





Abstract
U-BIOPRED is a European Union consortium of 20 academic institutions, 11 pharmaceutical companies and six patient organisations with the objective of improving the understanding of asthma disease mechanisms using a systems biology approach.
This cross-sectional assessment of adults with severe asthma, mild/moderate asthma and healthy controls from 11 European countries consisted of analyses of patient-reported outcomes, lung function, blood and airway inflammatory measurements.
Patients with severe asthma (nonsmokers, n=311; smokers/ex-smokers, n=110) had more symptoms and exacerbations compared to patients with mild/moderate disease (n=88) (2.5 exacerbations versus 0.4 in the preceding 12 months; p<0.001), with worse quality of life, and higher levels of anxiety and depression. They also had a higher incidence of nasal polyps and gastro-oesophageal reflux with lower lung function. Sputum eosinophil count was higher in severe asthma compared to mild/moderate asthma (median count 2.99% versus 1.05%; p=0.004) despite treatment with higher doses of inhaled and/or oral corticosteroids.
Consistent with other severe asthma cohorts, U-BIOPRED is characterised by poor symptom control, increased comorbidity and airway inflammation, despite high levels of treatment. It is well suited to identify asthma phenotypes using the array of “omic” datasets that are at the core of this systems medicine approach.
Abstract
Severe asthma results in more airway inflammation, worse symptoms and lower lung function, despite increased therapy http://ow.ly/QznR3
Introduction
A substantial number of patients with asthma require systemic corticosteroids to control symptoms and/or suffer from poor control and frequent severe exacerbations despite currently available treatment [1, 2]. Although recently developed biologic compounds targeting cytokines of the type 2 pathways show promise [3, 4], identification of new treatment targets and the selection of patients best suited to respond to individual biologics is still hampered by a poor understanding of the physiological, pathological and molecular heterogeneity of severe asthma [5, 6].
Severe asthma is a collection of disease entities with varying pathophysiological characteristics [7] that result in symptoms of cough, wheeze and breathlessness, with frequent exacerbations. To address the problem of phenotypic difference and heterogeneity, the Unbiased Biomarkers for the Prediction of Respiratory Disease Outcomes (U-BIOPRED) project was set up in 2009 as a public–private partnership within the framework of the Innovative Medicines Initiative, engaging academia, the pharmaceutical industry and patient groups. The aim of U-BIOPRED is to identify multi-dimensional phenotypes of severe asthma and new treatment targets using a combination of state of the art “omics” (transcriptomic, proteomic, lipidomic and metabolomic) technologies applying a systems biology approach [8], thereby driving unbiased discovery in both adult and paediatric severe asthma [9]. This novel approach is designed to make drug development more effective and efficient.
We present the baseline characteristics of the adult participants with severe asthma who form the majority of the U-BIOPRED cohort and compare these participants with those suffering from mild/moderate disease, in terms of their clinical, symptomatic, functional and biomarker features. In a parallel paper the characteristics of the paediatric cohort are reported. These first publications of U-BIOPRED will serve as the reference documents for all subsequent publications using the “omics” technologies that are at the core of this programme.
Methods
Participants
This was a multicentre prospective cohort study recruiting from 16 clinical centres in 11 European countries. Details of the participating centres, assessments and standard operating procedures are available in the online supplement. Prior to enrolment participants with severe asthma were required to have been under follow-up by a respiratory physician for at least 6 months, during which time assessments had been undertaken to optimise asthma control and medication adherence [2]. The study was approved by the ethics committee for each participating clinical institution, and adhered to the standards set by International Conference on Harmonisation and Good Clinical Practice. It is registered on ClinicalTrials.gov (identifier: NCT01982162). All participants gave written and signed informed consent.
Adult groups
The definition of severe asthma used in this study was agreed at a U-BIOPRED consensus meeting [2]. Participants with asthma had either airflow reversibility (increase in forced expiratory volume in 1 s (FEV1) >12% predicted or 200 mL following inhalation of 400 µg salbutamol), airway hyperresponsiveness (methacholine provocative concentration causing a 20% fall in FEV1 <8 mg·mL−1, or diurnal peak expiratory flow amplitude >8% of mean), or a decrease in FEV1 of 12% predicted or 200 mL within 4 weeks after tapering maintenance treatment. Four groups were recruited, as follows.
