



The SleepStripTM: an apnoea screener for the early detection of sleep apnoea syndrome
- 1Scientific Laboratory Products, Ltd., Tel Aviv, Israel. 2Sleep Laboratory CHU A.Vésale, Free University of Brussels, Montigny-le-Tilleul, Belgium. 3Med. Poliklinik of Philipps University, Marburg, Germany. 4Sleep Laboratory, Technion-Israel Institute of Technology, Haifa, Israel
- P. Lavie, Sleep Lab, Gutwirth Building, Technion City, Haifa, Israel, 32000. Fax: 972 48323045
Abstract
Sleep apnoea syndrome (SAS) is a largely undiagnosed and prevalent disorder. It is associated with cardiovascular morbidity as well as excessive daytime sleepiness and poor quality of life. In the present study the SleepStripTM, a novel screening device is introduced, which is low cost and easy to use and is aimed for widespread use.
The results of three independent validation studies, which compared the SleepStripTM score (Sscore) against “gold standard” polysomnographically-determined apnoea/hypopnoea index (AHI), are reported both separately and combined. Four hundred and two patients suspected of SAS underwent full polysomnography recordings concomitantly with the use of the SleepStripTM.
For all samples combined, the correlation between AHI and Sscore was r=0.73, sensitivity and specificity values ranged from 80–86% and 57–86% respectively, and the area under the curve derived from receiver-operating characteristic curves ranged from 0.81–0.92 at varying AHI thresholds.
Though not intended as a substitute for polysomnography, the SleepStripTM may provide initial screening information, which may be useful in both clinical and experimental settings.
- apnoeas
- hypopnoeas
- received-operator characteristic curves
- screening
- SleepStrip
Conflict of interest: P. Lavie is the scientific advisor to the company manufacturing the SleepStrip. N. Hadas is the company's R&D manager. T. Shochat is the Clinical Trials Director of the company. P. Lavie and N. Hadas are both shareholders in the company.
Sleep apnoea syndrome (SAS) is a common sleep disorder affecting 2% of females and 4% of males in the adult population 1. However, it is estimated that the vast majority of patients remain undiagnosed. Based on a sample of nearly 5,000 working adults aged 30–60 who were medically insured, Young et al. 2 have reported that 93% of females and 82% of males with moderate to severe SAS remained undiagnosed. SAS is associated with increased cardiovascular morbidity, including systemic and pulmonary hypertension 3–6, cardiac arrhythmias 7 and ischaemic heart disease 8, 9. Studies have shown increased mortality of SAS patients, mainly from cardiovascular causes 10, 11. Furthermore, studies have shown that SAS patients with excessive daytime sleepiness are prone to motor- and work-related accidents 12, 13.
The “gold standard” for diagnosing SAS is a full night polysomnographic (PSG) recording, based on which the apnoea index (AI) or the apnoea/hypopnoea index (AHI) is computed.
Due to the limited numbers of recording beds and the lack of awareness among family and primary care physicians, many patients may be delayed in receiving treatment or remain untreated. The high costs and long waiting lists for overnight PSG recordings in the sleep clinics also contribute to this situation. Elderly and/or sick patients may find the PSG equipment too cumbersome, and may be reluctant to spend the night in the sleep laboratory.
Ambulatory sleep monitoring techniques do not provide an adequate solution for the need to screen large populations for sleep apnoea. In many cases where the attendance of a technician is required, the cost associated with home monitoring is not much different than the cost of laboratory recordings. As yet, there is insufficient experience and lack of validation of unattended monitoring systems, which might considerably reduce the cost of PSG recordings.
Sleep questionnaires are widely used as a first-line screening procedure to identify high-risk sleep apnoea populations. Chesson et al. 14 reviewed several predictive equations and questionnaires designed to determine the probability of SAS prior to PSG recordings. These pretest methods were usually self-administered, and focused on factors such as observed apnoeas, snoring, age, gender, body mass index (BMI), etc. In general, for high probability assignment (≥70%), these tests yielded low sensitivity values (∼30–40%), leaving the majority of severe apnoea patients unidentified.
