



Annual risk of infection with Mycobacterium tuberculosis
- H. Rieder
- H. Rieder, International Union Against Tuberculosis and Lung Disease, Jetzikofenstr. 12, 3038 Kirchlindach, Switzerland. E-mail: TBRieder@tbrieder.org
Abstract
The average annual risk of infection with Mycobacterium tuberculosis is a calculated average from an observed prevalence of infection, approximating the incidence of infection. It has the potential to be informative about the extent of transmission in a community. Where serial surveys are available, secular trends in transmission might be ascertained. The prerequisite for calculating the average annual risk is the successful determination of the prevalence of infection. Difficulties arising with tuberculin skin-test surveys include logistical problems in sampling a representative portion of the population. Therefore, a compromise assesses the prevalence of infection among school children as an indicator of transmission in the community at large. The utilisation of tuberculin surveys is further compounded by the unpredictable specificity of the tuberculin skin test and, thus, the predictive value of a positive test result. Statistical approaches using mixture analysis may overcome this problem to some extent, but the experience is limited. Cytokine-derived assays, such as the interferon-γ release assays, are promising in providing higher specificity, but they require venepuncture.
- Epidemiology
- tuberculosis
SERIES “CONTROVERSIAL ISSUES IN TUBERCULOSIS”
Edited by A. Torres and J. Caminero
Number 2in this Series
An understanding of the epidemiology of tuberculosis can best be obtained by using a model that follows the sequence of its pathogenesis from exposure to latent infection to overt tuberculosis, and to death from tuberculosis 1. However, our knowledge of the epidemiology of tuberculosis has historically moved in the opposite direction, from the description of mortality, later to morbidity, and finally to understanding the role of latent infection.
The purpose of this paper is to summarise the historical and present role in the assessment of the average annual risk of infection with Mycobacterium tuberculosis, and its contribution to the understanding of the dynamics of tuberculosis epidemiology.
Development of the risk of infection as a model
In 1934, Muench 2 proposed a means to derive average annual rates of infection incidence from observed infection prevalence using, among others, the example of infection with M. tuberculosis. In 1957, Nyboe 3 formulated the simplest model to estimate expected prevalence (P) of infection from a known constant risk (R) by age and calendar year, i.e. P = 1–(1–R)a, where a is the age at which the observed prevalence is expected. Solved for R, the following is obtained: R = 1–(1–P)1/a. This is now the standard approach to derive the average annual risk from prevalence of infection under the assumption of no change over calendar time 4, 5. This is, however, an assumption that is more likely to be wrong than correct. Figure 1⇓ shows that the true incidence of infection is likely to change over calendar time; it may decline, it may increase, or it may be a mixture of ups and downs, yet a calculation of the average annual risk may yield precisely the same results. This shortcoming had also been pointed out by Nyboe 3. This author also highlighted the difficulties in separating those infected from those who are not because of the often ubiquitous presence of sensitising environmental mycobacteria that lead to nonspecific cross-reactions.
First, the changes of risk over calendar time were addressed in the work of the Tuberculosis Surveillance and Research Unit (TSRU). The TSRU developed a model of the dynamics, i.e. taking calendar changes in the risk of infection into account to ascertain changes from a series of tuberculin skin-test prevalence surveys 6. If serial tuberculin skin-test surveys are available, the point in time b+x, which lies between calendar time b, at which the tested cohort was born, and calendar time b+a, the calendar time at which the survey was conducted, can be determined. With this approach, the risk of infection becomes a better approximation of the average annual incidence of infection in the community. This model was developed using data from Dutch army/navy recruits who were persons of approximately the same age. It neglects any variations of the infection risk in the community that are linked to important variables, such as age and sex, which have been shown to vary considerably within the same calendar year 7, 8.
Secondly, the reduced specificity of the tuberculin skin test in areas where cross-sensitisation is frequent was not addressed by the TSRU report 6, largely because it was not of particular relevance in The Netherlands at the time the data had been collected.
Tackling these issues is of relevance as it is now clear that there is a central role of incidence and prevalence of infection in the epidemiology of tuberculosis 9. Tuberculosis has no defined incubation period and, thus, cases of tuberculosis will continue to emerge as long as there are individuals who harbour latent infection with M. tuberculosis. Therefore, knowledge of the risk of infection and its secular trends does not only give information about the past, but it is also an important piece of information that can provide insight into the likely prospects for the future.
