



Fungal infections in transplant recipients
- 1Pulmonary Division and 2Dept of Radiology, University Hospital of Geneva, and 3Dept of Pathology, University Medical Centre, Faculty of Medicine, University of Geneva, Geneva, Switzerland
- L.P. Nicod, Pulmonary Division, University Hospital of Geneva, 24 rue Micheli-du-Crest, Geneva 14, CH-1211, Switzerland. Fax: 41 223729929
Abstract
Fungi are ubiquitous and the respiratory tract is exposed to aerosolized spores of both fungi that are “pathogenic” even in the normal host, such as Cryptococus neoformans, and those that are “opportunistic”, such as Candida and Aspergillus species, among others. Although these latter species may occasionally form fungal balls or induce allergic phenomena in the normal host, they produce more invasive diseases in immunosuppressed patients. Among these diseases, pseudomembranous aspergillosis has recently been described.
The diagnostic approach to these entities, and, in particular, the thin dividing line between colonization and infection are addressed, along with the diagnostic value of the various procedures.
New prophylactic regimens are reviewed such as the possibility of using amphotericin aerosols in combination with systemic azole administration.
The authors would emphasize the importance of restoring lung defences by not only decreasing immunosuppressive regimens but also considering the use of newly available recombinant cytokines such as growth factors, to reduce neutropenia, for instance, in addition to antifungal drugs when infection is diagnosed. However, immunomodulation procedures are far from being well established.
- fungal infections
- immunosuppression
- opportunistic infections
- prophylaxis
- transplantation
- treatment
Fungi are ubiquitous in nature and their constant aerosol exposure to respiratory tissue is unavoidable. Some, such as Cryptococcus neoformans and, in North America, Blastomyces, Coccidioides immitis or Histoplasma capsulatum are “pathogenic” even in the normal host. A separate group of potential fungal pathogens generally infect only those patients with abnormal host defences against infection. Among these so-called “opportunistic” fungi, Candida and Aspergillus species are those most commonly found in transplant patients 1 but others such as Torulopsis glabrata or Phycomycetes (Mucor or Rhizopus) can also occur.
The respiratory tract is an obvious portal of entry, especially soon after transplantation, not only because the immunosuppressive regimen is at its highest but also because the anatomical barrier of the mucosa is altered. Nevertheless, the gastrointestinal tract and intravascular catheters may occasionally be the source of fungal infection.
Incidence of fungal infection
Fungal infections have been reported to occur in 15–25% of patients after lung transplantation. In 1993, a 14% infection rate was reported in Pittsburgh, PA, USA, of which 56% was due to Candida and 33% to Aspergillus. The mortality rate reached 61% in these patients, with the first death occurring as early as 6 days after transplantation and a median occurrence at 44 days 2. Although, in some series of heart/lung and lung transplant recipients, Candida infections were more frequent than those due to Aspergillus 3, in others Aspergillus infections predominated 4, 5.
In the present authors' experience of lung transplantation, 84% of patients yielded positive respiratory specimens for fungi. Candida albicans were the most frequent isolates and were found in 20 of 31 patients 6. The second most frequently occurring fungus was Aspergillus fumigatus, isolated from 16 patients. Preoperative sputum examinations revealed A. fumigatus in three patients, two of whom immediately yielded a positive postoperative respiratory tract specimen, and one of whom developed invasive Aspergillus bronchitis. It is thus likely that most infections were hospital-acquired and caused by a contaminated water source, ventilation systems or construction projects. Among the Aspergillus species, A. fumigatus is the most common human pathogen. A. niger, A. terreus and A. nidulans are, however, also found. C. albicans was found in seven patients, one of whom yielded repeated respiratory tract and pleural fluid specimens positive for C. albicans immediately postoperatively. Other species, in particular C. norwegensis, C. lusitaniae and C. glabrata (or T. glabrata) were also isolated 6.