With the growing need for a reliable objective tool for the early detection of SAS, an efficient, low cost, disposable sleep apnoea screener was developed (SleepStripTM, S.L.P. Ltd., Israel). The device is designed to aid sleep specialists or other physicians in the initial assessment of patients with suspected SAS. The apnoea screener enables physicians to confirm or reject the suspicion of apnoea, as well as determine the severity of the condition. This in turn may help prioritize patients, so that those in greatest need of treatment will undergo full PSG recordings in a timely manner, while those without apnoea will be able to avoid this somewhat tedious procedure.
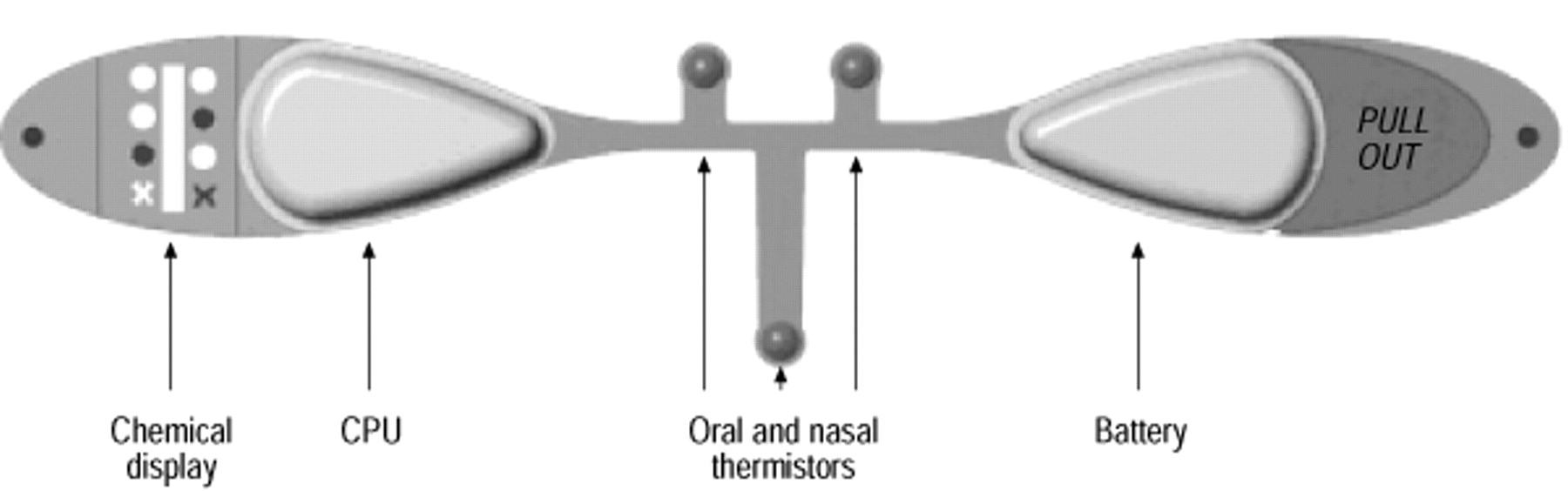
The SleepStripTM is a small, lightweight device worn underneath the nose and above the upper lip (fig. 1⇓). Patients are instructed to wear it just prior to bedtime and for at least 5 consecutive hours of sleep in their normal home environment.
