



An 11-yr-old male with pneumonia and persistent airway obstruction
- 1Dept of Paediatric Pneumology and Immunology, 2Dept of Paidopathology and Placentology 3Dept of Paediatric Surgery, University Hospital Charité, Humboldt University, Berlin, Germany
- B. Niggemann, Dept of Paediatric Pneumology and Immunology, Children's Hospital Charité, Humboldt University, Augustenburger Platz 1, D‐13353, Berlin, Germany. Fax: 49 30450566931. E‐mail: bodo.niggemann@charite.de
- bronchus
- children
- lung carcinoma
- mucoepidermoid carcinoma
- Wilms-tumour
Case report
At the age of 4 yrs the male child suffered from a Wilms-tumour of the right kidney treated by polychemotherapy (SIOP No. 9 for stage 1 using actinomycin and vincristin) and surgical removal. A year later, abdominal pain occurred and a local relapse of the Wilms-tumour was diagnosed. Further diagnostics revealed infiltration into the liver, diaphragm, and the thoracic wall. In addition, three lung metastases were found. The child received polychemotherapy again (according to protocol SIOP 93/01 for stage 4 using adriamycin, etoposide, carboplatin, ifosphamide) and radiotherapy of the lung, abdomen (15 Gray) and of the tumour site (35 Gray). The tumour could be resected. All follow-ups during the next 6 yrs showed remission and the child was healthy.
At the age of 11 yrs, he presented with fever and cough. The chest radiograph showed an opacity of the left upper field (fig. 1⇓). Under the suspicion of pneumonia, antibiotic treatment was started. Due to bronchial obstruction, the child received low-dose inhaled steroids and β‐adrenergic agents. Nonetheless, he still suffered from bronchial obstruction and intermittent fever. Pulmonary function measurement revealed a mixed restrictive and obstructive ventilation disorder (forced vital capacity 52%, forced expiratory volume in one second 49% and flow at 25% vital capacity 13% predicted). Computed tomography (CT) scan of the thorax (including radio-opaque material) was performed (fig. 2⇓).

Chest radiograph showing an opacity of the left upper field.

Computed tomography scan at tracheal level.
For further diagnosis flexible bronchoscopy was performed, revealing a ball-shaped, soft, solid tumour deriving from the left upper lobe bronchus and bulging into the ostium of the left main bronchus (fig. 3⇓). In order to obtain a thorough diagnosis of the tumour, thoracic surgical intervention was performed. The histology of the tumour revealed typical findings (fig. 4⇓).

