



Bronchial reactions to the inhalation of high-dose tobramycin in cystic fibrosis
- W.H. Nikolaizik,
- K. Trociewicz and
- F. Ratjen
- W.H. Nikolaizik, Dept of Paediatrics, University Hospital Essen, Hufelandstr. 55, 45122, Essen, Germany. Fax: 49 2017235721. E‐mail: wilfried.nikolaizik@uni-essen.de
Abstract
It has been established that inhaled tobramycin has a positive effect on respiratory function in Pseudomonas-aeruginosa positive patients with cystic fibrosis (CF). In a previous study the authors reported that low-dose tobramycin preparations containing the preservative phenol caused significant bronchial obstruction. Recently, high-dose tobramycin preparations with and without preservatives/phenol have become available.
To assess the airway response to these preparations flow/volume curves in 12 patients with CF (four males, eight females, mean age±sd=19.0±7.4 yrs) were measured. The tobramycin preparations: Nebicina® 2.0 mL (150 mg, containing the preservative phenol), Distobram® 3.0 mL (150 mg, containing preservatives), Tobi® 5.0 mL (300 mg), Tobi® 2.5 mL (150 mg), and Tobi® 5.0 mL, were used after bronchodilator application.
Immediately and/or 5 min after the tobramycin inhalations there was a significant fall in lung function with the different preparations. There was no significant difference between preparations with and without preservatives/phenol. The bronchial obstruction was comparable to that observed after the inhalation of low-dose tobramycin and after saline. After 10 min of inhalation, the lung function returned to baseline values. Most patients preferred the Tobi® 2.5 mL and disliked the Nebicina® preparation due to the unpleasant taste. Preceding treatment with bronchodilators prevented the decline in lung function.
Assessment of bronchial response at the first nebulisation of high-dose tobramycin and, in case of significant obstruction, β‐agonists in combination with the antibiotic inhalation are recommended.
- bronchial response
- bronchodilator
- cystic fibrosis
- inhalation
- lung function
- tobramycin
The regular use of aerolised antibiotics can slow down the decline of respiratory function and reduce the frequency of hospitalisations in patients with cystic fibrosis (CF) 1, 2. However, some patients complain of bronchial irritation such as cough or tightness of the chest when inhaling tobramycin. Bronchial obstruction after inhalation of tobramycin at a conventional low dose as used in Europe (80 mg) was demonstrated in 12 CF patients with moderate disease status 3. However, the preparation used for testing contained sodium ethylenediamine tetraacetic acid (EDTA) and sodium metabisulphite as an antioxidant and phenol as a preservative therefore, it remained unclear if the bronchial obstruction occurred as a reaction to tobramycin or due to the antioxidant and preservative. Furthermore, a similar bronchial obstruction was shown after inhalation of isotonic saline. Isotonic saline had a higher osmolality (288 mmol·kg−1 versus 174–234 mmol·kg−1) and a lower pH (4.7 versus 5.3–6.3) compared with the tobramycin preparations 3. These data indicate that the inhaled drug might not necessarily be the major cause of bronchial constriction and that other factors need to be taken into consideration as well.
An earlier multicentre, crossover study demonstrated that a regimen of very high-dose aerolised tobramycin (600 mg, three-times daily) for up to 56 days was highly effective in improving lung function and reducing the density of Pseudomonas aeruginosa in sputum 4. However, this regimen was not well tolerated owing to the high volume of the preparation. In a multicentre, double-blind, placebo-controlled follow-up trial 520 CF patients received either 300 mg of inhaled preservative-free tobramycin or placebo, twice daily in three on-off cycles for a total of 24 weeks. At week 20 the patients on active treatment had a 12% increase in the forced expiratory volume in one second (FEV1), a decreased density of P. aeruginosa of 1.1 log10 colony forming unit·g−1 of expectorated sputum, and a 26% lower risk of hospitalisation compared with the placebo group 5. The immediate effect on lung function was only measured 30 min after inhalation of tobramycin, the fall in FEV1 at this time reached −2.0%, the same as the fall after a placebo consisting of 1.25 mg of quinine sulphate in 5 mL of one-quarter strength of saline. More detailed testing within the first 10 min after inhalation, as described in a previous study 3, has not been performed. Therefore it remains unclear if bronchospasm occurred immediately after inhalation of high-dose preservative-free tobramycin. The aim of this study was firstly to assess the bronchial reactions to the inhalation of high-dose tobramycin preparations and compare the results with the previous study with low-dose tobramycin. Secondly, the effect of preservatives and phenol was assessed by the inclusion of different tobramycin preparations. Thirdly, the protective effect of bronchodilators preceding the inhalation was measured.
