



Serum procalcitonin in pneumococcal pneumonia in children
- M. Korppi and
- S. Remes
- M. Korppi, Dept of Paediatrics, Kuopio University Hospital, FIN-70210, Kuopio, Finland. Fax: 35 817172410
Abstract
Serum procalcitonin (PCT), a marker of bacterial infection, was measured in children with pneumonia to examine whether PCT can be used to screen pneumococcal (PNC) from viral pneumonia.
The number of patients was 132; mean age 3.0 yrs, and 64% were males. In all cases, pneumonia was radiologically confirmed, being alveolar in 46 and interstitial in 86 cases. The aetiology of infection was studied by a panel of serological tests for PNC, for five other respiratory bacteria and for seven common respiratory viruses. PNC infection was found in 25, mixed viral-PNC infections in 13 and viral infection in 17 cases.
In general, serum PCT was not associated with the type or aetiology of pneumonia. PCT values were >1.0 mg·L−1 in 40% of PNC cases, as compared to 12–15% in viral or mixed cases, respectively (p<0.05). PCT values were significantly higher in >2 yrs old children than in younger ones. The cut-off limits of 0.5 ng·mL−1, 1.0 ng·mL−1and 2.0 ng·mL−1 were tested for screening between PNC and viral pneumonia. The highest sensitivity of 55% was found at the 0.5 ng·mL−1 cut-off level, whereas the highest specificity of 88% was reached at the level of 1.0 ng·mL−1. The likelihood ratios, however, were far from optimal for both the positive and negative results.
Although marginally higher in pneumococcal pneumonia than in viral pneumonia, serum procalcitonin cannot be used to discriminate between these two types of pneumonia.
- children
- enzyme immunoassay
- pneumonia
- pneumococcus
- procalcitonin
- serology
Community-acquired pneumonia is a common clinical problem in childhood. Bacterial pneumonia cannot be differentiated from viral pneumonia on the basis of clinical or chest radiographic findings 1–3. In young children, the most important problem is how to differentiate between pneumonia caused by respiratory viruses and Streptococcus pneumoniae 1, 4. In addition, mixed infections caused by viruses and bacteria, especially respiratory syncytial virus (RSV) and pneumococci (PNC), are common 5. Leukocyte count, serum C-reactive protein (CRP) concentration or another nonspecific laboratory finding sometimes helps to differentiate between either bacterial or viral aetiology. In recent years, several studies have focused on the use of CRP in bacterial and viral respiratory infections in children, but the results have been inconsistent 6–8. Therefore, most children with pneumonia are treated with antibiotics without knowledge of the causative agent.
Procalcitonin (PCT) is a newly recognized marker of bacterial infection 9, it contributes to the differentiation between septic and other infections in neonates 10 and older paediatric patients 11. In a panel of children in which the aetiology of infection was assessed 12, it was examined whether PCT can be applied for the discrimination between bacterial and especially pneumococcal pneumonia and viral aetiology of pneumonia.
Material and methods
Study subjects
In the course of a prospective study in 1981–1982, 195 children were treated for presumed pneumonia in the Dept of Paediatrics, Kuopio University Hospital, Finland 4. The diagnosis of pneumonia, based on pulmonary infiltrations on chest radiographs evaluated by two radiologists, was confirmed in 161 cases. In 1999, there were 132 acute serum samples (82%) available for PCT measurements, and these cases form the material of the present study. Twenty-seven per cent of the patients were infants <12 months and 53% were <24 months of age. The mean age was 3.0 yrs, and 64% were males. The type of pneumonia was alveolar in 46 cases and interstitial in 86 cases
Study design
The clinical characteristics and aetiological findings of the patients have been published earlier 4, 12, 13. Pneumococcal aetiology was studied by antigen assays in acute serum and urine 4, by antibody assays to capsular C-polysaccharide (C-PS), to type-specific capsular polysaccharides (CPS) and to pneumolysin (PNL) in paired sera 4, and by immune complex assays measuring circulating C-PS, CPS and PNL specific complexes in acute and convalescent sera 13. Among the 132 patients of the present study, the antigen assays were positive in six cases, antibody assays in 14 cases and immune complex assays in 21 cases. Based on combined serological data, S. pneumoniae aetiology was indicated in 41 cases (32%).