Measuring the incidence of infection with Mycobacterium tuberculosis
If the primary interest is in assessing the incidence of infection with M. tuberculosis in a community, a legitimate question is why a detour has to be made to derive the risk of infection from prevalence, rather than directly measuring the incidence of infection. There are several impediments to doing that. Most important is that even where the incidence of infection is relatively large, i.e. typically 1–3% 4, 5, the change is nevertheless so small as to require repeated tests of a large population. The small prevalence entails a poor predictive value of a positive test result. Repeat testing of low-grade reactors entails the risk of boosting, so called because the induration size tends to increase on repeat testing even if no infection was acquired in the interim between the two tests 10. While a methodology has been developed to address the boosting problem in incidence surveys 11, it has never gained wide acceptance.
Assessing changes in transmission
The quality of global tuberculosis notifications to the World Health Organization (WHO) has been very poor in the past, undoubtedly not reflecting the worldwide problem 12. Thus, the WHO decided to alternatively ascertain the average annual risk of infection to get a better handle on changes in transmission of M. tuberculosis in various countries from which such information was available up to the mid-1980s.
The analyses were based on a review of all tuberculin skin-test surveys among children, representing countries from all but the European Region (currently consisting of 54 countries, omitted on purpose) of the WHO Regions, which are internationally defined by the United Nations. All surveys available to the WHO that met pre-defined criteria on survey quality were included in the analysis 4, 5. These analyses showed that the risk of infection among children declined in many regions, albeit to a very different extent, from several per cent each year to virtually no change. While the latest survey reported in this analysis was conducted in 1987, the majority was carried out before HIV infection could have impacted to a great extent on the survey. Furthermore, the age group in which these surveys were carried out were beyond survival of a perinatally acquired HIV infection and too young to have sexually transmitted HIV infection.
This often slow decline was not particularly surprising as national tuberculosis programmes in many of the surveyed countries were either nonexistent 13 or chaotic at best 14. When the International Union Against Tuberculosis and Lung Disease (The Union) initiated its model programmes in collaboration with some of the poorest countries in the world 15, determining the risk of infection among school children was to be an integral part for ascertaining programme effectiveness.
Practical problems encountered
Tanzania was the first country to implement, in collaboration with The Union, what is now known as the DOTS strategy 16. The results of the tuberculin skin-test surveys were presented at TSRU meetings 17–19, but were never published in the formal biomedical literature. Several major obstacles were encountered when attempting to measure the extent of impact of the national control programme on the transmission of tubercle bacilli.
First, the coverage with bacilli Calmette-Guérin (BCG) vaccination made it necessary to exclude more than half of the eligible children from analysis as the most obvious source of nonspecific reactions, and, thus, making the sample less representative of the target population. Secondly, the observation of a staggering amount of nonspecific reactions in Tanzania made it virtually impossible to disentangle the underlying prevalence of infection with M. tuberculosis in the test population from cross-reactions due to infection with environmental mycobacteria 20. Thirdly, the growing impact of HIV on tuberculosis morbidity 21 seemingly overpowered any reduction in transmission accomplished by the control programme.
The test population of children was chosen for their accessibility in schools, but also to obtain insight into recent transmission patterns more rapidly from a few serial surveys than would be readily feasible by choosing older population segments. Conversely, this selection has two additional disadvantages. First, the younger the test population, the lower the expected prevalence of infection and, thus, the poorer the predictive value of a positive test result. Secondly, the approach may show the impact of excess transmission arising from HIV-associated tuberculosis on the youngest population. It fails to inform about the potential of HIV infection to impact on tuberculosis, directly and indirectly, in the age groups at main risk of HIV infection. Nothing is known about the extent of those already infected or about those still at risk of becoming infected in these age groups that increasingly shape the dynamics of tuberculosis in many sub-Saharan countries 22–25.
In Kenya, a perceptible increase of infection among children has been observed in recent years, correlated with the prevalence of HIV infection among tuberculosis patients 26. Transmission from excess tuberculosis cases resulting from HIV infection may thus show up in children after some time, but the measure is crude and hinges significantly on the extent of social interaction between the generation with HIV infection and the children enrolled in a survey. The determination of the precise extent of excess transmission is further hampered by the previously mentioned extent of nonspecific tuberculin skin-test reactions.