Patients and methods
A total of 12 patients with CF (four males and eight females, mean age 19.0±7.4 yrs), were studied. Inclusion criteria were colonisation by P. aeruginosa for ≥6 months, regular inhalation treatment with tobramycin for ≥3 months, age 10–30 yrs, and a forced vital capacity (FVC) of 40–90% predicted values. Exclusion criteria were any change of inhaled medications 1 month prior to the study or during the study period, and a history of allergic bronchopulmonary aspergillosis. Approval from the local ethics committee was obtained before the start of the study. All patients were informed about the purpose of the study and gave their informed consent.
The patients included in the study inhaled one of the following preparations on six consecutive days at the same time of the day. On the first day the patients inhaled saline 0.55%, and on the following 4 days, either Nebicina® (Lilly, Sesto Fiorentino, Italy), Distobram® (Lilly, Lisbon, Portugal), Tobi® (Pulmopharm, Munich, Germany) 2.5 mL or Tobi® 5.0 mL in a randomised and balanced order. Saline was used at a concentration of 0.55% to adjust the osmolality to that of the tobramycin preparations. The tobramycin preparations were used as supplied by the manufacturer: Nebicina® 150 mg·2 mL−1 (containing 0.20 mg disodium EDTA and 2.88 mg sodium metabisulphite as an antioxidant, and 10 mg phenol as a preservative); Distobram® 150 mg·3 mL−1 (containing 0.30 mg disodium EDTA and 8.76 mg sodium metabisulphite as an antioxidant, no phenol); and Tobi® 300 mg·5 mL−1 (containing no antioxidant, no preservative). On the first 5 days inhalations were performed without preceding bronchodilatation, on day six the patients inhaled Tobi® 5 mL after bronchodilatation with four puffs of salbutamol (0.4 mg) via spacer. Using this design every single patient was able to complete the study within a week so that the day-to-day variability could be kept to a minmum. On the study days flow/volume curves including FVC, FEV1 and maximal expiratory flow at 50% of remaining FVC (MEF50) were measured before saline or tobramycin inhalations, immediately afterwards, and again 5 and 10 min afterwards. The results were expressed as percentage of predicted values according to Polgar and Promadhat 6 and Morris 7. A minimum of three forced expiratory manoeuvres were performed for every recording, and data used were from the best manoeuvres according to the guidelines of the American Thoracic Society 8, 9.
Every single patient included in the study inhaled saline and the different tobramycin preparations from the same Pari MasterTM compressor with an LL nebuliser via mouthpiece as supplied by the manufacturer (Labhardt AG, Starnberg, Germany). The manufacturer specifications were: total output of 0.55 g·min−1, median particle size generated 3.3 µm with 67% of particles <5 µm. The length of inhalation was recorded. Osmolality and pH of the nebulised solutions were measured in three cases in the reservoir container of the nebuliser at the beginning and the end of the saline and tobramycin inhalations. The patients were asked to score their subjective chest symptoms such as cough, tightness of the chest and dyspnoea by using a graded scale (0=no symptoms, 1=mild symptoms, 2=moderate symptoms, 3=severe symptoms). At the end of the study the patients were asked to rank their individual preferences of the different study inhalations.
Statistics
Statistics employed included the Wilcoxon signed-rank test and the Pearson's Chi-squared test with Yates' correction. Correlation coefficients were determined using Pearson's linear regression analysis. The coefficient of variation was determined as standard deviation divided by the sample mean. The sample size (12 patients) was based on the results of a previous study by the authors. A p<0.05 was considered to be significant.