Group A: severe nonsmoking asthma (SAn)
Participants in this group were nonsmokers for at least the past 12 months, with a less than 5 pack-year smoking history, with asthma and uncontrolled symptoms defined according to Global Initiative for Asthma (GINA) guidelines [10] and/or frequent exacerbations (more than two per year) despite high-dose inhaled corticosteroids (≥1000 µg fluticasone propionate per day or equivalent dose).
Group B: smokers and ex-smokers with severe asthma (SAs/ex)
This group was defined as for the SAn group except that they were either current smokers or ex-smokers with a smoking history of at least 5 pack-years.
Group C: mild/moderate nonsmoking asthmatics (MMA)
Participants in this group were nonsmokers for at least the past 12 months, with a less than 5 pack-year smoking history and had controlled or partially controlled asthma symptoms, as defined by GINA, whilst receiving a dose of <500 µg fluticasone propionate/day or equivalent.
Group D: healthy nonsmoking controls (HC)
These participants had no history of asthma or wheeze, had no other chronic respiratory disease, were nonsmokers for at least the past 12 months with a smoking history of ≤5 pack years and their pre-bronchodilator FEV1 was ≥80% pred.
Protocol and assessments
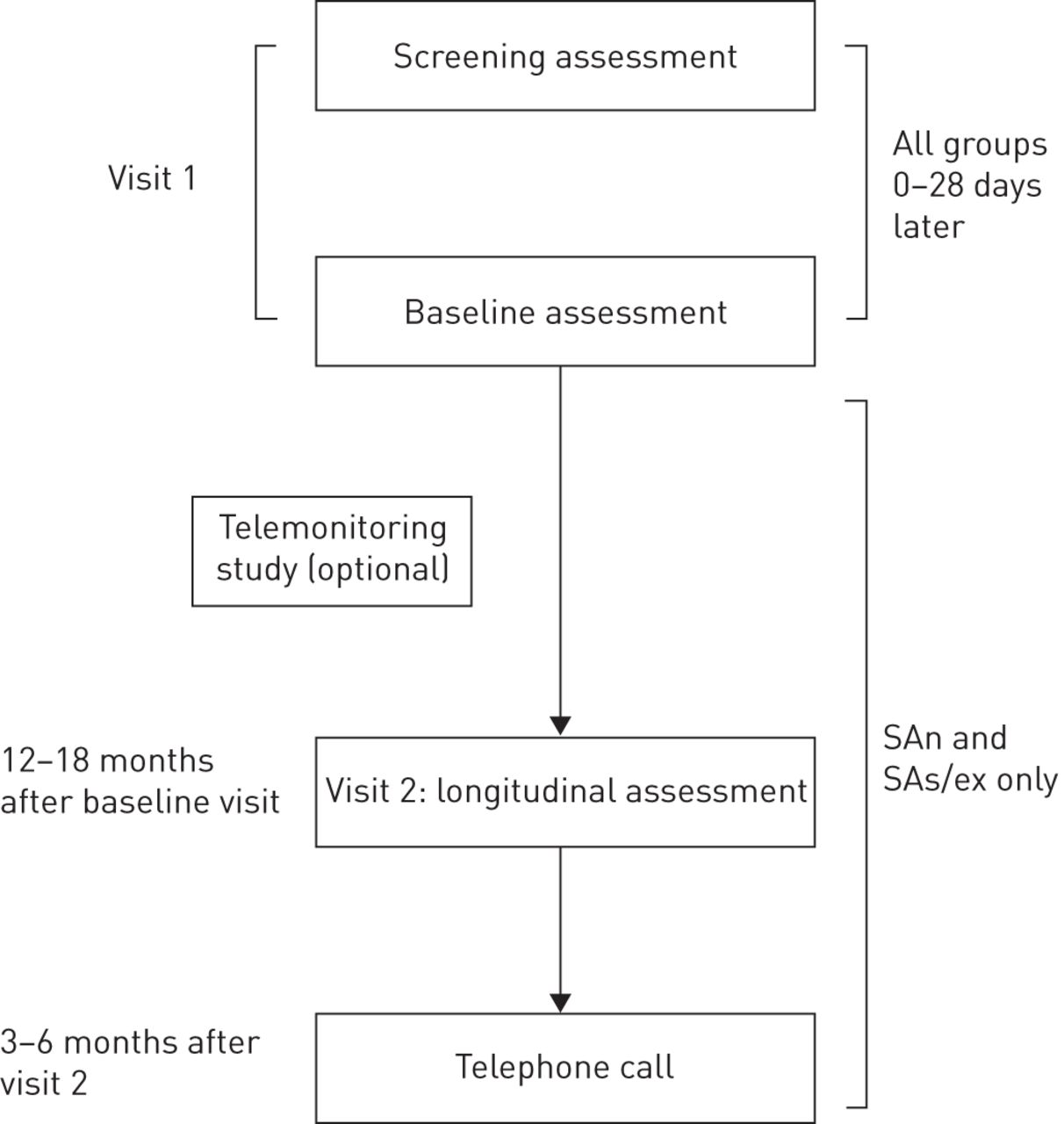
Participants attended a screening visit to assess eligibility for the study (figure 1). They underwent a baseline visit (up to 28 days later) and were invited to attend for an optional bronchoscopy, high-resolution lung computed tomography and telemonitoring sessions. Spirometry, haematological profiles, and fraction of exhaled nitric oxide level (FeNO) at 50 mL·s−1 were performed. Induced sputum was obtained [11] and differential sputum eosinophil and neutrophil counts measured following a standardised operating procedure. Sputum supernatants and cell pellets were collected. Allergic status was obtained by either skin prick testing or measurement of specific immunoglobulin (Ig)E to six common aeroallergens. Blood and urine samples were taken for lipidomic, proteomic and transcriptomic analyses for later assessment. An optional sample was taken for genetic analysis. Subsets of participants underwent plethysmographic measurements, high-resolution computed tomography and collection of exhaled breath for measurement of metabolites including volatile organic compounds, all for future analyses. All investigations were performed according to standardised operating procedures (online supplement).

Visit schedule. SAn: severe nonsmoking asthma group; SAs/ex: smokers and ex-smokers with severe asthma.
