





Abstract
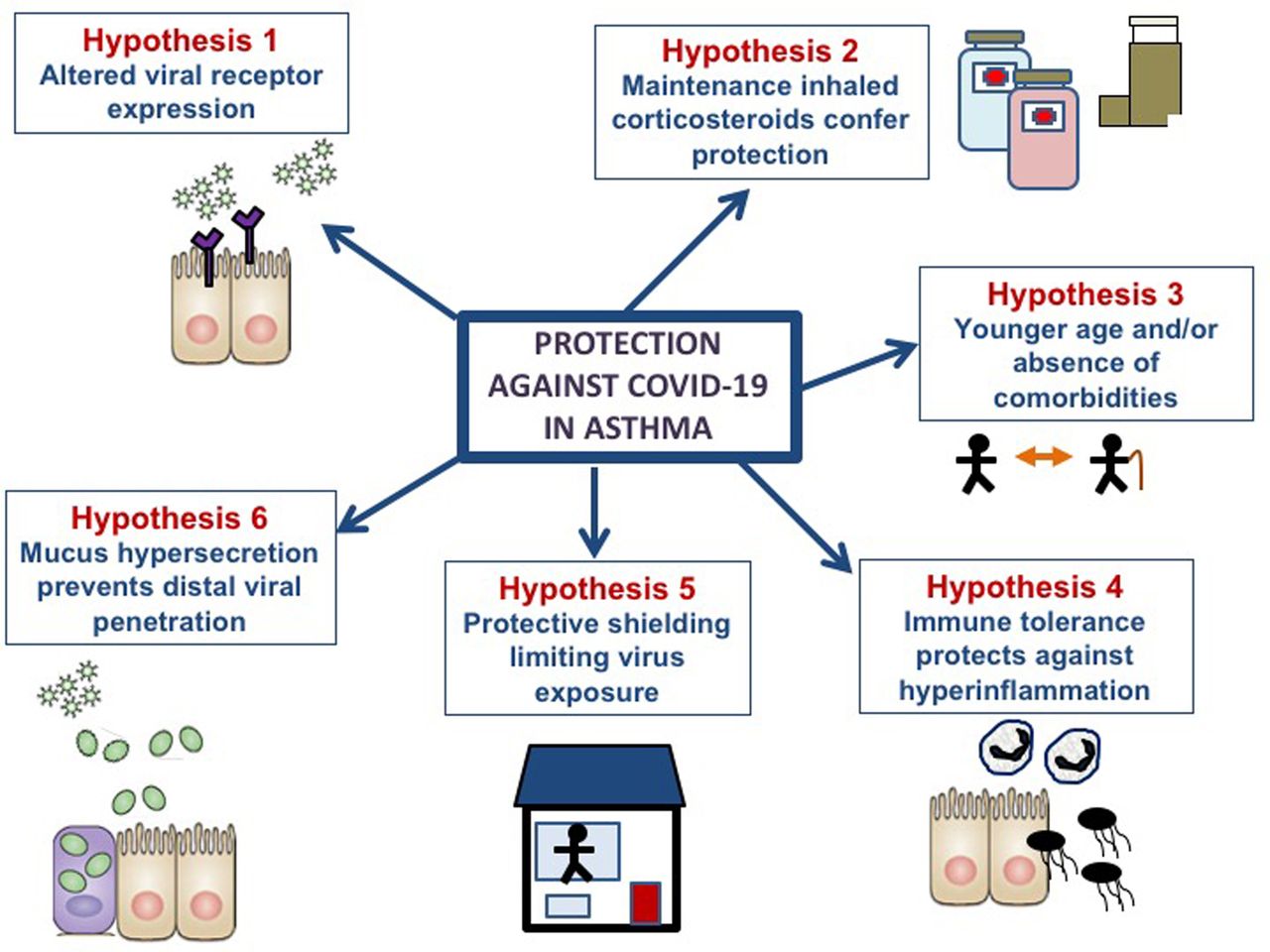
Asthma may protect against poor outcomes in COVID-19 due to several possible mechanisms including altered viral entry receptor expression, inhaled corticosteroid use, chronic inflammation, reduced viral exposure due to shielding and/or mucus hypersecretion.