Viral aetiology was studied by antibody assays in paired sera and antigen assays in nasopharyngeal aspirates for respiratory viruses, including RSV, parainfluenza 1, 2 and 3, influenza A and B, and adenoviruses 4. A viral infection was diagnosed in 38 cases; among them, RSV was identified in 30 cases.
In addition, antibodies were measured to Haemophilus influenzae, Branhamella catarrhalis, Mycoplasma pneumoniae and Chlamydia spp in paired sera, as described previously 4. One or more of these bacteria caused 13 (10%) infections. Mixed infection with S. pneumoniae was present in three and with RSV in six cases. All these cases were excluded from the aetiological analysis of the study.
In the present paper, the aetiological groups were as follows: PNC infection alone in 25 cases; mixed viral-PNC infection in 13 cases; viral infection alone in 17 cases (fig. 1⇓). The number of children with no aetiological findings was 64.
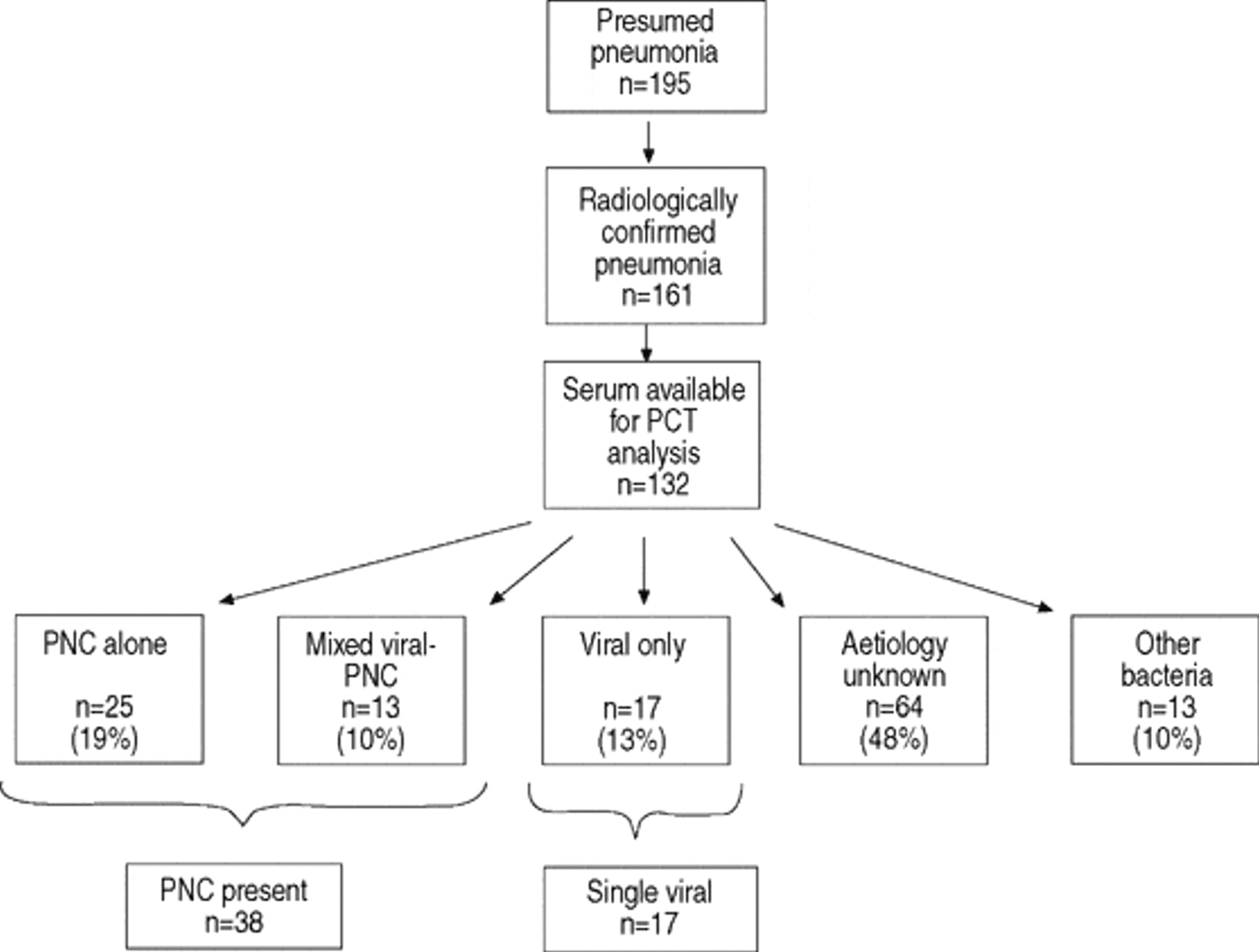
Flow chart of the present study. Six of the 13 children with other bacteria (see text) also had viral and three had PNC infection.
