



A new asthma severity index: a predictor of near-fatal asthma?
- P. Lee,
- J. Abisheganaden,
- C.B.E. Chee and
- Y.T. Wang
- J. Abisheganaden, Dept of Respiratory Medicine, Tan Tock Seng Hospital, 11 Jalan Tan Tock Seng, Singapore, 308433. Fax: 65 3577871
Abstract
Bronchial hyperresponsiveness (BHR), measured as the provocative dose of inhaled histamine or methacholine required to produce a 20% fall in forced expiratory volume in one second (FEV1) (PD20), is widely used as one of the indices of asthma severity. Excessive bronchoconstriction, reflected by the maximal percentage fall in forced vital capacity (FVC) at PD20 (ΔFVC %) during BHR testing, is considered to be the most important pathophysiological determinant in fatal asthma. The present study hypothesized that an index which combines both the ease of airway narrowing and excessive bronchoconstriction, ΔFVC %/log(PD20), may be better in assessing asthma severity, especially in those at risk of near-fatal attacks.
The dose-response curves of 46 asthmatics who underwent methacholine challenge testing were studied. Group 1 (n=14) patients had mild disease, Group 2 (n=21) had moderate disease and Group 3 (n=11) had severe disease, as classified according to the Global Initiative for Asthma. Nine patients had prior intubation for near-fatal asthma.
ΔFVC %/log (PD20) was better than ΔFVC % and PD20 in categorizing patients into the three severity groups (p<0.0001), but more importantly, it was able to discriminate patients with previous intubation from those without (p=0.04). It also correlated better with FEV1 (% predicted), frequency of symptoms and inhaled steroid requirement than either index alone.
It is concluded that the percentage fall in forced vital capacity/log of the provocative dose causing a 20% fall in forced expiratory volume in one second combines information on the ease and excessive degrees of airway narrowing in asthma. This new index may be better at assessing asthma severity and in discriminating those at risk of near-fatal attacks.
- Excessive bronchoconstriction
- intubation
- near-fatal asthma
Bronchial hyperresponsiveness (BHR), measured as the provocation concentration (PC20) or dose (PD20) of inhaled histamine or methacholine required to produce a 20% fall in forced expiratory volume in one second (FEV1), is widely used as a diagnostic test for bronchial asthma as well as an index of asthma severity 1–3. However, the use of BHR as an index of asthma severity has been questioned following prospective studies, that have shown poor correlation between PD20 and risks for clinical exacerbation 4–6 as well as in the detection of those at risk of fatal attacks 7–9.
At present there is increasing evidence that airway hyperresponsiveness implies more than just hypersensitivity. Woolcock et al. 10 found that the histamine dose-response curves of asthmatics differed from normal subjects by their position, slope and maximal response. Apart from a shift to the left, asthmatics have steeper slopes and higher maximal responses 10–11. This implies that airway narrowing is characterized by at least two abnormalities: a leftward shift of the dose-response curve (ease of airway narrowing) and an upward displacement of the maximal response (excessive bronchoconstriction). The PD20 (or PC20) is a single point in the dose-response curve which reflects the ease of airway narrowing, while the level of maximal response reflects the propensity for airway closure. This propensity for airway closure is not obtained during routine BHR testing due to the inherent risks of provoking an excessive fall in FEV1.
Recently, Gibbons et al. 12 proposed a novel, indirect method for the detection of excessive bronchoconstriction in patients with mild asthma. They found that excessive bronchoconstriction, as measured by the maximal percentage fall in forced vital capacity (FVC) at PD20 (ΔFVC %) during BHR testing, significantly correlated with the number of prescriptions per month for oral corticosteroids. They concluded that ΔFVC % might be useful in detecting the asthmatic at risk for serious disease 12. A previous study has validated their findings and has shown that ΔFVC % correlated with the dose of inhaled corticosteroid 13. However, ΔFVC % did not correlate with the frequency of asthma symptoms, spirometry or PD20.