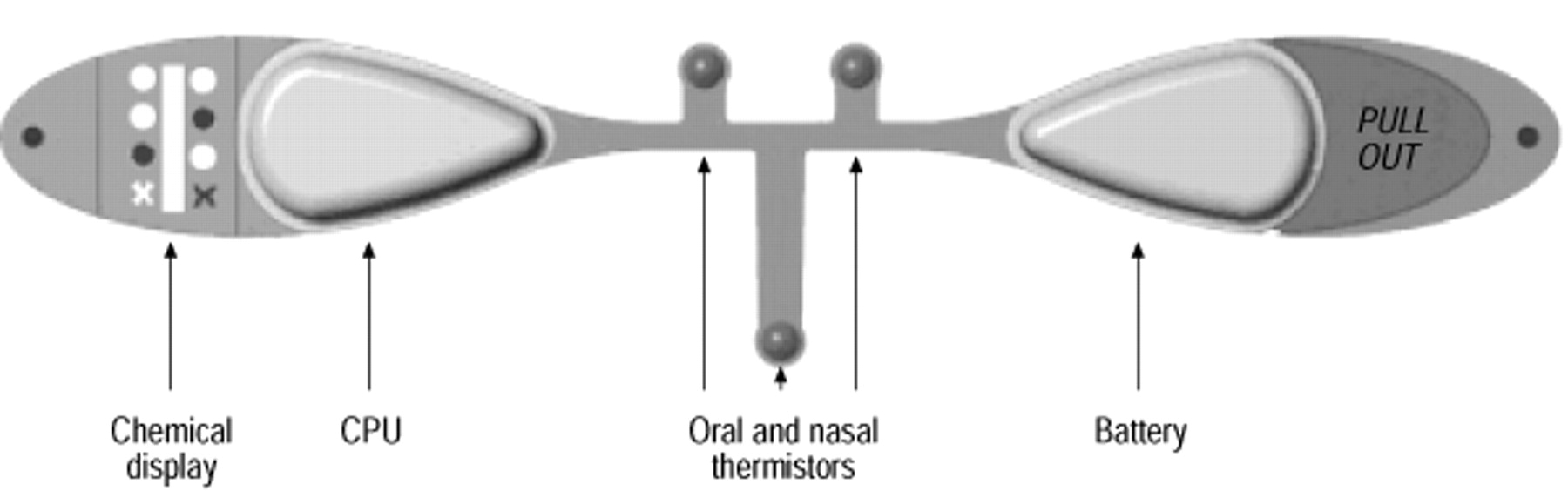
Schematic picture of the SleepStripTM. CPU: Central processing unit.
The device comprises flow sensors (oral and nasal thermistors), real-time analysis hardware and software, and a miniature display unit. A decrease or complete cessation of respiration is identified and counted throughout the night, following a 20-min calibration period. After at least 5 hours of recording, the SleepStripTM score (Sscore), which represents the number of respiratory events per hour of recording is computed and displayed.
In the present multi-centre study, the performance of the SleepStripTM in detecting respiratory events and establishing an Sscore was compared to the AHI obtained by standard PSG recordings in the sleep laboratory.
Subjects and methods
Patients
This study combined the data of three validation studies performed independently in sleep clinics in Israel, Germany and Belgium. Each clinic received approval from their respective local ethical committee for research on human subjects. Four hundred and two patients participated. Three hundred and three were from Israel, 50 from Belgium and 49 from Germany. All were suspected of having sleep apnoea, and underwent full overnight PSG monitoring in the sleep clinic concomitantly with the use of the SleepStripTM. Age ranged between 18–86 yrs, BMITM ranged between 18–59 kg·m−2.
Procedure
Conventional PSG recordings included monitoring of respiration using respiratory effort belts around the chest, oronasal temperature to assess respiratory flow, oxygen saturation and percentage of sleep-time with oxygen saturation <90%. Respiratory disturbances included apnoeas, defined as cessation in airflow ≥10 s, and hypopnoeas, defined as a reduction in the amplitude of the respiratory signal of at least 50% for ≥10 s, followed by either a decrease in oxygen saturation of 4%, or signs of physiological arousal. Based on these measurements, AHI and lowest nocturnal oxygen saturation were determined.
In order to determine the reliability of the SleepStripTM as an apnoea/hypopnoea screener, the device was attached above the upper lip as described before, in addition to the conventional thermistors used for PSG monitoring. Preliminary testing revealed that positioning of the SleepStripTM next to conventional thermistors did not interfere with their operation. Patients were requested to wear the device for at least 5 h post-calibration (at least 5-h of sleep after the 20-min calibration period) to allow for collection of sufficient data. Failure to maintain the device in place for the full 5-h period was consequently indicated on the chemical display. Although a score was computed, its validity may be questionable. Therefore, all devices worn for less than the required 5-h period were excluded from analysis.
Data management
Experienced scorers in each of the three laboratories scored PSG recordings using standard criteria 15 and established AHI. Automatically derived Sscores from SleepStripTM displays were collected.
Data analysis
Pearson correlations were performed between the SleepStripTM Sscores and PSG determined AHIs. The Sscore was tested separately against three AHI cut-off points, representing three levels of SAS severity, i.e. mild (>10), moderate (>20) and severe (>40). Since the Sscores are considered to be roughly equivalent to the AHI, sensitivity and specificity values of the Sscores were computed respectively for three Sscore thresholds, again representing mild, moderate and severe levels of SAS (>10, >20, >40). These analyses were done for each country separately and for the entire sample combined. The analysis of diagnostic accuracy of the SleepStripTM was based on receiver-operator characteristic (ROC) curves 16. This analysis was performed only for the entire sample. Accuracy was considered with respect to the “gold standard”, i.e., the AHI values, again using three levels of severity (AHI >10, >20, >40).
