





Abstract
Decreased FEV1 after complete ICS withdrawal in severe COPD was not progressive and did not predict clinical changes http://ow.ly/TtYDV
To the Editor:
The combination of an inhaled long-acting β2-agonist with an inhaled corticosteroid (ICS) is widely used in the management of chronic obstructive pulmonary disease (COPD), primarily to prevent exacerbations [1]. Concerns about the increased risk of pneumonia, even with newer ICS [2], have generated interest in whether the ICS can be safely withdrawn from patients with COPD. We recently reported, in the WISDOM (Withdrawal of inhaled steroids during optimized bronchodilator management) study (clinicaltrials.gov identifier number: NCT00975195), that patients who continued treatment with a long-acting β2-agonist plus a long-acting muscarinic antagonist did not have an increased risk of exacerbations [3]. However, we observed a statistically significant difference in forced expiratory volume in 1 s (FEV1) after complete ICS withdrawal and at the end of the study in favour of continued ICS treatment.
Here we present data on the time course of lung function in the WISDOM study before, during and after ICS withdrawal using the results of daily home-based spirometry. With daily measurements of lung function, we aimed to explore the time course of the change in lung function in more detail. Some of the results from this study have been previously reported in the form of an abstract [4].
The WISDOM study methodology and results have been published previously [3, 5]. Briefly, following a 6-week run-in on a combination treatment with long-acting β2-agonist/long-acting muscarinic antagonist/ICS (salmeterol/tiotropium/fluticasone propionate), patients with COPD were randomised to either continue this treatment or have the ICS withdrawn in a stepwise manner over 12 weeks.
Lung-function change was measured using spirometry (EasyOne; NDD Medical Technologies, Chelmsford, MA, USA, and Zurich, Switzerland) performed by trained staff during clinic visits and, following suitable training, by the patients themselves each day throughout the 52-week study. In the clinic lung function was assessed post-bronchodilator at the screening visit where patients were allowed to take their medication in the morning. The baseline value for lung function was assessed pre-bronchodilation at the randomisation visit. After randomisation, the first step-down in ICS dose from 500 to 250 µg twice daily took place in the group who discontinued ICS.
Predefined end-points included changes from baseline to study weeks 6, 12, 18 and 52 in trough FEV1 (measured in the clinic), and changes from baseline to study weeks 6, 12, 18, 27, 36, 45 and 52 in weekly mean FEV1, measured by home spirometry in the 7 days before the corresponding clinic visit. These end-points were analysed using a restricted maximum likelihood-based repeated measures approach adjusting for baseline FEV1. To determine the comparability of in-clinic and home-based spirometric data, a post hoc Bland–Altman analysis was performed to establish the level of agreement between these measurements.
A post hoc exploratory analysis of 46 consecutive weeks of home-based spirometric data was also undertaken. The 6 weeks immediately before the study week 12 clinic visit (ICS reduction from 250 µg to 100 µg twice daily) were designated as weeks −6 to −1 and the 40 weeks immediately after complete ICS withdrawal as weeks 1 to 40. For each week, the weekly mean FEV1 for each patient was calculated if there were at least four measurements during the 7-day week, with no imputation for missing data. A separate analysis of covariance with terms for treatment and baseline FEV1 was performed on the change from baseline at each week and the adjusted means presented graphically for each treatment group. The rates of change in FEV1 from week 6 to week 40 (stable phase 6 weeks after the last change in treatment) were compared using a random-effects model adjusting for baseline FEV1.
A total of 2488 patients were randomised to study treatment and 2027 completed the study. Baseline in-clinic spirometry data were available for 2441 patients (n=1223 randomised to continued ICS treatment, and n=1218 to ICS withdrawal). The treatment groups were generally well matched in terms of baseline demographic and clinical characteristics. The Bland–Altman analysis of the overall study period showed good agreement between home-based and in-clinic data with a mean difference of between 40 and 50 mL that was consistent over time.