Results
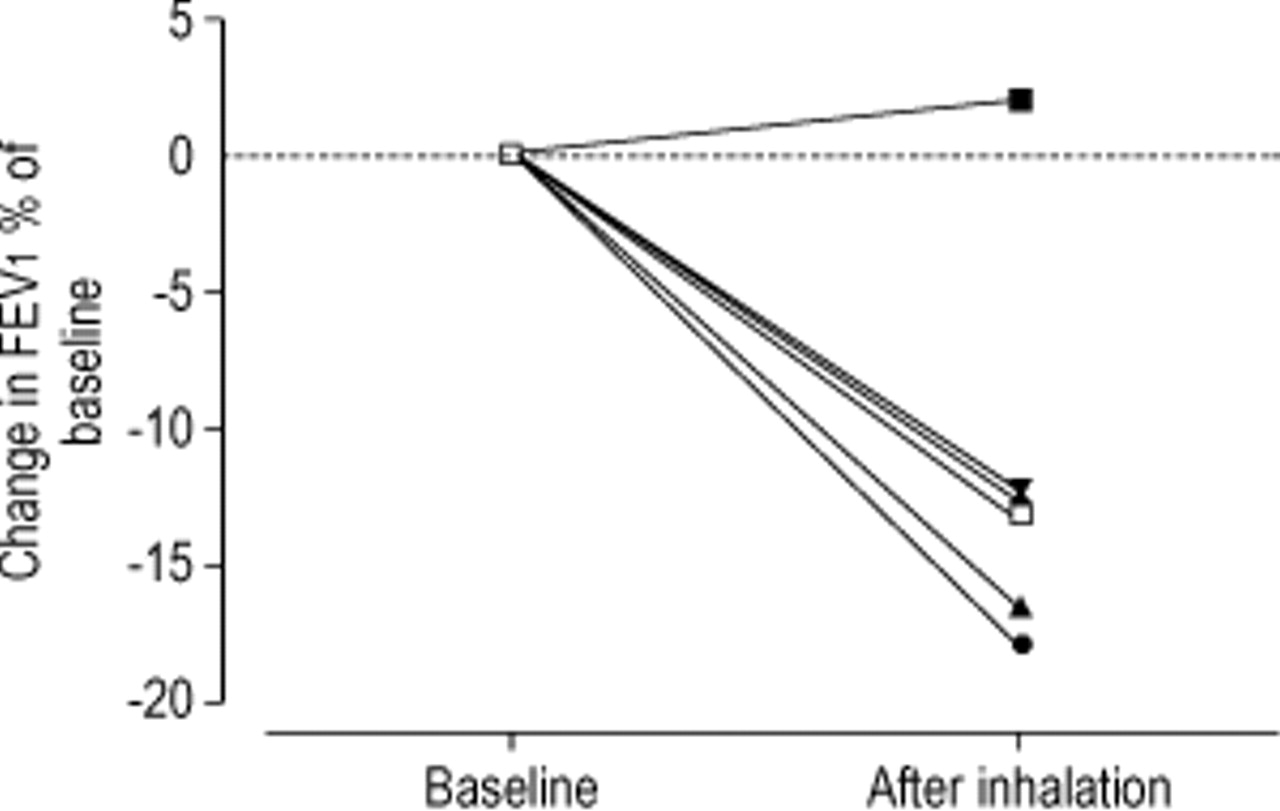
Table 1⇓ summarises the results of the lung function tests, and figure 1⇓ shows the percentage change from baseline in FEV1 after inhalation of the different tobramycin preparations and NaCl 0.55%. The vital capacity (VC) decreased significantly immediately and/or 5 min after the inhalation of Distobram® and Tobi® 2.5 mL. FEV1 fell significantly after Nebicina® and Tobi® 2.5 mL, as did peak expiratory (PEF) after Nebicina®, and MEF50 after Nebicina®, Distobram® and Tobi® 2.5 mL. Tobi® 5.0 mL caused a similar decrease in lung function although the difference did not reach statistical significance. There was a small drop in oxygen saturation, which did not reach statistical significance after either preparation. After 10 min of inhalation lung function tests had normalised. Placebo inhalations with saline 0.55% caused a significant fall of FEV1, PEF and MEF50, which was similar to that observed after the different tobramycin preparations. When the inhalation of Tobi® 5.0 mL was preceded by bronchodilation lung function remained stable. In fact there was even a small improvement in the three indices of bronchial obstruction, FEV1, PEF and MEF50.