Results
Results from 288 patients (72%) were available for analysis (205 from Israel, 39 from Belgium and 44 from Germany). Data from 88 cases (22%) were discarded due to insufficient sleep (<5 h), data from 31 cases (8%) were discarded due to technical malfunction of the SleepStripTM (11 cases had both insufficient sleep and technical malfunction) and data of six cases (1.5%) were missing.
SleepStripTM score and apnoea/hypopnoea index
Table 1⇓ shows the correlations between AHI and Sscores for each country and for the three samples combined. The overall correlation was r=0.73 (p<0.001). Sensitivity and specificity values of the SleepStripTM for identifying patients with different AHI thresholds for each country separately, and for all samples combined, are presented in table 2⇓. Sensitivity and specificity values ranged between 0.85–0.88 and 0.52–0.91, respectively, for a threshold >10; 0.70–0.85 and 0.65–0.86, respectively, for a threshold >20; and 0.75–0.88 and 0.81–0.94, respectively, for a threshold >40.
Pearson correlations between the SleepStripTM score and Apnoea/hypopnoea index (AHI)
Sensitivity and specificity values for each country separately and for all samples combined
Accuracy analysis
ROC curves for the entire sample at three AHI thresholds are plotted in fig. 2⇓. The area under the curve (AUC) for an AHI>10 was 0.81 (p<0.001, confidence interval (CI) 0.76–0.86); AUCs for AHIs >20 and >40 were 0.84 (p<0.001, CI 0.79–0.89) and 0.92 (p<0.001, CI 0.89–0.96), respectively.

Receiver operating characteristic curve showing the sensitivity/specificity of each of the observed values of the SleepStripTM score in relation to an apnoea/hypopnoea index cutoff point of: a) 10 (area under the curve (AUC)=0.81); b) 20 (AUC=0.84); and c) 40 (AUC=0.92).
Figure 3⇓ shows a Bland-Altman plot of the relationship between the difference between the AHI and the Sscore versus their mean values. As can be seen, there is a bias of −5.8 events (95% CI −8–−3.6 events) indicating a small overestimation of the severity of the apnoea by the SleepStripTM.

{kind=link}
{kind=link}
{kind=link}
Bland-Altman plot of the relationship between the difference between the apnoea/hypopnoea index (AHI) and the SleepStripTM score (Sscore) versus their mean value. Mean bias (—), +2sd (····) and −2sd (- - - -) lines are shown.
Discussion
In the present study, the SleepStripTM, a novel, objective apnoea screener was introduced, and its validity in detecting SAS against overnight PSG recordings was challenged, in patients suspected of SAS examined in three different countries.
In a large meta-analysis, Ross et al. 17 reviewed the literature for various screening and diagnostic methods developed for the detection of sleep apnoea. Seventy-one studies, which assessed sensitivity and specificity values using PSG as the “gold standard”, were reported. These methods included portable devices, partial channel PSG, oximetry, partial time PSG, predictive equations, and other miscellaneous methods such as questionnaires, ear, nose and throat examination, flow volume loops and general impression by clinicians.
Twenty-five studies of portable devices were reported. Only two of these were done in patients' homes, the rest were done under supervision in the sleep laboratory. Sensitivity values ranged from 78–100% and specificity values ranged from 62–100%. Issues related to unattended home-monitoring such as reliability, equipment failure rates, compliance, prices and safety were rarely reported.
Other screening methods were also assessed. Twelve oximetry studies yielded moderate results, with sensitivity values ranged from 36–100% and specificity values ranged from 23–99%. Only two of these studies were done at home, the others were done under full laboratory supervision. Three studies of partial PSG, recording oximetry, airflow and thoracoabdominal movement, showed good diagnostic accuracy, with sensitivity values ranged from 82–94%, and specificity values ranged from 82–100%. Seven studies assessed partial time PSG during the night or day. The night-time studies reported sensitivity values ranged from 42–93%, and specificity values ranged from 70–100%; the daytime studies reported sensitivity values ranged from 66–100% and specificity values ranged from 50–100%, using various thresholds of AI/AHI. Four studies of flow volume loops reported sensitivity ranged from 41–59% and specificity ranged from 54–85%. Global clinical impressions yielded sensitivity values ranged from 52–79%, and specificity values ranged from 50–100%.
