 and 19.49 by the random effects and exact methods, respectively), thereby suggesting an association between mycobacteria and sarcoidosis. In addition to the conventional technique of random effects meta-analysis, the partial polynomial multiplication algorithm 15 was also used in the present study; because the method is exact the sparseness of individual studies in the current analysis was not an issue. Although the OR doubled with the exact technique, the CIs also widened, suggesting a weaker but definite association.
There are numerous factors that favour mycobacteria as a trigger for sarcoidosis. These include: histopathological appearances of the granulomas 2; reports of mycobacterial disease either existing coincidentally, succeeding or pre-dating sarcoidosis 59, 60; and the finding of mycobacteria in occasional granulomas of sarcoidosis 61–63. Passage experiments have also suggested that mycobacteria with characteristics of M. tuberculosis may be the incriminating agent 64–67. Recent studies on humoral immunity to mycobacterial antigens from sarcoidosis patients have renewed interest in the potential of mycobacteria in sarcoidosis 68. It has also been suggested that the organism might exist in a cell-wall deficient bacteria (L-form) and may be difficult to isolate 69. However, there is no clear evidence to determine whether the tubercle bacillus is really the cause of sarcoidosis.
The presence of mycobacteria can be considered incidental but it may also suggest that sarcoid lesions result as a continued reaction to mycobacteria. The isolation of genetic material from mycobacteria in granulomas of sarcoidosis, at least, suggests that the granuloma was initiated by mycobacteria but whether the organism is currently viable is a different question.
Do mycobacteria have a role to play in causing sarcoidosis? The case of sarcoidosis does not meet Koch's postulates but this is not always true and many pathogens, for example Pneumocystis jiroveii, cannot be grown outside the host but do clearly cause pulmonary disease. It is also possible that these mycobacteria may be different from the conventional mycobacteria in that they may be difficult to culture using existing microbiological techniques. In fact, the organism causing Whipple's disease (T. whippelii) was grown in culture using a technique that added the cytokine interleukin-4, which causes deactivation of macrophages 70. The present meta-analysis does provide evidence to suggest an association in ≥30% of cases, but future research is necessary to establish the cause of this association.
Interestingly, the presence of mycobacteria also seems to influence disease outcome, with mycobacterial nucleic acid-negative patients showing better outcomes 58. In one study it was reported that all patients with mycobacteria-positive samples did not respond to the typical immunosuppressive treatment for sarcoidosis but the remaining mycobacteria-negative patients reacted positively to the same therapy 46. Also, patients with positive mycobacterial nucleic acid samples have been found to show a tendency for a chronic disease course compared with mycobacteria-negative patients 55.
Can treatment with anti-tuberculous drugs alter the natural history and course of sarcoidosis? Very few trials have been conducted in the past and the results of these trials have been discouraging. These trials were generally small studies and were limited by time-bias and the use of older regimens based on isoniazid, amino-salicylic acid and streptomycin 71–76. The current authors' experience (in a high tuberculosis-endemic zone) with a large (n = 500) number of patients with sarcoidosis show that a substantial number (on an average 40%, unpublished data) of patients are treated for tuberculosis and anti-tuberculous therapy probably does not influence outcome in these patients. However, this data reflects only the patients who have been referred to the tertiary care institute and this observation needs to be confirmed by a randomised controlled trial.
The major limitation of the present systematic review is reflected in the highly variable results with rates of mycobacteria-positive samples ranging 0–100%, which precludes any definite causal association. The reasons may be manifold and include issues of technique (including the type of mycobacteria detected) and thus the sensitivity and specificity of PCR 77; the organ specificity of the biopsy specimens may also have some role to play. Some variation may also be observed because of the difference in local environmental exposures and the fact that some sarcoidosis patients may have a disorder initiated by organisms or triggers other than mycobacteria.
In conclusion, the results of the present study suggest an association between mycobacteria (both Mycobacteria tuberculosis complex and nontuberculous) and sarcoidosis. These mycobacteria might be members of slow-growing types with low pathogenic potential but the capability of eliciting a type IV immune response. To avoid methodological diversity, larger multicentre trials with a central laboratory for sample testing should be designed.
- Received January 8, 2007.
- Accepted May 8, 2007.
- © ERS Journals Ltd