Participants with severe asthma were reviewed at 12–18 months after enrolment and were also invited to attend if they experienced an exacerbation. At 12–24 months they were contacted by phone or by post to obtain information on asthma control.
Data were entered on an electronic case report form. The study was run and monitored by Cromsource (www.cromsource.com). Samples were sent to the Centre for Integrated Genomic Medical Research Biobank in Manchester, UK. Datasets were uploaded on to the tranSMART system, an open-source knowledge management platform for sharing research data [12] supported by the European Translational Information and Knowledge Management Services (eTRIKS) project.
The study aims are published on the U-BIOPRED home page (www.europeanlung.org/en/projects-and-research/projects/u-biopred/home).
Questionnaires
The following were administered at baseline: 1) the Asthma Control Questionnaire (ACQ5) [13] to assess current asthma control; 2) the Asthma Quality of Life Questionnaire (AQLQ) [14] to assess quality of life and psychological morbidity; 3) the Hospital Anxiety and Depression Scale (HADS) [15]; 4) Sino-Nasal Outcomes Test (SNOT20) [16] to measure upper airway symptoms; 5) the Epworth Sleepiness Scale (ESS) [17] to measure sleep and daytime drowsiness; and 6) the Medicines Adherence Response Scale (MARS) [18] to measure adherence.
Statistical analysis
Continuously distributed data were either summarised using mean±se if symmetrical, or median (interquartile range) values. Nonsymmetrical variables all exhibited positive skew and were log-transformed prior to association testing. Missing data were not imputed. p-values were calculated using a general linear model for continuous variables or a general logistic model for categorical variables. No adjustment for multiple testing was applied as the analyses were considered exploratory. Analyses were performed using R version 2.15.2 (R Core Team, 2012; www.r-project.org).
Results
A total of 610 adults were recruited over an 18-month period: 311, 110, 88 and 101 into the SAn, SAs/ex, MMA and HC groups, respectively (table 1 and figure 2).
Group demographics
There were more females in the SAn group (66%) compared to the other asthma groups (50%), with the age of onset of asthma 18 years later in the SAs/ex compared with SAn group. Participants with severe asthma had a higher body mass index (BMI) than those in the MMA and HC groups and were older (table 1). Both severe asthma groups experienced 2.5 exacerbations in the preceding 12 months as compared with 0.4 in the MMA group (p<0.001). There was a higher rate of intensive care unit admissions in the SAn participants compared to the SAs/ex group (p<0.05). Further split of the severe asthma groups based on current and ex-smoking is presented in the online supplement (table S5).