Methods
A serum sample was taken on admission, and stored at −70°C until studied for PCT. Serum PCT was measured by immune luminometric assay with the LUMItest procalcitonin kit (Brahms Diagnostica; GmbH, Berlin, Germany). The manufacturer's reference value for serum PCT was 0.5 ng·mL−1. White blood cell counts (WBC), erythrocyte sedimentation rates (ESR) and serum CRP concentrations were studied by routine methods, and the results have been published earlier 12.
Analysis
Due to the right-skewness of the serum PCT concentrations, the results are presented as medians and 25th–75th percentiles. PCT values are also presented in four groups: <0.5 ng·mL−1, 0.5–1.0 ng·mL−1, 1.0–2.0 ng·mL−1 and >2.0 ng·mL−1. Standard parametric and nonparametric tests were used in the statistical analyses. The diagnostic parameters sensitivity, specificity and likelihood ratios for the positive (LR+) and negative (LR−) test result were calculated by using routine equations.
Results
The association between the type of infiltration, that is alveolar or interstitial, and serum PCT concentrations was studied in a total of 132 children with radiologically verified pneumonia (table 1⇓). The median PCT was 0.45 ng·mL−1 (25th–75th percentile 0.22–1.20) in children with alveolar pneumonia and 0.28 ng·mL−1 (0.11–0.71) with interstitial pneumonia (p%0.067). Serum PCT values were significantly lower in children <2 yrs old than in older children; the medians (25th–75th percentile) were 0.24 ng·mL−1 (0.11–0.62) and 0.49 ng·mL−1 (0.13–1.15), respectively (p%0.02). The medians were 0.23 ng·mL−1 and 0.25 ng·mL−1 before 12 months and between 13 and 23 months of age, respectively. The association between the type of infiltration and PCT values was analysed also by the multiple linear regression model, adjusted for age, and the association remained nonsignificant (data not shown). A low PCT <0.5 ng·mL−1 was present in 79 children (60%). The respective figure for high PCT >2.0 ng·mL−1 was 11 (8%); nine (82%) children were >2 yrs old (p<0.05 versus younger children).
Serum procalcitonin (PCT) in 132 children with pneumonia in relation to the radiological type of infiltration
The association between the aetiology of infection and PCT values were studied in the 119 children with viral, pneumococcal or unknown aetiology of pneumonia (table 2⇓). No difference was seen between these groups, and mixed infections did not differ from single PNC or viral infections. Adjustment for age by the multiple regression analysis did not influence the results (data not shown). Serum PCT was >1.0 mg L−1 l in 40% of PNC cases, as compared to 12–15% of viral or mixed cases, respectively (p<0.05). Likewise, the median PCT was 0.81 ng·L−1 (25th–75th percentile 0.17–1.57) in children with single PNC pneumonia and only 0.48 ng·L−1 (0.19–0.69) in those with single viral pneumonia; the difference was not statistically significant (p%0.11). The PCT values varied from immeasurable to 6.4 ng·L−1, and the variation was wide within all aetiological groups.
Serum procalcitonin (PCT) in 119 children with pneumonia in relation to the aetiology of infection
The PCT values of 0.5 ng·mL−1, 1.0 ng·mL−1 and 2.0 ng·mL−1 were tested as screening limits between PNC and viral pneumonia (table 3⇓). In this analysis, the cases with PNC aetiology, whether single or mixed, were combined to the group of PNC pneumonia, and single viral cases formed the viral pneumonia group. The highest sensitivity was 55% at the 0.5 ng·mL−1 cut-off level, being of course, lower at higher levels. The highest specificity 88% was reached at the level of 1.0 ng·mL−1. At best, the likelihood ratio for the positive result was 2.6 and for the negative result 0.6, being far from optimal (>10 for LR+ and <0.1 for LR−). The receiver operator characteristic (ROC) curve for serum PCT as a predictor of pneumococcal versus viral pneumonia is shown in figure 2⇓.