After liver transplantation, opportunistic fungi produce up to 37% of pneumonias, usually within 2–3 months of transplantation 7. Invasive mycoses are also more frequent after prolonged corticosteroid or antibiotic administration, prolonged surgery, retransplantation and systemic cytomegalovirus infections 7, 8. After kidney transplantations, 2–14% of infectious complications are caused by opportunistic fungi 9. Opportunistic pulmonary mycoses are more common after allogeneic than autologous bone marrow transplantation. This lower incidence is due to the shorter period of neutropenia and the quicker recovery of efficient immunity 10. Although Candida species are the most common isolates, Aspergillus is the most common cause of fungal pneumonia in patients following allogeneic bone marrow transplantation, and develops in up to 20% of them 11, 12, with the worst prognosis 13.
Pathologies related to most common fungi
Aspergillus species
The principal types of aspergillosis that affect immunocompromised patients are angioinvasive, chronic necrotizing and tracheobronchial. Other forms such as aspergilloma, allergic bronchopulmonary aspergillosis or bronchocentric granuloma are less commonly described following transplantation 14.
Invasive pulmonary aspergillosis
Classically, the major risk factors for invasive pulmonary aspergillosis include severe or prolonged neutropenia (absolute neutrophil count <500×106·L−1) and prolonged high-dose corticosteroid therapy 15. In the absence of an effective host immune response, the spores mature into hyphae that can invade the pulmonary structures, particularly blood vessels. This results in pulmonary arterial thrombosis, haemorrhage, lung necrosis and systemic dissemination.
Macrophages and granulocytes are the major immunoregulatory cells involved in host defences against fungal infections. It has been demonstrated that corticosteroids suppress macrophage and granulocyte function, whereas little effect of the suppression of T‐lymphocyte function by cyclosporin has been noted 16.
The isolation of Aspergillus from bronchoalveolar lavage fluid and/or sputum has been shown to correlate with the histopathological changes of invasive pulmonary aspergillosis in bone marrow recipients 17 in whom invasive forms cause the highest mortality 13. Aspergillus isolation from culture of respiratory secretions, pleural fluid or ascitic fluid has also been correlated with invasive Aspergillus infection and poor outcome in recipients of both liver and kidney transplants 18, 19. In cases in which the diagnosis need to be proven, transbronchial biopsy is usually of little sensitivity, being as low as 20% 20, whereas transthoracic needle biopsy or open lung biopsy provides a higher and more specific diagnostic yield 21.