Therefore it has been hypothesized that a new index, which combines both the ease of airway narrowing and excessive bronchoconstriction, ΔFVC %/log(PD20), may be better in assessing asthma severity especially in those at risk of near-fatal attacks. The objectives of the present study were to determine if the new index correlated with symptoms, spirometry, steroid usage, eosinophil count, immunoglobulin-E (IgE) and serum eosinophilic cationic protein (ECP) better than either index alone, and more importantly, if the new index was able to identify patients at risk of near-fatal asthma exacerbation.
Materials and methods
Study design
Forty-six adults with symptoms of asthma and documented airway reversibility or positive methacholine challenge tests (MCT) were recruited from the respiratory outpatient clinic of Tan Tock Seng Hospital from February–April 2000. These patients were stable for the previous 4 weeks, with no change in their medications, and had no recent respiratory tract infection or hospitalization for asthma. Smokers, pregnant subjects and those with FEV1 <60% predicted were excluded. Near-fatal asthma was defined as severe exacerbation, which resulted in intubation and mechanical ventilation and this was determined from case-record review.
All subjects underwent routine history and physical examinations. All had baseline spirometry testing and were asked to record: 1) their symptoms using a four-point rating scale, 2) morning (07:00–08:00 h) and evening (19:00–20:00 h) peak expiratory flow (PEF) values measured with mini-Wright peak flow meters before medications and 3) daily medication requirement in their diary cards for 2 weeks. They were classified into mild, moderate and severe groups according to a modified Global Initiative for Asthma (GINA) protocol (table 1⇓) and were advised to omit inhaled and oral medications 24 h before MCT.
Classification of asthma severity (modified Global Initiative for Asthma)
The MCT was performed at the same time of the day using the standard protocol described by Yan et al. 14. Aerosols of physiological saline and methacholine were generated by a dosimeter system (MEFAR ‘MB3‘, Bovezzo, Italy) to give an output of 0.15 mL·min−1 of aerosol and particle size of 0.5–4.0 µm. The aerosol delivery time was preset at 1.2 s and the pause time between inhalations at 6 s. Baseline spirometry was performed, followed by five inhalations of saline as diluent control. This was followed by inhalations of two different concentrations (2.5 and 26 mg·mL−1) of methacholine, to produce cumulative doses ranging from 20–2,400 µg. Doubling doses were given within the dose range of 20–2,400 µg and all subjects received the same dose range. The FEV1 and FVC were recorded by a pneumotachograph system (Sensormedics 2450, Yorba Linda, CA, USA) 1 min after each dose of methacholine. Spirometric measurements were made in accordance with the recommendations of the American Thoracic Society 15. The FVC manoeuvre was continued until a plateau in the FEV1 curve was achieved by visual inspection and the minimum duration of the FVC manoeuvre was 6 s. MCT was stopped when either FEV1 fell by ≥20% from baseline, measured after saline inhalation, or the maximum dose (2,400 µg) of methacholine was reached. The PD20 and ΔFVC % were calculated using log-linear interpolation. Nineteen patients agreed to undergo repeat MCT 2 weeks after their first test, which was conducted at the same time of the day, in order to determine the repeatability of the proposed index.
Skin-prick tests to a standard array of 21 aeroallergens relevant to the local population and blood samples for absolute eosinophil count, IgE and ECP were performed in all subjects. The absolute eosinophil count was estimated by the Coulter method using Beckman-Coulter Gen-S; IgE level was obtained with immunofluorometry performed on the Immulite analyzer and the serum ECP was estimated using the Unicap testing system. The normal range for IgE was 5–100 IU·m−1.
The study was approved by the ethics committee and all subjects gave informed consent. The research was conducted according to the principles of the Declaration of Helsinki.