{kind=link}
{kind=link}
The receiver operator characteristic (ROC) curve for serum procalcitonin in differentiating pneumococcal from viral pneumonia (see also table 4⇓). Area under ROC curve%0.6053.
Diagnostic parameters for serum procalcitonin in differentiating pneumococcal (PNC) from viral pneumonia.
A significant association was seen between serum PCT and CRP concentrations, but not between PCT and WBC or ESR results (table 4⇓). When PCT was <0.5 ng·mL−1, CRP was under 60 mg·L−1 in 86% of the cases. The agreement between the higher values was less pronounced.
Association between serum procalcitonin and other nonspecific inflammatory parametres in 119 pneumonia patients with pneumococcal, viral or unknown aetiology.
Discussion
Serum PCT values were marginally higher in PNC than in viral or mixed viral-PNC pneumonia, being higher in children ⇒2 yrs old than in younger children. In contrast, no significant difference was seen between alveolar and interstitial types of pneumonia. There was a high degree of overlapping between all age and diagnostic groups. As demonstrated also by the ROC curve, there was no cut-off limit with a good sensitivity and specificity for screening of PNC from viral pneumonia, suggesting an only minor value for PCT measurements in clinical practice.
Several studies have been published on PCT in the diagnosis of bacterial infection. However, no studies have been published on the role of PCT in bacterial pneumonia or in PNC pneumonia with careful aetiological assessments. An elevated, >0.5 ng·mL−1 serum PCT level was found in over half of PNC pneumonia cases, in agreement with previous studies on bacterial pneumonia 14, 15. On the other hand, that limit was exceeded as often as in one third of viral pneumonia cases. Many authors have reported elevated PCT concentrations in bacteraemic or septic infections 9, 16–18. in a recent study, pct distinguished better than crp bacterial from viral meningitis in children 9. Likewise, PCT seems to be better than CRP in the early diagnosis of neonatal bacterial infections 17. Like other nonspecific markers of inflammation, PCT may reflect more, the invasiveness than the bacterial aetiology of infection 12, also correlating with the outcome of infection 16, 17.
When measured by an immune luminometric assay, the manufacturer recommends the PCT value of >0.5 ng·mL−1 as elevated. Gendrel et al. 19 have suggested the value of 1.0 ng·mL−1 for the screening limit between viral and bacterial infections 19. In accordance, viral infections were rare (12%) in outpatients, if serum PCT concentration exceeded that limit. However, in both studies the values greatly overlapped between bacterial and viral infections 19. The observations on PCT were in agreement with previous observations on CRP 12. Viral pneumonia was rare if CRP exceeded a certain cut-off limit (60 mg·L−1), but no value was capable of ruling out bacterial aetiology of pneumonia 12. This similarity was as expected, since serum CRP and PCT associated significantly in the present study. Thus, serum PCT is not at any cut-off limit sufficiently sensitive or specific to be used for screening of PNC from viral or other bacterial pneumonia in clinical paediatric practice.
Recently, Toikka et al. 20 have suggested the 2.0 ng·mL−1 limit for the screening between bacterial and viral pneumonia in children. In this study with a large spectrum of community-acquired pneumonia mainly in young children, this limit was exceeded only in 8% of the cases. Other nonspecific inflammatory parameters, especially CRP, were also usually elevated in these children. Thus, the PCT value >2.0 ng·mL−1 >1.0 ng·mL−1, as seen also in the present study, seems to be sufficient to rule out viral aetiology of paediatric pneumonia 19.
Difficulties in determining the causative bacterial agent in pneumonia may have an impact on this result. The methods for testing PNC infections, although reasonably well validated 13, 20, 21, have been, until recently, used only in research laboratories. S. pneumoniae was detected by measuring soluble antigens and soluble antibodies to three antigens and by detecting immune complexes specific for the same three antigens 12. Despite this large diagnostic panel, most cases were diagnosed only by one assay for one antigen. Therefore, the clinical significance of PNC infections indicated by serological methods is thus far open, especially if the nonspecific host response indices are low and if the clinical signs resemble more viral than bacterial infection.
In conclusion, serum procalcitonin has a limited value in discriminating pneumococcal or other bacterial pneumonia from viral pneumonia in children.
- Received February 21, 2000.
- Accepted December 12, 2000.
- © ERS Journals Ltd.