Mortality rates from infections can be high (50–70%), and patient outcome depends on the early institution of antifungal therapy, the severity of the underlying disease and the speed of granulocyte recovery 15, 22.
Invasive aspergillosis has been described as occurring following up to 18% of heart and lung transplants 23, but mortality can be reduced with pre-emptive therapy and reduced immunosuppression 6, 24.
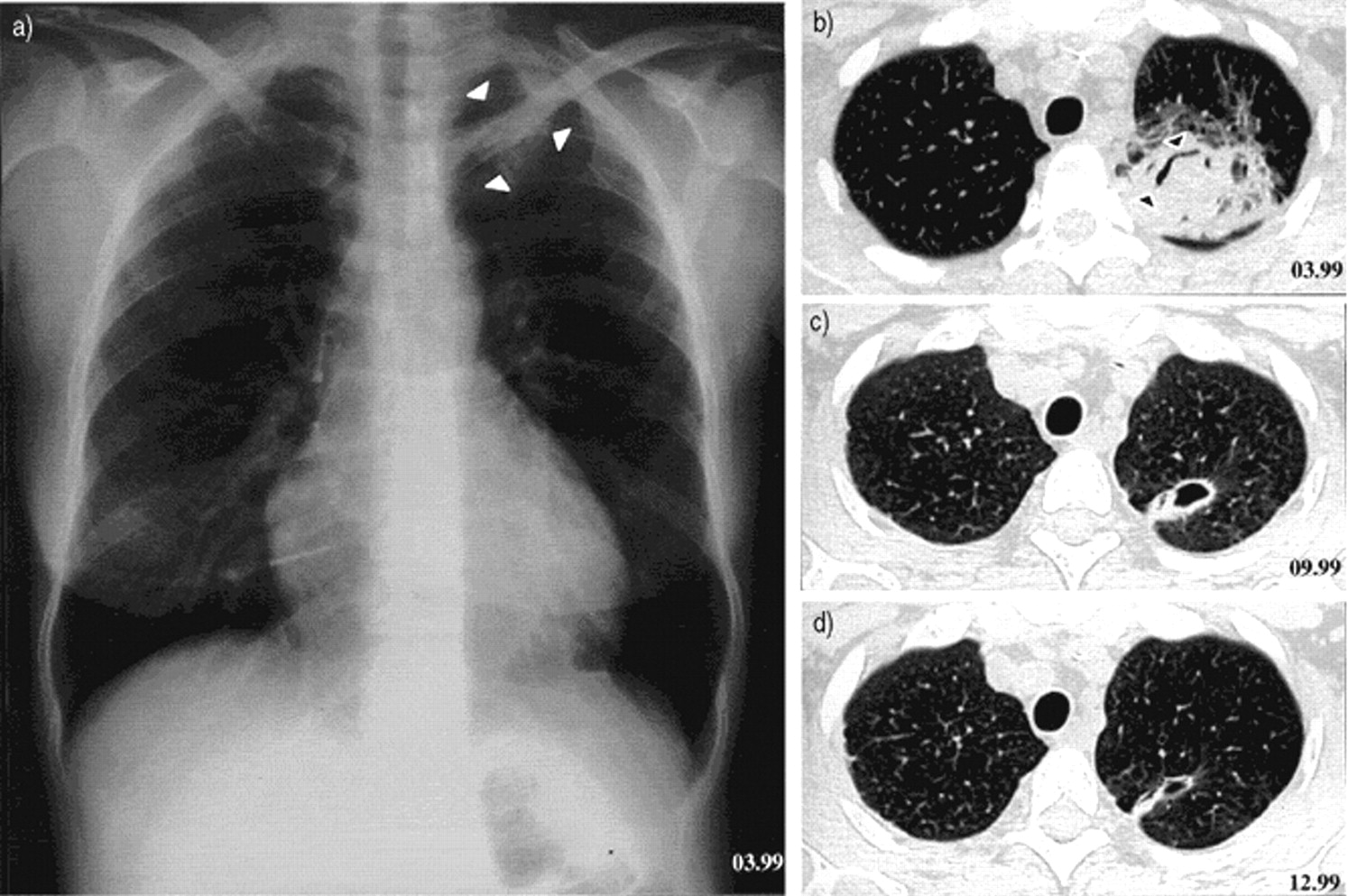
Invasive pulmonary aspergillosis appears on radiographs as multiple ill-defined 1–2‐cm nodules that gradually coalesce into larger masses or areas of consolidation (fig. 1⇓) 25. An early computed tomography finding, but seen with thin collimation, is the rim of ground-glass opacity surrounding the nodules (computed tomography halo sign) 26. This sign is, however, nonspecific and has also been described in patients with tuberculosis, mucormycosis and Wegener's granulomatosis 1. Cavitation is usually a late finding. The intracavitary mass composed of sloughed lung and the surrounding rim of air may be seen as “the air crescent sign”. Lobar consolidation is more common and less specific 27. Pleural effusion is unusual and adenopathy rare.
Ulcerative aspergillus tracheobronchitis
Aspergillus tracheobronchitis has been well described by Kramer et al. 4 as occurring at the bronchial anastomosis in the necrotic walls after lung transplantation, where it can cause deep ulceration or dehiscence. In the present authors' series, of the nine patients showing microscopic evidence of fungi on bronchial biopsy, two also showed clinical evidence of bronchial aspergillosis. One patient developed invasive pseudomembranous right-sided bronchial aspergillosis due to A. fumigatus ∼28 days after transplantation. This occurred on the medial proximal part of the donor bronchi, where a limited area (∼2.5×3 cm) of necrosis had been observed a few days after transplantation. The infection healed within 19 weeks of itraconozale treatment. In a second case, ∼3 weeks after transplantation, a pseudomembranous aspergillosis distal to the bronchial suture of the right main bronchus obstructed ∼80% of the luminal area while extending into the intermediate bronchus. Under itraconozale treatment, the bronchial aspirate remained positive for 4.5 months, and the bronchus infection was healed after 6 months.