Both portable devices and the SleepStripTM are intended for home use. In comparison with the SleepStripTM, some of the portable devices have shown higher sensitivity and specificity values. This is most likely due to the additional channels of information available on these systems. However, as the majority of these studies were conducted in the supervised laboratory setting, these performance levels are likely to decrease substantially in unattended studies, as technical malfunctions and compliance issues come into play. Performance of the SleepStripTM may also decrease during unattended home monitoring, despite its simple and easy-to-use design. The present authors are currently conducting a study, which examines the reliability and performance level of the device in domiciliary use. Initial results on 28 patients indicate a correlation of r=0.66 (p<0.01) for all technically valid tests (n=24). However, one third of these had either removed or dislocated the strip during the night. Exclusion of this group resulted in a correlation of r=0.80 (p<0.001). Thus, physicians must ensure that patients fully understand and comply with the instructions for use.
Overall, the SleepStrip study results were generally more accurate than the results of studies using predictive equations and questionnaires, flow volume loops and clinical impressions, as well as some oximetry studies. SleepStrip results are comparable to those of portable devices and partial time PSG, and are slightly lower than those of partial PSG, which have been recommended as prescreening tests or replacements for full PSG 17.
The use of ROC curves to establish the accuracy of a new diagnostic technique against a traditional technique is applied here to the SleepStripTM. While computing sensitivity and specificity at specific thresholds may give some information on the accuracy of a new technique, this information may be misleading, as it applies to only small and isolated parts of the puzzle. ROC curves give an overall estimate to the quality of the information obtained by the new technique across all possible sensitivities and specificities obtained by varying the threshold used. The closer the curve reaches the upper left-hand corner of the graph, the larger the AUC and the higher the quality and accuracy of the information obtained. It is then possible to go back to the coordinates of the curve in order to find the optimal trade-off between sensitivity and specificity desired for the purposes of the test.
Overall accuracy of the SleepStripTM based on the ROC curves was high, with increased accuracy in screening SAS in the higher severity levels. Nevertheless, the scatter of the datapoints around the mean value of the bias shows that in many cases the SleepStripTM may significantly over- or under-estimate the true AHI.
Finally, the authors should emphasize that the SleepStripTM is not intended to replace full PSG for the diagnosis of SAS. Its purpose is to allow large-scale initial screening for SAS with relatively low cost and effort. This may be applied both in clinical practice and for research purposes.
In clinical practice, the SleepStripTM may be particularly useful for early screening of patients with risk factors for SAS such as obesity, snoring, hypertension, or family history. The importance of screening for SAS even in the absence of complaints of disturbed sleep and hypersomnolence was demonstrated in a large cross-sectional study (the Sleep Heart Health Study) on the association between SAS and cardiovascular disease (CVD). Shahar et al. 18 reported that even ranges of apnoea which are considered normal (AHI ≤10) were associated with mild to moderate CVD. No associations were found between sleep fragmentation and either apnoea indices, or CVD. Thus, early detection of SAS in asymptomatic individuals might be critical in preventing cardiovascular sequelae. In a recent editorial, Hedner and Grote 19 pointed out that the need to screen large high-risk populations who are asymptomatic for SAS warrants “simple and reliable diagnostic tools”, as well as the promotion of awareness and education. The SleepStripTM may be an excellent tool for implementing such a strategy.
Furthermore, patients with medical conditions which frequently coexist with SAS, such as ischaemic heart disease, chronic obstructive pulmonary disease and end stage renal disease, may find the SleepStripTM particularly appealing, as it can be used in the comfort of their home. Early diagnosis and treatment in such clinical populations may improve both management strategies and quality of life.
To date, most cross-sectional prevalence studies as well as longitudinal follow-up studies on sleep apnoea syndrome relied on either subjective questionnaire-based data and large sample sizes, or objective polysomnographic based data and small sample sizes. The SleepStripTM may enable studies with larger samples based on objective evidence for sleep apnoea syndrome to be carried out. Such studies may give better estimates of the prevalence of sleep apnoea syndrome in specific clinical populations and in the population at large, as well as long-term evaluation of developing comorbidity and treatment outcomes.
- Received March 23, 2001.
- Accepted August 2, 2001.
- © ERS Journals Ltd