Statistical analysis
The data were not normally distributed, therefore nonparametric tests were used for analysis. The three asthma severity groups were compared using Kruskal-Wallis variation of Wilcoxon signed-rank test and correlations were performed using Spearman's rho testing. The Chi-squared test was used to compare qualitative variables, while the Mann-Whitney test was used to compare quantitative variables between two groups. A p-value of ⪕0.05 was considered significant. Repeatability of the new index was assessed by the method of Bland and Altman 16.
Results
Forty-six asthmatics participated in the study. The mean±sd age was 40.8±16.0 yrs with a male to female ratio of 2.1:1. The mean FEV1 (% pred) was 84.5±18.8 and FEV1/FVC (%) was 70.1±11.6. Sixty-five per cent of the subjects were found to be atopic and the majority (63%) whose skin-prick test was positive, developed reaction to mite antigen, 54% to house dust extract, 6.5% to cockroach antigen, 2.2% to cat and dog epithelia as well as 2.2% to grass and pollen extract.
There were 14 patients in the mild group, 21 in the moderate group and 11 in the severe group (table 2⇓). Nine subjects gave a history of endotracheal intubation for near-fatal exacerbation; three were in the moderate group and six in the severe group. Of these nine subjects, eight had case-record documentation of their intubation for asthma exacerbation. The average time interval was 22 months (range 12–54 months) between the event and conduct of the study. The frequency of symptoms and FEV1 (% pred) were significantly different among the three groups and the patients in the moderate and severe categories required higher doses of inhaled corticosteroid and β2-agonist (p<0.0001). Although there was no statistical difference in the absolute eosinophil count, IgE and serum ECP observed among the three groups, the mean IgE