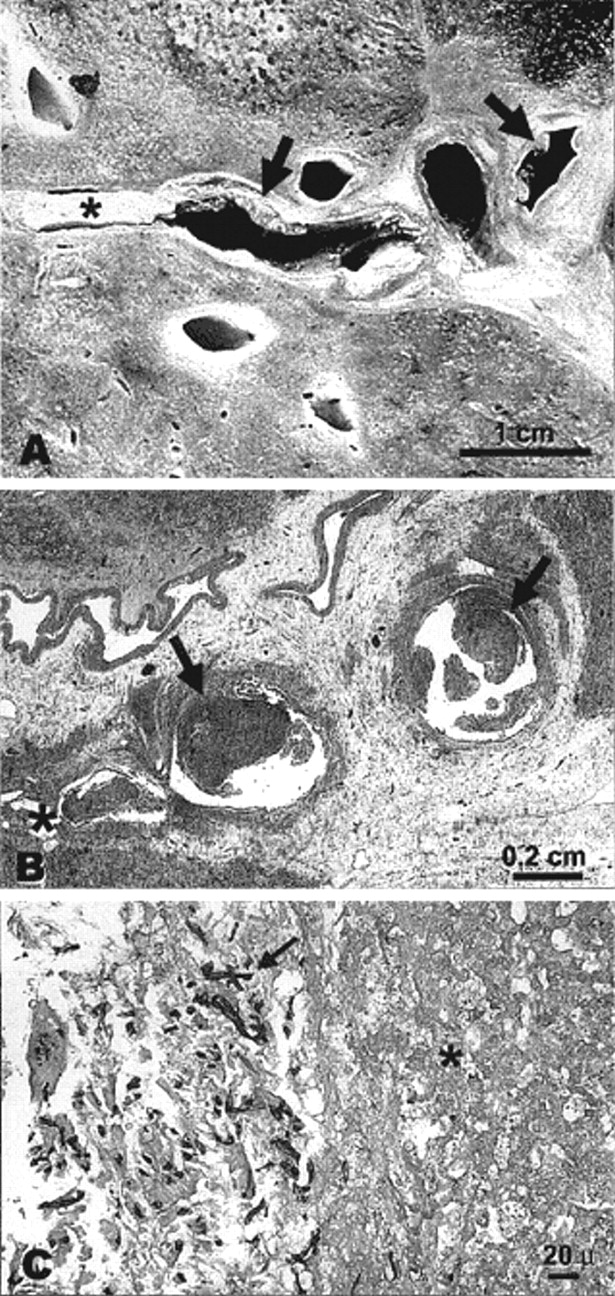
The present authors had a patient with ulcerative bronchitis due to Aspergillus >6 months after lung transplantation on a previously normal mucosa, while receiving high doses of inhaled steroids, and a few days after pulse steroid administration. These ulcerations healed 2 months later under itraconozale treatment (unpublished data). These forms of either invasive tracheobronchial aspergillosis or obstructive bronchopulmonary aspergillosis have been described not only after lung transplantation but also after allogeneic bone marrow transplantation and in patients with acquired immune deficiency syndrome 28, 29. An example of a pseudomembranous aspergillosis found on autopsy is shown in figure 2⇓.
Other forms of disease related to Aspergillus
Chronic necrotizing or semi-invasive aspergillosis typically occurs in patients with mild immunosuppression such as occurs in chronic obstructive pulmonary disease, sarcoidosis or underlying malignancy. It progresses slowly over a period of weeks or months. Aspergilli invade the tissues adjacent to cavities, increasing their size due to progressive necrosis. In transplantation, these slowly invasive forms are not described as distinct entities compared with the acute invasive forms.