Spirometry
FEV1 (% predicted or actual) was lower in the three asthma groups compared to the HC group (p<0.001), with the severe asthma groups having the lowest FEV1. Forced vital capacity (FVC) (% predicted or actual) was also lower in both the SAn and SAs/ex groups when compared to the MMA (p<0.001) and HC groups (p<0.001). The mean FEV1/FVC ratio was lower in those with severe asthma (0.64 and 0.61, respectively) compared to the MMA (ratio 0.72; p<0.001) and HC groups (ratio 0.79; p<0.001), respectively (table 1).
Medications
Within the SAn and SAs/ex groups 46% and 45% respectively received daily oral corticosteroids, and 17% and 16%, respectively, received anti-IgE therapy. Use of nebulised β-agonist was higher in the SAn and SAs/ex groups. Other classes of therapy were also used (table 2).
Medications
Questionnaires
ACQ and AQLQ scores reflected worse asthma control and increased morbidity in both severe asthma groups with minimal impairment in the MMA group. A similar pattern was seen with anxiety and depression. There were more upper airway symptoms measured using the SNOT20 in both severe asthma groups compared with the MMA group. Similarly the ESS scores indicated that there was an increase in sleepiness in the severe asthma groups compared to only a very mild impairment in the MMA group (table 3).
Questionnaires
The MARS questionnaire scores for adherence to treatment recorded by the three asthma groups were in the range of 21 to 22, with the severe asthma groups recording higher scores (p<0.005), indicating better adherence. The AQLQ score was correlated to several variables, including FEV1 (95% CI 0.5 to 0.7; p<0.001), FEV1/FVC (95% CI 1.14 to 2.8; p<0.001), exacerbations in the previous year (95% CI −0.8 to −0.2; p<0.001), BMI (95% CI −0.006 to −0.002; p<0.001) and pack-years smoked (95% CI −0.003 to −0.001; p<0.001) (figure 3).

Consort diagram. CT: computed tomography; GWAS: genome-wide association study; NA: not applicable.

Contour plots of the Asthma Quality of Life Questionnaire (AQLQ) related to baseline demographics. Figures represent scatter plots describing the relationship between each factor and the asthma quality of life z-score. The contour lines are coloured blue to red, to indicate increasing density of points in the graph. The density was modelled using two-dimensional kernel density estimation. The contour plots show weak inverse relationships and particularly the scatter between quality of life and c) exacerbations, e) body mass index (BMI) and f) smoking history (pack-years), a strong inverse relationship between quality of life and d) asthma control (ACQ5) and weak positive relationships between quality of life and a, b) measures of lung function (forced expiratory volume in 1 s (FEV1) and FEV1 to forced vital capacity (FVC) ratio).
Atopy and comorbidities
There was a high incidence of atopy in the four groups, at 70% in the asthma groups and 46% in the HC group. The incidence of allergic rhinitis, hay fever and nonallergic rhinitis were highest in the asthma groups. Participants in the HC group were much less allergic with only a third reporting hay fever and only a sixth, rhinitis or eczema.
The presence of nasal polyps was associated with severe asthma, regardless of smoking status (four-fold increased incidence in SAn and SAs/ex groups versus MMA group; p<0.001) (table 4). No such association was seen with allergic or nonallergic rhinitis, hay fever or reported eczema. Gastro-oesophageal reflux disease was more common in severe asthma (46% SAn, 63% SAs/ex) than in MMA (21%) and HC (11%), with a greater incidence reported in the SAs/ex group versus the SAns group (p=0.004).
Comorbidities
Blood and sputum biomarkers
Blood eosinophil counts were similar in all three asthma groups. Each group had a significantly higher blood eosinophil count than the HC group (SAn versus HC, p=0.002; SAs/ex versus HC, p=0.005; MMA versus HC, p<0.001). Blood neutrophil counts were significantly higher in the severe asthma groups compared to the MMA group.
Sputum samples were provided and met criteria for analysis in 44.2% of the asthma participants and 40.6% of the HC group. Median sputum eosinophil counts for the SAn, SAs/ex, MMA, and HC groups were 2.75%, 4.13%, 1.05% and 0%, respectively (table 5). The sputum eosinophil count was higher in the two severe asthma groups combined compared to the mild/moderate asthma group (table 5; figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
a) Sputum eosinophil count and b) sputum neutrophil count, by cohort. The boxes represent median and interquartile range values; whiskers extend to the extreme point, no more than 1.5 times the interquartile range from the box, with outliers denoted by open circles and raw data by black circles overlaid. SAn: severe nonsmoking asthma; SAs/ex: smokers and ex-smokers with severe asthma; MMA: mild/moderate nonsmoking asthma; HC: healthy nonsmoking controls.