and serum ECP values were higher with increasing clinical severity. Peak flow diurnal variability over a period of 2 weeks was <20% in all patients except one patient in the severe group who had PEF variability of 22%, supporting that the majority of patient's asthma had been stable.
Characteristics of patients in three groups according to Global Initiative for Asthma classification of severity
While ΔFVC % and log(PD20) were able to categorize patients into the three asthma severity groups, the new index ΔFVC %/log(PD20) gave a smaller p-value (p<0.0001) than log(PD20) (p=0.001) and ΔFVC % (p=0.009) alone (fig. 1⇓). The new index also correlated better with GINA classification of severity (r=0.62, p<0.0001) and inhaled steroid usage (r=0.68, p<0.0001) than either index alone (table 3⇓).
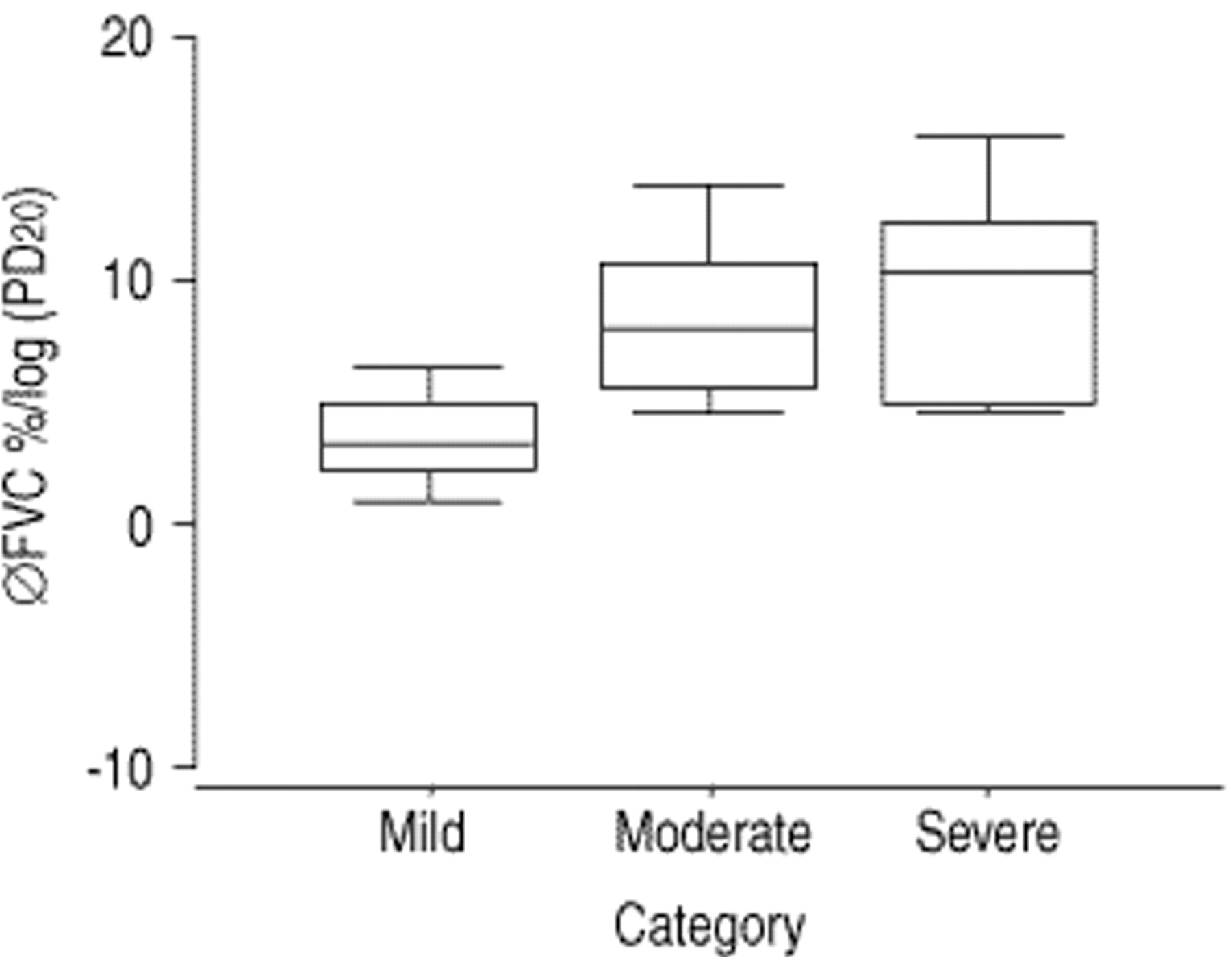
Distribution of the new index among three severity groups. The new index was good in categorizing patients into mild (n=14), moderate (n=21) and severe (n=11) (p<0.0001). ΔFVC %: maximal percentage fall in forced vital capacity at provocative dose of inhaled histamine or methacholine required to produce a 20% fall in the forced expiratory volume in one second (PD20). Mild versus moderate (p<0.0001); mild versus severe (p<0.0001); moderate versus severe (p=0.4).
Correlation of severity indices with other clinical and biochemical parameters
A detailed analysis of the indices between severity groups was conducted and it was found that all three indices were useful to varying degrees in categorizing patients into mild and moderate or severe groups: ΔFVC %/log(PD20), p<0.0001; log(PD20), p=0.001; and ΔFVC %, p<0.05. However for patients in the moderate and severe groups, no significant difference was observed for these indices. Neither of the indices correlated well with the eosinophil count, IgE or serum ECP levels (table 2⇑).