Allergic bronchopulmonary aspergillosis has occasionally been described after transplantation 14. Milder forms may have local consequences such as bronchocentric granulomatosis that may be underestimated. The physiopathology of allergic bronchopulmonary aspergillosis and bronchocentric granulomatosis may be better understood in the near future with the recent observation that aspergilli share epitopes similar to the cytoplasmic structures of epithelial cells. These local infections could trigger autoimmune processes 30. It is possible that such phenomenona do occur in the lungs of transplant recipients, leading to bronchial inflammation and stenosis.
Aspergilloma can be present in pre-existing pulmonary cavities before transplantation. With immunosuppression, aspergilli can invade adjacent structures and lead to widespread disease 23. Preventive surgical removal of such mycetoma remains a matter of debate, especially for mycetoma resulting from previous invasive aspergillosis after bone marrow transplantation 31.
Candida species
Candida species are found in the human gastrointestinal tract, from oropharynx to anus, in the female gynaecological tract and on the skin 32. Small numbers of yeast colonies are normally present, increasing in number when the normal microbial flora is altered by antibiotics or when there is a defect in immune competence.
Disseminated candidiasis is one of the most common serious opportunistic mycoses in severely immunocompromised patients. Pulmonary candidiasis is uncommon, except in lung transplants, where they colonize and invade necrotic tissues and bronchial anastomoses. The clinical patterns range from mucocutaneous to invasive disease 23. If isolation of Candida from the sputum of many seriously ill patients on antibiotics is very common, pneumonia is considered unusual 33. Isolation of Candida from a patient with pulmonary infiltrates after lung transplantation should, however, not be dismissed as benign colonization, and, clearly, histological confirmation of invasive disease is essential for diagnosis and the institution of aggressive antifungal therapy. The clinical symptoms are usually nonspecific: prolonged fever despite broad-spectrum antibacterial therapy, accompanied or not by cough or haemoptysis. Chest radiographic abnomalities with disseminated candidiasis usually consist of patchy airspace consolidations in a lower lobe distribution 34, 35. Diffuse reticular or reticulonodular opacities are less common. Pleural effusions are reported in 25% of patients 33. Pulmonary cavitation and adenopathy are rare and the air crescent sign has also rarely been reported 36.
Mucormycosis
The most frequent genera within the family Mucoraceae to cause human infection are Mucor, Absidia and Rhizopus. Mucor is the most frequent, causing mucormycosis. Rhinocerebral mucormycosis in diabetic patients is perhaps the best-described infectious syndrome with Mucor, but increasing incidence of this invasive pulmonary infection among immunosuppressed patients has been reported 37. Other groups at increased risk of pulmonary mucormycosis are patients with diabetes mellitus, renal failure and burns 37.
Clinically, after inhalation or aspiration of organisms, pulmonary infection with Mucor can be chronic, such as in mycetoma, or acute. Like Aspergillus, these fungi have a propensity for invasion of pulmonary arteries, causing pulmonary artery thrombosis, pulmonary infarction and haemorrhage, with possible systemic dissemination. Cavitation is common, but the air crescent sign is seen less frequently in these patients than in aspergillosis.
Diagnosis relies on the demonstration of the typical broad nonseptate hyphae in lung tissues obtained by biopsy, aspiration, or autopsy. Treatment with amphotericin B is recommended, but survival from acute pneumonia in the compromised host is rare.
Rising opportunistic fungal infections
T. glabrata is a yeast-like organism, normally present commensally in the human vagina. T. glabrata pneumonias have been reported in myelosuppressed patients with neoplastic disease. T. glabrata was isolated from the bronchoalveolar lavage fluid of three of 26 of the present authors' lung transplant patients. Pneumonia can occur and progress despite amphotericin B treatment, but apparent lung infection has also been seen to regress without specific treatment, with bone marrow recovery after bone marrow transplantation 38.