Flexible bronchoscopy revealed a ball-shaped soft solid tumour deriving from the left upper lobe bronchus and bulging into the ostium of the right main bronchus.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
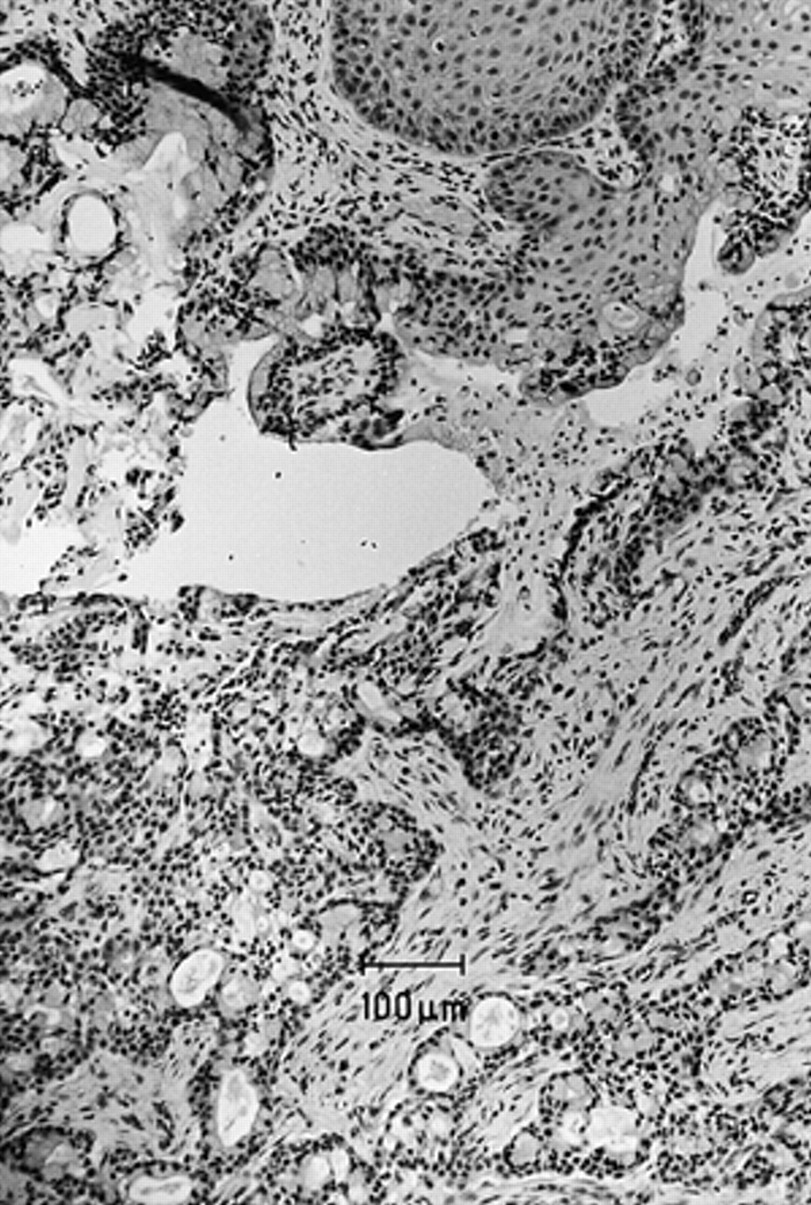
Histology of the tumour (haematoxylin and eosin staining).
BEFORE TURNING THE PAGE, INTERPRET THE CT SCAN (FIG. 2⇑) AND THE HISTOLOGY OF THE TUMOUR, AND SUGGEST A DIAGNOSIS.
Interpretations
The CT-scan (fig. 2⇑) showed an opaque left anterior upper lobe segment and positive air bronchogram, indicating an atelectasis. The histological work-up (fig. 4⇑) showed a tumour composed of intermediate to high-grade squamous cells forming nests, and mucin-containing glands. There were few mitotic figures and mild nuclear atypia.
Diagnosis: “Mucoepidermoid carcinoma of the left main bronchus, possibly as secondary malignancy in a male child with a history of a Wilms-tumour”
Successful lobectomy of the left upper lobe and sleeve resection of the upper lobe bronchus led to in toto resection of the tumour. The postoperative course was completely uneventful. The child was in excellent condition and lung function gradually normalized.
Discussion
Mucoepidermoid carcinoma (MEC) of the lung (formerly called bronchial adenoma) is a rare tumour, especially in children 1–3. The youngest patients reported were aged 3 4 and 4 yrs 5, 6. The tumour was believed to arise from excretory ducts of submucosal bronchial glands with a common origin of the salivary glands 7. A recent cytogenetic study indicates that the t(11;19) may be associated with the mucoepidermoid phenotype 8.
Mucoepidermoid tumours of the lung are usually located in the main or segmental bronchi 2, 4, 6, 8, 9, with some cases occurring in central airways such as the trachea 7, 10 or carina 1. Histologically, MEC are classified as low-grade to high-grade carcinomas. Surgical resection is the treatment of choice, using complete excision, lobectomy and/or sleeve resection 11–13.
Children are usually diagnosed following recurrent pneumonias 8, 9, 14–16, persistent cough 1, 9, 11, and/or wheezing (not responding to bronchodilator therapy) 4, 7, 8, 11, 17. Some younger children may be misdiagnosed as new-onset asthma 10. Other children present with atelectasis by complete or partial airway obstruction or with unilateral hyperlucent lungs 14, 17. MEC infrequently presents with haemoptysis 16.
In this case, intensive polychemo- and radiotherapy for relapse of the Wilms-tumour may have predisposed for developing secondary malignancy. Usually MECs are regarded as primary pulmonary tumours 18. The present case may therefore be the first of an MEC presenting as a secondary malignancy in a child.
Fortunately, low-grade malignant tumours are much more common than high-grade ones 19. Children, especially have an excellent prognosis if low-grade tumours can be resected completely. Therefore, in cases of unclear obstructive symptoms or recurrent pneumonias, a chest radiograph should be used to readily identify suspicious signs followed by further diagnostic steps including bronchoscopy.
- Received August 13, 2001.
- Accepted October 3, 2001.
- © ERS Journals Ltd