{kind=link}
Mean change in the forced expiratory volume in one second (FEV1) immediately and/or 5 min after inhalation of the different tobramycin preparations and saline. □: NaCl; ▾: Distobram®; ▴: Nebicina®; ♦ Tobi® 150 mg; • Tobi® 300 mg; ▪: Tobi®+bronchodilator.
Lung function data
Five of the 12 patients were sensitised to at least one allergen assessed by a standard skin-prick test to house mite 1 and 2, birch and grass pollen, cat, dog, and horse danders, Aspergillus fumigatus, Alternaria and Cladosporium. The groups with and without allergies were not significantly different in their response to the tobramycin preparations and saline. Five of the 12 patients used inhaled corticosteroids at doses between 400–3,000 µg·day−1 (median 1,000 µg·day−1). The groups with and without inhaled corticosteroids were not significantly different in the response to the tobramycin preparations and saline. The bronchodilator response, which was defined as increase in FEV1 after the inhalation of salbutamol, ranged from 3–26% (median 9%). This increase in FEV1 was not significantly correlated with the change in lung function that was measured after the inhalation of tobramycin or saline.
The intra-individual variability of lung function was determined as day-to-day variation of the first five baseline lung function tests without preceeding bronchodilation. The coefficients of variation (%) were calculated as follows (mean±sd): VC: 5.2±5.1, FEV1: 6.9±3.5, PEF 19.1±12.7 and MEF50 19.8±11.0. To achieve lung function changes on a significance level of 5%, a change of more than twice this calculated coefficient of variation was required. The number of single patients reaching a significant fall in lung function is summarised in table 1⇑. A significant fall in VC was observed most frequently after NaCl 0.55%, Nebicina® and Tobi® 300 mg, a significant fall in FEV1 after Distobram®, a significant fall in PEF after Tobi® 300 mg, a significant fall in MEF50 after Nebicina® and Tobi® 300 mg, and a significant fall in oxygen saturation after Nebicina® and Distobram®. The differences in response to the different preparations were not statistically significant.
Only one patient had a significant fall in VC and FEV1 when the inhalation of Tobi® 300 mg was preceeded by bronchodilation, and no patient at all had a significant fall in oxygen saturation after the inhalation of Tobi® 150 mg and Tobi® 300 mg preceeded by bronchodilation.
The inhalation times (mean±sd) were: NaCl 0.55% (5.0 mL): 16.4±2.5 min; Nebicina® (2.0 mL): 8.1±2.6 min; Distobram® (3.0 mL): 10.4±2.7 min; Tobi® 150 mg (2.5 mL): 9.4±3.3 min; Tobi® 300 mg (5.0 mL): 20.2±3.6 min; and for Tobi® 300 mg (5.0 mL) with preceding bronchodilation: 18.0±2.8 min.
At the beginning of the inhalations the median osmolality was: 182 mmol·kg−1 for saline 0.55%, 197 mmol·kg−1 for Nebicina®, 127 mmol·kg−1 for Distobram®, 179 mmol·kg−1 for Tobi® 150 mg (2.5 mL), and 180 mmol·kg−1 for Tobi® 300 mg (5.0 mL). The pH was: 4.8 for saline 0.55%, 6.2 for Nebicina® and Distobram, and 6.4 for Tobi® 150 mg (2.5 mL) and Tobi® 300 mg (5.0 mL). At the end of the inhalations there was an increase in osmolality except for Nebicina® reaching 217 mmol·kg−1 for saline 0.55%, 184 mmol·kg−1 for Nebicina®, 138 mmol·kg−1 for Distobram®, 199 mmol·kg−1 for Tobi® 150 mg (2.5 mL), and 206 mmol·kg−1 for Tobi® 300 mg (5.0 mL). The pH at the end of the inhalation was determined as 5.0 for saline 0.55%, and 6.4 for Nebicina®, Distobram®, Tobi® 150 mg (2.5 mL), and Tobi® 300 mg (5.0 mL).