Biomarkers in blood, sputum and exhaled air
There were no significant differences in differential sputum neutrophil counts between the two severe asthma groups, which when combined were significantly higher compared to the MMA group (table 5).
There was a significant negative association between log sputum eosinophils (absolute or %) and FEV1 (% predicted or actual value) when all cohorts were considered and an adjustment for age, sex and smoking was applied. There were significant negative associations between log blood eosinophils (%) and FEV1/FVC ratio (p=0.002) and between blood neutrophils (%) and actual FEV1 (p=0.002) and FEV1/FVC ratio (p=0.026).
Exhaled nitric oxide
FeNO levels in all asthma groups were higher than those in the HC group, but the FeNO levels in the severe asthma groups were not different from the levels in the MMA group. The presence of nasal polyps was associated with a higher FeNO (mean increase 2.1 ppb, 95% CI 1.5 to 2.9 ppb; p<0.001) (table 5).
Discussion
In this large European cohort, patients with severe asthma experienced more symptoms, more exacerbations, higher levels of anxiety and depression, and a higher incidence of nasal polyps, gastro-oesophageal reflux symptoms and airflow obstruction than patients with milder disease. The clinical characteristics of asthma were present despite higher doses of treatment that included doses of inhaled corticosteroids equal or more than 1000 µg of fluticasone (or equivalent), with 45% of the combined severe asthma group receiving a daily dose of prednisolone. The characteristic features of the severe asthma U-BIOPRED cohort are similar to those reported in previous cohort studies [6, 19–21]. While the entry criteria for severe asthma were comparable for most of these cohort studies, the ENFUMOSA study required a lower threshold with an inhaled corticosteroid dose of ≥1200 µg of budesonide or beclomethasone with at least one exacerbation in the past year. Of these five cohorts, the current U-BIOPRED severe asthma cohort appears to be the most severe with a higher reported exacerbation rate of 2.5 per year, a reduced mean FEV1 of 67.5% of predicted and a higher proportion of patients on oral corticosteroid therapy taking a mean dose of 14 mg per day.
One of the novel features of the U-BIOPRED cohort is the inclusion of a smoking and ex-smoking severe asthma group. Patients with asthma who smoke have been reported to have poorer disease control and a reduced therapeutic response to inhaled corticosteroids [22], possibly through the induction of corticosteroid insensitivity [23, 24]. However, our analyses of the nonsmoking and the smoking/ex-smoking severe asthma groups identified few differences in demographics, airway physiology, inflammatory markers and asthma symptoms between these groups. In both groups, a similar percentage received oral corticosteroid therapy; they also had similar degrees of airflow obstruction. The slightly lower level of FeNO in the smoking/ex-smoking group might be explained by an effect of current smoking [25]. One notable difference is that asthma onset occurred on average 18 years later in the smokers and ex-smokers than in the nonsmokers, and yet the degree of airflow obstruction measured was similar. One interpretation is that there may be a more rapid rate of loss of lung function in the patients with asthma who smoke. The significant correlation between AQLQ scores and the number of pack-years of smoking exposure would also support a contribution of cigarette smoke to impaired quality of life in this group. We also split the demographic data of the groups by smoking status rather than severity (table S5 of the online supplement). This revealed that current smokers had a lower BMI compared with ex- and never-smokers.
In agreement with the SARP study [20], patients with severe asthma (especially smokers) were less frequently atopic than those with mild/moderate disease. There was also a clear association of both nasal polyps and gastro-oesophageal reflux disease with disease severity, with approximately one-third and one-half reporting polyps and reflux respectively, a finding that is in keeping with previous reports [5]. Nasal polyps are commonly found in severe asthma, and are associated with a particularly severe phenotype. There is evidence that treating nasal polyps with anti-IgE therapy results in better asthma outcomes [26]; however, whether this is due to an effect on the underlying asthma or the polyps is unknown. The link with higher FeNO levels is in keeping with work showing that nasal polypectomy leads to a fall in FeNO [25].
Our findings are also similar to other studies published from severe asthma registries. In agreement with both the British Thoracic Society's [27] and Belgium's [28] severe asthma registries our patients are predominantly female, with a high BMI and evidence of fixed airflow obstruction. Moreover there are similarly high levels of reflux, nasal polyps and exacerbations despite greater levels of medication.