Relating risk of infection to burden of disease
It had been proposed by Styblo 27 to study the relationship between disease incidence and infection risk, showing a constant relationship in the pre-chemotherapy era settings. This was expanded in a later study by Murray et al. 28. The weakness of the latter paper lies in its admission that there were actually some studies only on prevalence, and that the incidence was estimated by dividing the prevalence by two, a somewhat circular argumentation. If the risk of infection is driven by the incidence, then intervention with curative chemotherapy would be futile. The expected immediate impact of case finding and chemotherapy modifies the person-time of infectiousness in the community, and only indirectly modifies the incidence whereby the incidence in two populations might be the same, but the risk of infection may vary greatly depending on how long each incident case is allowed to transmit 29. Yet, despite the apparent flaw in argumentation, the erroneous notion that information about the risk of infection allows the estimation of disease incidence stubbornly persists, even in some prominent publications 30.
Addressing methodological shortcomings of tuberculin skin testing
Tuberculin skin testing dates back to the 19th century 31. Fifty years after Koch's development of Old Tuberculin, Seibert 32 produced a standardised tuberculin, which is now the international standard 33 against which all commercially available tuberculins should be tested 34. Globally, the most widely used tuberculin is PPD RT23 (Statens Serum Institut, Copenhagen, Denmark) 35. Specific guidelines on how to carry out a tuberculin skin-test survey are available 36, which should help to reduce technical errors.
The major obstacle to determining the prevalence of infection, and, thus, deriving the risk of infection, is related to the varying and unpredictable specificity of the tuberculin skin test in various settings 20. Specificity is driven by the frequency of nonspecific sensitisation to environmental mycobacteria, as well as the type, policy and extent of BCG vaccination. In such settings, it often becomes arbitrary to define a cut-off point that “balances” errors resulting from a lack of sensitivity against errors from a lack of specificity. Similarly, assuming a symmetric distribution around the true mean of the diameter of tuberculin skin-test reaction sizes from true tuberculous infection 36 becomes a doubtful undertaking 20. Estimation with such techniques is further hampered by often observed terminal-digit preference.
Terminal-digit preference refers to the readily observable fact that humans tend to exhibit preferences for certain digits, such as those ending in zero or five, or even numbers over odd numbers. This can create problems when cut-off points containing such digits are being used to determine the proportion of individuals who are infected with M. tuberculosis. The simplest way to correct some of these errors is to use a smoothing strategy, such as moving averages over two 37, or more adjacent indurations. A more convincing approach is to combine smoothing with penalised likelihood and the transfer of counts from preferred to nonpreferred digits 38, yet this is much more demanding both computationally and statistically. The model allows a quantification of digit preferences and a correction for them.