To the Editor,
We read with interest the study by Beurnier et al. describing a lower prevalence of asthma (4.8%) in a cohort of 768 patients hospitalised with COVID-19 compared to the general population, none of whom presented with an asthma exacerbation and only one who was treated for bronchospasm. This subgroup also had significantly reduced mortality compared to a control group without asthma [1]. These findings must be considered preliminary given that they arise from a relatively small, single-centre cohort. In particular, the control group differed significantly in age (older) and gender balance (greater male:female ratio), both associated worse outcomes and raising the possibility that the results represent statistical artefact. However, if corroborated, these data reflect a surprising departure from previous respiratory viral pandemics, most recently the 2009 H1N1/Influenza A outbreak, where asthma was observed to be a major comorbidity in patients requiring hospitalisation (∼25% of admissions in a UK series [2]). Asthma was subsequently shown to be associated with an increased risk of acquisition of H1N1/Influenza A virus [3] and consequent exacerbation [4]. Strikingly, the original SARS-CoV-1 pandemic was also characterised by an extremely low prevalence of chronic lung disease comorbidities [5], further suggesting that SARS-associated coronaviruses may not exacerbate asthma to the same extent as other respiratory viruses.
The mechanisms underlying this phenomenon are unknown. The authors propose two hypotheses to explain their observations: a lower expression of angiotensin-converting enzyme 2 (ACE2), the putative viral entry receptor for SARS-CoV-2, in asthma and/or a protective effect of inhaled corticosteroids (ICS), the mainstay of maintenance treatment in asthma, with ICS treatment linked to reduced sputum ACE2 expression in asthma [6]. We suggest three further hypothetical mechanisms. Firstly behavioural factors are likely to be important. Protective shielding for at-risk groups including those with asthma has been widely advocated by international guidelines. Reduced exposure to SARS-CoV-2 amongst patients with asthma may therefore be contributing to the low prevalence of asthma in hospitalised cohorts. However the low rates of chronic respiratory illnesses in case series from the start of the pandemic before social distancing measures were introduced, suggests this cannot be the sole explanation. Government policies to limit the spread of the pandemic have also led to reductions in air pollution, which increases the severity of virus-induced asthma exacerbations [7].
Secondly chronic inflammation in asthmatic lungs, arising from repeated epithelial insults by aeroallergens, pollutants and viruses, may lead to a degree of immune tolerance that could in turn act to restrict the development of the excessive inflammatory response that drives severity in COVID-19. Accordingly, pre-existing asthma was associated with reduced systemic inflammation in patients hospitalised with influenza [8] and reduced sepsis and sepsis-related mortality in pneumonia [9]. Type 2 inflammation, present in ∼50% of those with asthma, also protects against the development of sepsis in experimental models of bacterial respiratory infection [10].
Finally, mucus hypersecretion, a hallmark of asthma, may prevent SARS-CoV-2 from reaching the distal lung and protect from pathology. Secreted mucus rich in mucin glycoproteins, such as Muc5ac, acts as a first line of defence against infection. Asthma is associated with increased expression of MUC5AC [11] which, when over-expressed in transgenic mice, protects against influenza infection with reduced viral loads and attenuated cellular airway inflammation compared to wild-type controls [12]. It is thus conceivable that mucus hypersecretion in individuals with asthma prevents SARS-CoV-2 from penetrating far enough to gain access to the alveolar type 2 cells, the cells predominantly expressing ACE2 in the lung. However, mucus hypersecretion is not present in all those with asthma and may therefore only confer protection in some individuals. It is also notable that other conditions characterised by high sputum burden and increased mucins (e.g. COPD) are, in contrast, associated with poor outcomes from COVID-19. In these patients, other factors, such as old age and comorbidities, may offset any protective effect of increased mucus or other biological mechanisms.
In summary, a number of factors may be acting in concert to drive a potential protective phenotype observed in SARS-CoV-2 infection in asthma suggested from the study by Beurnier et al. (see fig. 1 for summary). Large-scale longitudinal studies incorporating sampling, such as that being undertaken by the International Severe Acute Respiratory Infection Consortium (ISARIC), should shed light on how immune responses to SARS-CoV-2 differ in individuals with and without asthma. Trials of recombinant human ACE2 (NCT04335136) and ICS (NCT04416399, NCT04355637) are also ongoing, the results of which are eagerly awaited. Understanding the basis of differences in susceptibility to severe COVID-19 between asthmatic and non-asthmatic populations may ultimately offer important insights into therapeutically exploitable targets to reduce the overall burden of COVID-19.
{kind=link}
Hypotheses to explain the low prevalence of asthma in hospitalised COVID-19 and relatively improved outcomes in these patients.
Footnotes
Conflict of interest: Dr. Farne has nothing to disclose.
Conflict of interest: Dr. Singanayagam has nothing to disclose.
- Received August 6, 2020.
- Accepted October 23, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