The scores for cough, wheeze and dyspnoea and the individual preferences as reported by the patients are summarised in table 2⇓. Most cough was reported after NaCl 0.55%, Nebicina® and Distobram®, least cough after Tobi® 300 mg with preceding bronchodilatation. Most wheeze was reported after Nebicina®, and least wheeze after Distobram®. Most dyspnoea was reported after Nebicina® and Tobi® 300 mg, and least dyspnoea after Tobi® 150 mg. Overall, most patients preferred Tobi® 300 mg with preceding bronchodilatation and Tobi® 150 mg, and disliked Nebicina®. When NaCl 0.55% and Tobi® 300 mg with preceding bronchodilatation were not taken into consideration six patients preferred Tobi® 150 mg, four Distobram® and two Nebicina® while seven patients disliked Nebicina® most, three Tobi® 300 mg, and two Distobram®.
Scores for cough, wheeze and dyspnoea and the individual preferences of the 12 patients
Discussion
The inhalation of high-dose preparations of tobramycin caused significant bronchial obstruction in CF patients with moderate disease. These data confirm the results of the previous study with low-dose tobramycin inhalations 3. The degree of obstruction was similar in both studies. The tobramycin preparation used in the previous study contained sodium EDTA and sodium metabisulphate as antioxidants and phenol as preservatives. It was not clear whether the bronchial obstruction was caused by tobramycin or the antioxidants and preservatives. Therefore, preparations were used with and without antioxidants and preservatives in the current study. The differences between the preparations were only small indicating that the antioxidants and preservatives were not the major cause for the observed bronchial reactions. However, no long-term effects were investigated and a long-term deterioration cannot be excluded if preparations with antioxidants and preservatives are used.
In the previous study, the inhalation of isotonic saline caused a comparable obstruction as the inhalation of tobramycin indicated that the bronchial reaction was not directly caused by the different tobramycin preparations. The osmolality of isotonic saline was 288 mmol·kg−1 compared to 174–234 mmol·kg−1 for the different tobramycin preparations. The higher osmolality might also have been an explanation for the bronchial reactions after saline inhalation. For this reason saline at a concentration of 0.55% was used in the current study. The osmolality was adapted to that of the different high-dose tobramycin preparations. However, the same degree of obstruction was still observed. A possible explanation could be an asthmatic reaction. However, the groups with and without allergies were not significantly different in the response to the tobramycin preparations and saline. The same was applicable for the groups with and without inhaled steroids. In addition there was no correlation between the bronchodilator response and the degree of obstruction after inhalation with tobramycin or saline. This was in accordance with the data presented by Chua et al. 10, which demonstrated that airway obstruction after the inhalation of different antibiotics was not correlated with the bronchial reactivity. Another possible explanation might be the irritation of inhaled solutions inducing mucociliary clearance. In this case secretions obstructing the lumen of the small airways would cause bronchial reactions.
When only the different tobramycin preparations were taken into consideration the overall symptom score including cough, wheezing and dyspnoea was highest after the inhalation of Nebicina® and lowest after Tobi® 150 mg. Correspondingly most patients disliked Nebicina®, which was mainly due to the unpleasant taste of phenol. Conversely, most patients preferred the Tobi® 150 mg solution. Tobi® 300 mg had a slightly higher symptom score and was also ranked lower due to its longer inhalation time. The individual preferences can also effect the patients' compliance with treatment. It is likely that an unpleasant preparation might willingly be forgotten. For this reason the use of phenol-free tobramycin preparations might be favourable. The marketing prices per mg for each of the different preparations in Germany are the following: 0.09 E for Nebicina®, 0.14 E for Distobram®, and 0.20 E for Tobi®. Considering a daily treatment of either 150 mg b.i.d. continuously or 300 mg b.i.d. on alternate months the costs per year would be 9855 E for Nebicina®, 15330 E for Distobram®, and 21900 E for Tobi®.
In the previous study 3 as well as in an independent study from Canada 11 salbutamol significantly reduced the bronchial obstruction after the inhalation of low-dose tobramycin. These results were confirmed by the current study with high-dose tobramycin preparations. Since bronchial obstruction was not always realised by the patient 3, 11 the authors recommend that lung function tests should be performed at the first nebulisation with high-dose tobramycin. If lung function testing reveals significant bronchial reactions β‐agonists should be used in combination with the nebulisation of high-dose tobramycin preparations.
- Received June 25, 2001.
- Accepted January 31, 2002.
- © ERS Journals Ltd