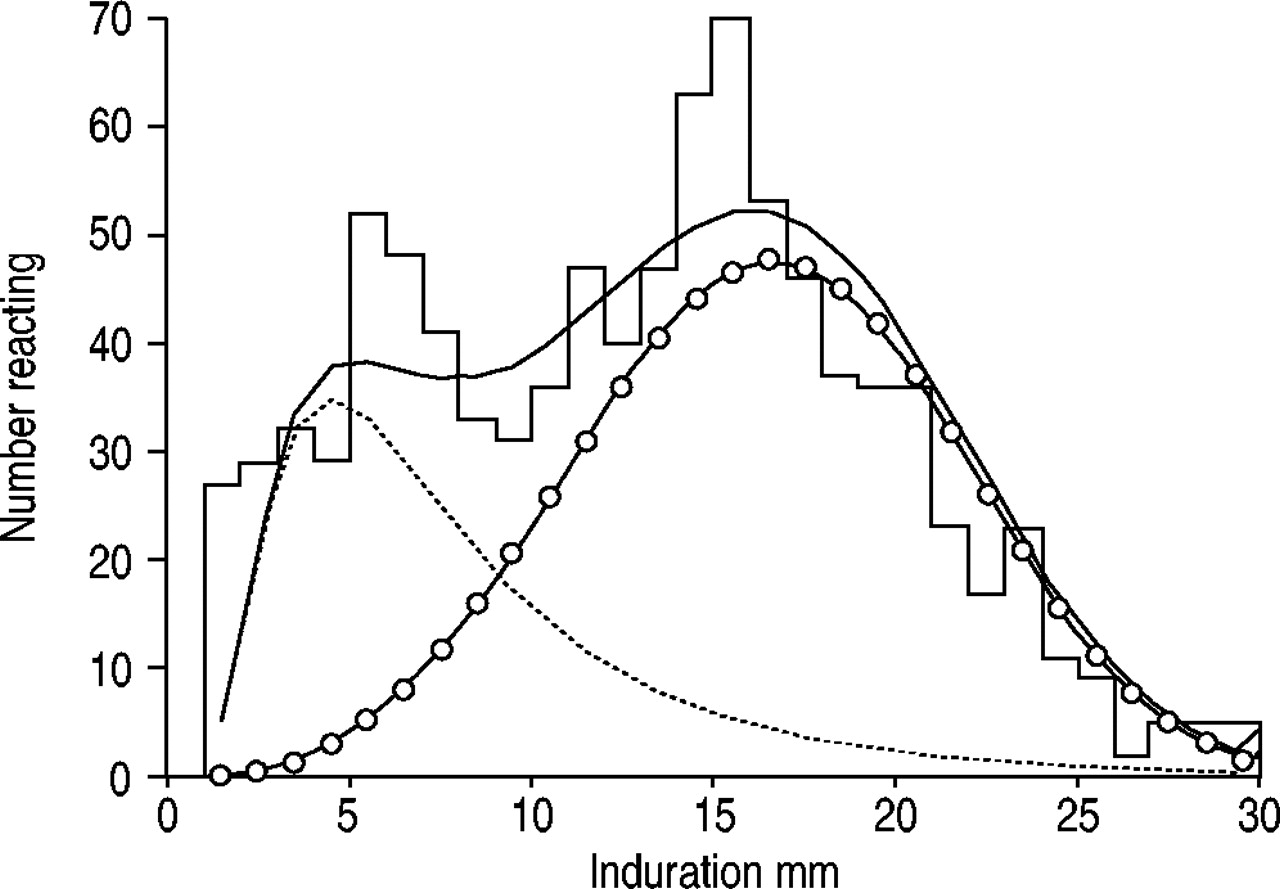
Models employing mixture analysis to estimate underlying distributions have been successfully used to estimate the prevalence of infection with M. tuberculosis both among BCG-unvaccinated subjects 39 and BCG-vaccinated subjects 40, albeit the experience is very limited. The basic assumption in mixture analysis of tuberculin skin-test surveys is that the observed distribution is the composite result of overlapping distributions attributable to infection with M. tuberculosis, a distribution resulting from infection with mycobacteria other than M. tuberculosis, and one arising among persons not infected with any mycobacterium. Mixture analysis estimates the parameters of the underlying distributions and seeks the distributions that best fit the observed 41. An example of the results of such an analysis with a reasonably good-fitting model is shown in figure 2⇓, utilising data from a large tuberculin skin-test survey conducted in southern India >40 yrs ago 42.
The most convincing approach might lie with the development of techniques that utilise M. tuberculosis-specific antigens that can neither be found in M. bovis-BCG nor in environmental mycobacteria. Some progress in this area is notable. Interferon-γ-release assays are aiding more or less in successfully overcoming the problem of nonspecific reactions attributable to BCG vaccination and infection with environmental mycobacteria 43–45. While it appears likely that this or similar types of techniques will ultimately overcome some of the shortcomings of tuberculin skin testing, they currently require venepuncture, which is acceptable in individual practice, but not in surveys among healthy children.
Risk of infection: what it can and cannot accomplish
Theoretically, the determination of changes in the risk of infection is the most informative indicator for changes in transmission patterns of M. tuberculosis in a community.
However, the technical, logistical and financial issues associated with the carrying out of representative tuberculin skin-test surveys might be a major impediment in many settings. Ethical issues also arise about the consequences of identifying children in a survey classified as being infected with M. tuberculosis. It is far from clear in which situation it is advisable to recommend preventive therapy for such children, and in which it is not only inefficient but also problematic because of the prevalence of liver disease in asymptomatic children who do not have access to determination of liver-enzyme levels 46.
The determination of the risk of infection will not allow estimation of disease incidence in a community. If carried out in children, it will also allow little insight on the impact that HIV may exert on a population. What a determination of the average annual risk of infection with Mycobacterium tuberculosis will provide if the infection prevalence can be determined successfully is to demonstrate the extent to which transmission to the youngest generation can be curtailed, a critical indicator for progress, or lack thereof, towards diminishing the tuberculosis problem in a community.