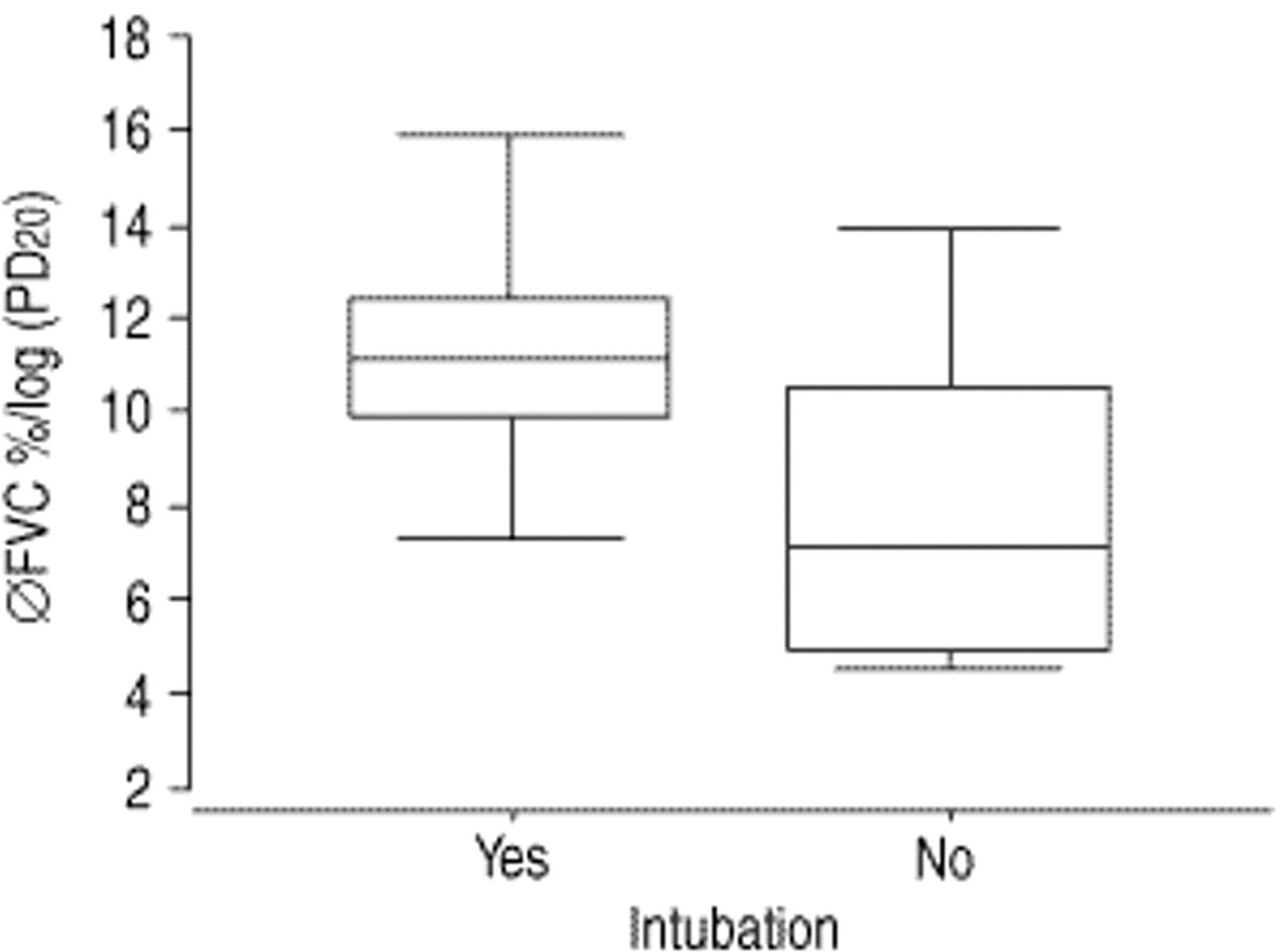
In the nine patients who had a previous history of endotracheal intubation for near-fatal exacerbation, the mean age was 44.4±15.8 yrs with a male to female ratio of 5:4. More than half (56%) were not atopic. The mean FEV1 (% pred) was 68.4±17.6 and the FEV1/FVC was 64.6±13.2%. The average doses of inhaled corticosteroid and β2-agonist used were higher in the intubated group, but they did not reach statistical significance (p>0.05). When these patients were compared with those without prior intubation within the moderate and severe groups, the new index was better than either ΔFVC % or log(PD20) in identifying patients at risk for near-fatal exacerbation (p=0.04) (table 4⇓ and fig. 2⇓).