Invasive fungal infections caused by unfamiliar species are increasingly being reported in immunocompromised patients 39. These emerging opportunistic fungi include Fusarium, a common plant pathogen; Penicillium marneffei; Trichosporon beigelii; Blastoschizomyces capitatus and Malassezia furfur. Thus Fusarium can cause disseminated infection similar to aspergillosis in profoundly neutropenic patients 40.
Cryptococcosis
C. neoformans is a fungus that exists as a yeast in both nature and tissue. The yeast cell is 4–6 µm in diameter, with a capsule, which, depending on the growth conditions, can make the entire organism range from 5–20 µm. It is abundant in soil and pigeon excrement.
Pulmonary cryptococcosis causes symptoms ranging from none to those of overt pneumonia. The resultant radiographic lesions vary from plate-like atelectases to diffuse interstitial infiltrates, from ill-defined tiny nodules to huge space-occupying masses. The progression of the disease varies with the state of immunosuppression 41. In immunocompromised patients, dissemination to extrathoracic sites such as the central nervous system, bone and skin is common 42. Immunocompromised patients often show few or no pulmonary symptoms, even in the presence of radiographically evident pulmonary abnormalities 42.
Positive sputum culture does not establish the diagnosis; it is therefore prudent to rely instead on demonstration of the fungus in tissue, either microscopically or on culture. Serum cryptococcal antigen titres are not usually elevated, except in patients with disseminated disease 42.
Treatment of fungal infection
Amphotericin B is the traditional drug of choice. The most prominent disadvantage of amphotericin B is its nephrotoxic effect. The treatment of aspergillosis with amphotericin B in solid organ transplant recipients results in a higher incidence of nephrotoxicity because of the concomitant use of cyclosporin 43. Liposomal amphotericin B (AmBisome) has far fewer side-effects and can be much more safely used in patients with solid organ transplants, despite concomitant use of cyclosporin A. In a series of 187 transplant recipients, liposomal amphotericin B was discontinued due to side-effects in 3% of cases. The overall mean increase in serum creatinine levels was 20%. Other side-effects included low serum potassium concentrations (36%) and a rise in alkaline phosphatase levels (26%) 44.
Liposomal amphotericin B markedly decreases the death rate due to aspergillosis in neutropenic patients after bone marrow transplantation from 90% down to 25% even when neutrophil counts are still low 45. The antifungal efficacy of AmBisome seems to be related to its ability to target fungi rather specifically 46.
Among azoles, fluconazole has been used effectively in localized Candida infections, and may also be an option in the treatment of systemic candidiasis 47, 48, but data supporting its use in pneumonia are lacking at the present time. Itraconazole or the new azole voriconazole 49 are effective therapies against aspergillosis, candidiasis or cryptococcosis. They are well tolerated. Enzyme-inducing drugs such as rifampicin and phenytoin significantly reduce the oral bioavailability of itraconazole, and plasma monitoring of its plasma concentration is recommended when enzyme-inducing agents are coadministered.
Itraconazole has been shown to be as effective as amphotericin B in small series of neutropenic patients 50, and in liver or heart transplant recipients 51, 52. An example of the evolution of invasive aspergillosis initially treated for 1 month with AmBisome followed by 9 months of itraconazole treatment is shown in figure 3⇓. Failure of itraconazole treatment of pulmonary aspergillosis in heart transplant recipients has been reported, but most of these patients had been maintained on high-dose steroids 53.
Modulation of immunosuppression has to be taken into account as a major component of fungal infection treatment. The use of haematological growth factors may prove to be useful in the near future in not only restoring the neutrophil count more quickly, but also increasing the capacity to contain fungal pathogens 54.
Prophylaxis of fungal infections
It is not easy to determine the pathogenic role of fungal isolates from the respiratory tract 55 i.e. to differentiate between infection, colonization and contamination. Several groups are very concerned by the high likelihood of disease when fungi are detected in respiratory tract specimens of either bone marrow or lung transplant recipients, especially with non-Candida strains 2, 56. It is important that potential transplantation candidates are screened for pre-existing fungal infections. Patients with positive cultures for Aspergillus and clinical or radiological signs suggesting an infection are usually given a therapy such as fluconazole for Candida or itraconazole and aerosolized amphotericin B for Aspergillus until signs of infection disappear 57.