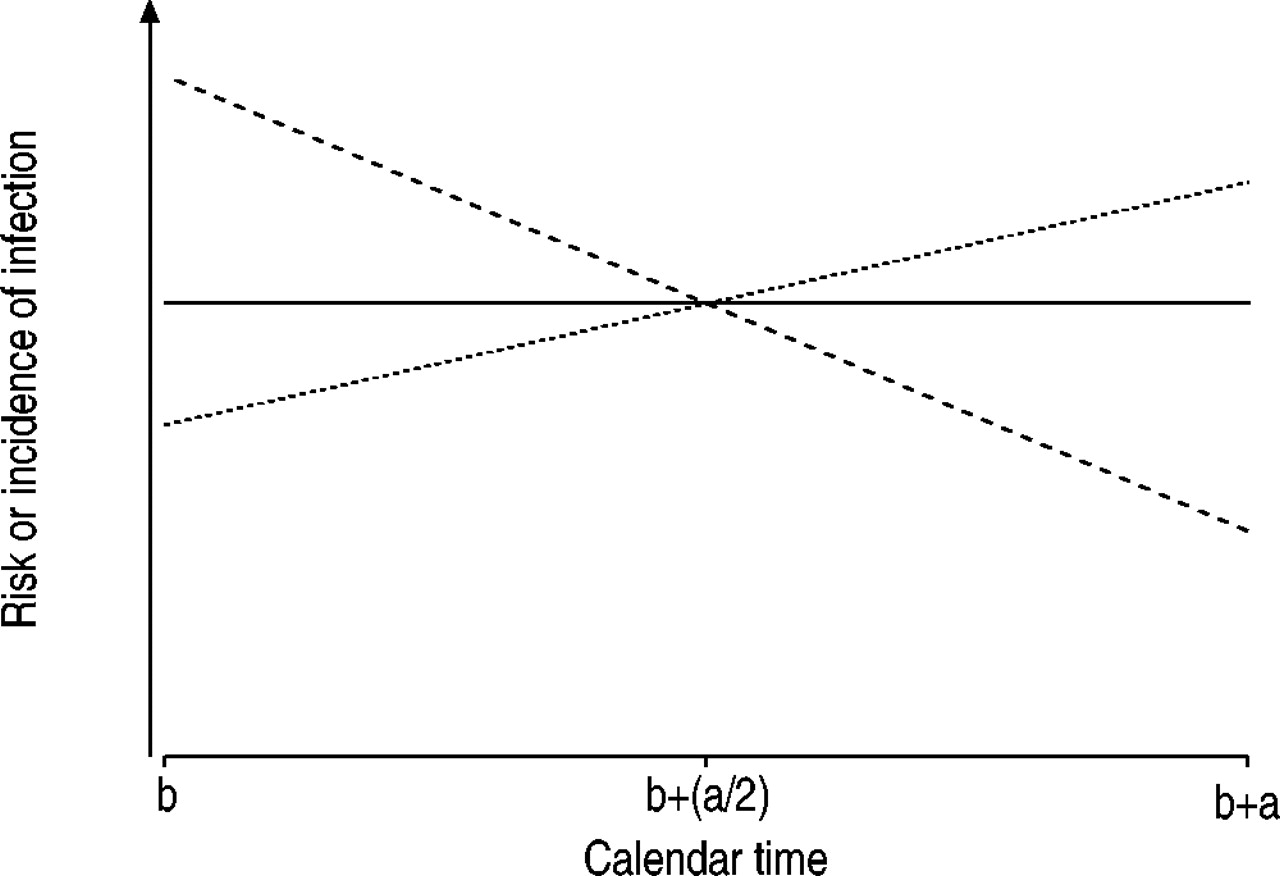
Schematic presentation of the course in the incidence and the calculated prevalence of infection with Mycobacterium tuberculosis, where b is the calendar time of birth and b+a is the calendar time when the birth cohort was evaluated. - - - -: incidence 1; ––––: calculated risk; ……: incidence 2.

{kind=link}
{kind=link}
Example of mixture analysis of the Tumkur survey 42 among 25–29-yr-old males showing observed induration sizes (histogram), the underlying distribution from infection with Mycobacterium tuberculosis (○), the underlying distribution from nonspecific cross-reactions (……), and the mixture distribution (––––). Reactors with 0-mm induration have been omitted for better display.
Footnotes
-
Previous articles in this series: No. 1: Cardona P-J, Ruiz-Manzano J. On the nature of Mycobacterium tuberculosis-latent bacilli. Eur Respir J 2004; 24: 1044–1051.
- Received September 4, 2004.
- Accepted September 15, 2004.
- © ERS Journals Ltd