{kind=link}
{kind=link}
The new index in the detection of patients at risk of near-fatal exacerbation in the moderate and severe groups. Within the moderate and severe groups, the new index was able to detect patients with a history of intubation from those without (p=0.04). ΔFVC %: maximal percentage fall in forced vital capacity at provocative dose of inhaled histamine or methacholine required to produce a 20% fall in forced expiratory volume in one second (PD20).
Characteristics of patients with previous history of intubation versus those without, in the moderate and severe groups
Measurements of log(PD20), ΔFVC % and ΔFVC %/log(PD20) made 2 weeks apart in 19 patients are presented in table 5⇓. There was no difference in ΔFVC %/log(PD20) measured between the first and second tests (p=0.2). The bias and 95% confidence interval for repeatability of the new index as calculated by the method of Bland and Altman 16 were −0.5 and −1.8–0.9, respectively.
Reproducibility study of the new index (Bland and Altman test)
Discussion
Asthma is a disease in which the airways narrow reversibly both too readily and too much in response to a wide variety of stimuli that have little or no effect on the normal lung. Airway narrowing that occurs too readily, i.e. BHR is easily assessed by measuring the PC20 or PD20 of an inhaled agonist that produces a 20% fall in FEV1. However, this does not assess the degree of excessive bronchoconstriction, which is an important pathophysiological abnormality that may predispose asthmatics to severe or even fatal attacks. Thus, it is not surprising that an imprecise relationship exists between PD20 and the clinical expression of asthma 4–6 as well as in the detection of those at risk of near-fatal exacerbation 7–9. Bronchoprovocation tests (BPTs) that employ high concentrations of agonist to measure the maximal response plateau directly are not practical for routine clinical purposes because of the inherent risks involved in producing an excessive fall in FEV1. The observation of a plateau on the dose-response curve in normal and mild asthmatics suggests the presence of protective factors, which prevent excessive airway narrowing 10, 17, 18. Although the reason why asthmatics lack a plateau is unclear, quantifying the degree of excessive bronchoconstriction during MCT by utilizing ΔFVC % as a surrogate marker in these patients may allow for early detection of those at risk of near-fatal exacerbation.
This study hypothesized that a new index, which combines both the ease of airway narrowing and excessive bronchoconstriction, ΔFVC %/log(PD20), may be better in assessing asthma severity and may prove useful in the identification of subjects at risk of near-fatal episodes. It was found that this new index was better than either individual index alone in assessing asthma severity. More importantly, it was able to discriminate subjects with previous intubation from those without. To the best of the authors' knowledge, the present study is the first to show that using a composite index of the ease of airway narrowing and excessive airway closure may be more indicative of the risk of near-fatal asthma, and that this may be safely measured during bronchoprovocation testing.
The results are in line with the recent observation of in'tVeen et al. 19 who showed that asthmatic subjects with severe disease and recurrent exacerbations have early airway closure during expiration, as demonstrated by an increased closing volume and closing capacity, in comparison with patients with severe but stable asthma. Their data indicate that such individuals who have difficult-to-control asthma with recurrent exacerbations are prone to airway closure, despite previous inhalation of a β2-agonist during a clinically stable period. The fact that the present findings are complementary is not unexpected, since a reduction in FVC during bronchoconstriction is likely to be determined by closure of small airways at low lung volumes 20, 21.
Although early and excessive airway closure seems to be a key factor in the pathogenesis of severe or near-fatal asthma, the pathophysiological correlation is complicated: airway closure in asthmatic airways is determined by a complex mechanical interaction of the airway structures including airway smooth muscle 22, pulmonary elastic recoil, airway parenchymal interdependence 23, thickness and elastic properties of the airway wall and submucosa 24–25, mucosal folding and mucosal liquid surface tension. Airway closure is therefore likely to be patchy and variable with respect to its distribution throughout the lung, and the lung volume at which closure occurs 26. King et al. 27 have recently shown that there are significant differences in airway closure between normal and asthmatic airways, and that in asthmatic airways, this distribution is patchy and uneven, probably as a result of the underlying allergic inflammation. Small-airway pathology is likely to induce airway closure 21, 23, potentially giving rise to air trapping during asthma exacerbation 23, 27. Because of the heterogeneity of asthma and the variable distribution of inflammation and airway closure, using a composite index of the ease of airway narrowing and excessive airway closure would seem logical. To be able to safely apply it during clinically stable periods of asthma would be of specific clinical relevance.