Patients colonized with Aspergillus either before or after lung transplantation and receiving prophylaxis show a decreased rate of fungal infection. Indeed, aerosolized amphotericin B (0.6 mg·kg body weight−1·day−1) divided into three doses and oral fluconazole (400 mg·day−1) during the postoperative period prevented the early occurrence of any fungal infection in 52 lung transplant recipients 57. Some groups have started using 15 mg amphotericin B twice daily for 2–3 months, as prophylaxis, with excellent preliminary results and little or no toxicity. In the present authors' lung transplant patients, fungi were found post-transplantation in the lower respiratory tract specimens of 26 of 31 (84%) patients, predominantly C. albicans (20 patients) and A. fumigatus (16 patients). Mycelia characteristic of Candida sp. or Aspergillus sp. were found in necrotic tissue at the bronchial suture in nine patients. Fluconazole (200 mg·day−1) or itraconazole (200–400 mg b.i.d.) was systematically used according to presumed fungal sensitivity after the discovery of fungi in lower respiratory tract samples. The mean duration of the 38 treatments was 3.6±2 months. After a median follow-up of 16 months, two cases of extended ulcerative and pseudomembranous A. fumigatus bronchitis observed early were also resolved under itraconazole treatment 6. Postoperative pre-emptive azole therapies thus appear well tolerated and effective in lung transplant recipients.
Azoles have been shown to be safe and efficient in the prevention of some invasive fungal infections in bone marrow transplantation 58, 59. Ketoconazole has been used in recent heart and kidney transplant studies. A cost-sparing effect was obtained by reducing the cyclosporin dosage required and because of its efficacy in preventing fungal infections and achieving a lower rejection rate 60, 61. However, care should be exercised not only because of drug interactions with azoles, but also because primary or secondary resistance to the antifungal drugs used may occasionally develop 62, 63.

A 55-yr-old female with “leukaemia and agranulocytosis”. a) Chest radiograph showing multiple bilateral focal areas of consolidatior. b) High-resolution chest computed tomography (slice thickness 1 mm) revealing dense focal parenchymal nodules with surrounding air crescents (hollow arrowheads) and ground-glass opacity (solid arrowheads), reflecting progressive necrotizing pneumonia. Invasive pulmonary aspergillosis was confirmed on autopsy.

Manifestations of pseudomembranous fungal bronchitis in a lung transplantation recipient on autopsy. A) Fibrinous or pseudomembranous bronchitis (arrow) with subocclusion of the airways (asterisk indicates subocclusion of the airways by pseudomembranes); B) fibrinonecrotic material (arrow) from the airway shown in A, with subocclusion of the bronchial lumen (asterisk); and C) rare Aspergillus hyphae (arrow) in the lumen without invasion of the necrotic bronchial wall (asterisk). (Internal scale bar a=1 cm; b=0.2 cm; c=20 µm.)
{kind=link}
{kind=link}
{kind=link}
A 47-yr-old female who underwent bone marrow transplantation in February 1999 for myelodysplasia. a) The chest radiograph 1 month later shows an ill-defined retroclavicular opacity in the left upper lobe (arrowheads). b) High-resolution chest computed tomography (CT; slide thickness 1 mm) reveals an area of dense focal consolidation with an air crescent (arrowheads) strongly suggestive of invasive aspergillosis. c, d) Follow-up CT examinations after 1 month of AmBisome followed by 9 months of itraconozole, after a further: c) 6 months; and d) 9 months.
Footnotes
Previous articles in this series: No. 1: Hammerschlag MR. Chlamydia pneumoniae and the lung. Eur Respir J 2000; 16: 1001–1007. No. 2: Ewig S, Schäfer H, Torres A. severity assessment in community-acquired pneumonia. Eur Respir J 2000; 16: 1193–1201.
- Received January 31, 2000.
- Accepted June 26, 2000.
- © ERS Journals Ltd