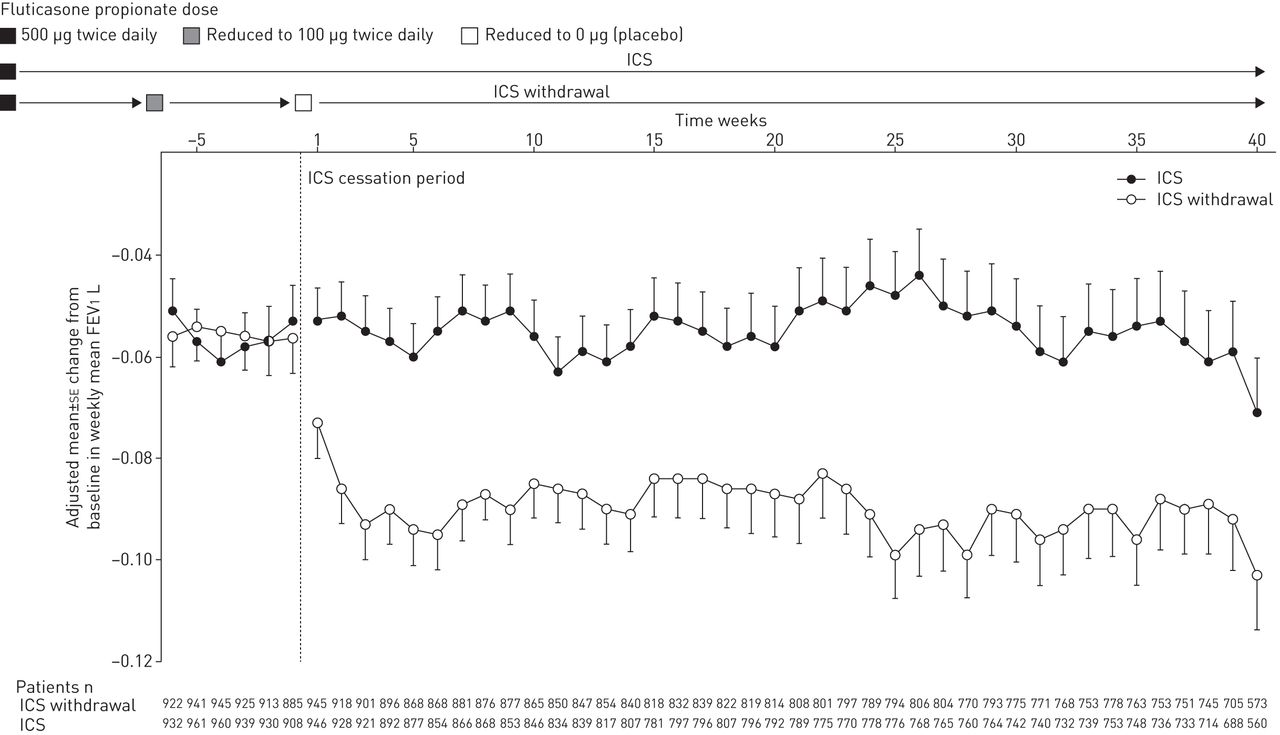
Analysis of the predefined end-points showed a decrease in weekly mean FEV1 in the ICS-withdrawal group starting ∼6 weeks after complete withdrawal of ICS. The adjusted mean treatment differences in on-treatment weekly mean FEV1 were 4 mL and 6 mL at study weeks 6 and 12, when patients were on medium- or low-dose ICS, respectively, increasing to 42 mL at study week 18 (p<0.001). The treatment difference remained statistically significant at subsequent visits, ranging from 36 mL at study week 27 to 48 mL at study week 52, compared with the in-clinic difference in trough FEV1 at study week 52 of 43 mL. The post hoc analysis revealed that the decrease in FEV1 observed in the ICS withdrawal group started in the first week following complete withdrawal of ICS and continued for a further 2 weeks (fig. 1), after which FEV1 stabilised. During the stable phase from week 6 to week 40 after ICS withdrawal, no further decrease in FEV1 was observed in the ICS withdrawal group and the slopes of FEV1 in the two groups were similar (p=0.408).
{kind=link}
Adjusted mean±se change from baseline in on-treatment weekly mean forced expiratory volume in 1 s (FEV1) 6 weeks before and 40 weeks after complete inhaled corticosteroid (ICS) withdrawal. The timeline for the figure is anchored to clinic visit 5, the point at which ICS therapy was discontinued. Therefore, the weeks shown in the figure correspond to the time before or after study week 12 and do not correspond to actual study weeks. Week −1 corresponds to the home-based data gathered the week prior to withdrawal and weeks 1–40 correspond to the weekly home-based data gathered after ICS discontinuation. Only patients with home-based data after ICS withdrawal have been included. The total number of patients included in the analysis who contributed a weekly mean for at least one of week 1 to week 40 after ICS withdrawal was 2135 (1066 in the ICS group, and 1069 in the ICS withdrawal group).
Our study design has strengths and limitations. Strengths include the large sample size and the use of weekly mean FEV1 values based on at least four data points, which helped to overcome the impact of day-to-day variability. Potential limitations of this analysis of home-based spirometry are its post hoc nature and the potential unreliability of estimates of weekly mean FEV1 based on four unsupervised home readings per week. However, the overall numbers of weekly mean FEV1 values for the period of interest (weeks 1–40 after ICS withdrawal) were similar for the two treatment groups over time, allowing valid comparisons to be made between them.
Starting ICS treatment has been shown to result in a small but significant increase in post-bronchodilator FEV1 compared with placebo or a long-acting β2-agonist [2, 6, 7]. Conversely, withdrawing ICS treatment is associated with a fall in the in-clinic measurements of FEV1 and worsening of symptoms [8, 9]. Our analysis shows that lung function can be maintained with low doses of ICS and that ICS withdrawal was associated with a nonprogressive reduction in lung function within 3 weeks of complete withdrawal. Thereafter, the change in spirometry over time was not different to that seen in patients still taking an ICS. Moreover, patients who continued to take an ICS had a similar disease course in terms of lung function to those who withdrew from ICS treatment. Although lung function worsened, the change was small, not progressive and did not predict clinically important changes, at least over the follow-up period of this study.
Acknowledgements
Medical writing assistance was provided by Marshall Naden (Complete HealthVizion, Glasgow, UK), which was contracted and compensated by Boehringer Ingelheim Pharma GmbH & Co. KG (Ingelheim, Germany).
Footnotes
Support statement: This work was supported by Boehringer Ingelheim Pharma GmbH & Co. KG. Funding information for this article has been deposited with FundRef.
Conflict of interest: Disclosures can be found alongside the online version of this article at erj.ersjournals.com
- Received August 21, 2015.
- Accepted October 7, 2015.
- Copyright ©ERS 2015