Although sudden and unexpected deaths in patients with mild and well-controlled asthma have been reported 28, studies of risk factors in fatal and near-fatal asthma indicate that these deaths occur more frequently in the setting of under-treated and unrecognized asthma. The epidemiological and clinical data are supported by post mortem studies of the airways in cases of fatal asthma which show extensive bronchial epithelial damage, mucous plugging, thickening of the basement membrane, airway smooth muscle hypertrophy and hyperplasia, and inflammatory cells in the airway wall. These pathological findings suggest long-standing, persistent airway inflammation and structural change 29–31.
It seems likely that patients with long-standing disease and altered airway structure are more likely to die from asthma. However, the exact mechanisms leading to death remain unclear. In some cases of asthma, where mucous plugging or submucosa oedema of the airways were not found at post mortem, excess bronchial muscle shortening was postulated to be an important cause of death 32. On the other hand, patients with status asthmaticus often had airways filled with mucous plugs. The controversy of possible mechanisms leading to death in asthma were further heightened when Azzawi et al. 33 and later Sur et al. 34 reported that there were more neutrophils and relatively less eosinophils in the airways of patients who died suddenly, than in those whose death occurred hours later. They concluded that these two groups of patients dying from asthma (i.e. “sudden versus slow”) could represent two distinct pathological entities initiated by different inflammatory stimuli, which resulted in excessive airway narrowing. On the other hand, it might be argued that the different profiles of inflammatory cells in relation to time observed in cases of fatal asthma could represent progression of airway inflammation. The duration of the fatal attack could be determined by pre-existing airway structure such as smooth muscle mass, mucous glands and airway thickness.
To date, good clinical and physiological methods for identifying persons at risk of severe morbidity and death from asthma are lacking 35 and the importance of determining the risk of fatal and near-fatal asthma by assessing airway hyperresponsiveness remains controversial.
This study has shown that, by combining the ease of airway narrowing and excessive bronchoconstriction, the new index found ΔFVC %/log(PD20) in contrast to ΔFVC % or PD20, was able to detect patients at risk of near-fatal exacerbation during their stable and optimized state. It was better in categorizing stable asthmatics into mild, moderate and severe groups and it correlated well with GINA classification, frequency of symptoms, FEV1 (% pred) and dose of inhaled corticosteroid. Good reproducibility of the index was also demonstrated over a 2-week period.
The limitations of the present study were the sample size and the number of patients with near-fatal asthma. Thus, it was not possible to determine threshold values of the index in the detection of this group of patients with greater accuracy. Nevertheless, the new index showed promise in its ability to discriminate asthmatics at risk of serious disease, by demonstrating a good correlation with clinical severity and corticosteroid requirement. Larger prospective, case-control studies are needed to validate the findings of the present study.
Conclusion
Although much of the focus of asthma research is directed towards ease of airway narrowing, it should not be forgotten that excessive gas trapping and hyperinflation can rapidly result in death and serious morbidity. This new index, which combines two important pathophysiological mechanisms for asthma, namely, ease of airway narrowing and propensity for excessive bronchoconstriction, may serve to alert the physician to closer monitoring of the asthmatic at risk of serious disease as well as be a useful adjunct in guiding asthma management.
Acknowledgments
The authors would like to thank C.H. Soh and A. Earnest for their invaluable input in the statistics section of the paper, M. Tang in the data collection and K.P. Leong for making serum eosinophil cationic protein estimation possible.
- Received August 25, 2000.
- Accepted March 3, 2001.
- © ERS Journals Ltd