We found a greater degree of sputum eosinophilia in the two severe asthma groups compared to the mild/moderate asthma group. Up to 60% of patients in the two severe asthma groups had a differential sputum eosinophil of >1.9% (the established upper limit of normal for differential sputum eosinophil counts [29]). This percentage is similar to previous reports in severe asthma [21]. The level of sputum eosinophilia observed in the mild/moderate asthma group are also similar to those reported previously [30].
The higher blood neutrophil count in participants with severe asthma may represent the effect of systemic corticosteroids which can increase blood neutrophil numbers. Sputum neutrophil counts were similar in the three asthma groups and were significantly higher than in the healthy control group. This similarly could represent the effect of corticosteroids although severe asthma has been linked to a higher level of sputum neutrophils [31, 32].
The impact and burden on our participants' health was noticeable with measures of symptoms and quality of life being far worse in severe asthma as compared to mild/moderate asthma, despite the use of higher doses and more classes of asthma treatment. Levels of anxiety and depression were also higher with severe asthma. There were significant relationships between quality of life measures and airflow obstruction, smoking history and BMI, supporting the contribution of these factors to an impairment of quality of life; however, the scatter of data reveals that these parameters are not closely related. The number of exacerbations experienced was greater than 2.5 exacerbations per participant in both severe asthma groups in the preceding year. These findings highlight the need for an integrative assessment of clinical and physiological disease markers and, additionally, biological markers of disease in the assessment of severe asthma. For example, the finding that bariatric surgery has an effect on measures of airway hyperresponsiveness [33] and is associated with a lower all-cause mortality at 5 years particularly in younger, predominantly female populations [34] may point towards the need for specific and targeted intervention in people with severe asthma and obesity.
There are several limitations to our study. First, there is no perfect way to assess treatment adherence; however, we only approached patients managed in a specialist respiratory clinic and only those who had been assessed to be adherent were eligible for the study. Furthermore, MARS scores were high, indicating good levels of self-reported adherence. Secondly, subjective or historical data were assessed by questionnaire which may be prone to recall bias. Thirdly, the success rate in obtaining adequate quality sputum for analysis was in the 42–50% range and the number of bronchoscopies was relatively lower in the SA and SAs/ex groups. Finally, due to the numerous formulations and inhaler devices used across Europe it was not possible to calculate the precise daily equivalent inhaled corticosteroid dose for each participant and therefore these data are not shown; however, high (>1000 μg FP) or low (<500 μg fluticasone propionate per day) dose was a study entry requirement for the severe and moderate groups, respectively.
We have been successful in recruiting a substantial cohort of patients with the most severe asthma that has similar characteristics to previously reported cohorts. This gives confidence that the U-BIOPRED consortium will define distinct phenotypes and endotypes of severe asthma. Matching these data to the “omics” information with future unsupervised analyses will help identify new treatments for patients with severe asthma who currently have limited treatment options, and will improve our understanding of this important chronic disease.
Acknowledgements
This paper is presented on behalf of the U-BIOPRED Study Group with input from the U-BIOPRED Patient Input Platform, Ethics Board and Safety Management Board. We thank all the members of each recruiting centre for their dedicated effort, devotion, promptness and care in the recruitment and assessment of the participants in this study.
The members of the U-BIOPRED Study Group are as follows: Kamran Tariq, NIHR Southampton Respiratory Biomedical Research Unit, Clinical and Experimental Sciences, NIHR-Wellcome Trust Clinical Research Facility, Faculty of Medicine, University of Southampton, UK; Patrick Dennison, NIHR Southampton Respiratory Biomedical Research Unit, Clinical and Experimental Sciences, NIHR-Wellcome Trust Clinical Research Facility, Faculty of Medicine, University of Southampton, UK; Annelie F. Behndig, Umeå University, Sweden; Wim van Aalderen, Academic Medical Centre, University of Amsterdam, The Netherlands; Rene Lutter, Academic Medical Centre, University of Amsterdam, The Netherlands; Ariane Wagener, Academic Medical Centre, University of Amsterdam, The Netherlands; Kees van Drunen, Academic Medical Centre, University of Amsterdam, The Netherlands; Pieter-Paul Hekking, Academic Medical Centre, University of Amsterdam, The Netherlands; Paul Brinkman, Academic Medical Centre, University of Amsterdam, The Netherlands; Koos Zwinderman, Academic Medical Centre, University of Amsterdam, The Netherlands; Nadia Mores, Università Cattolica del Sacro Cuore, Italy; Giuseppe Santini, Università Cattolica del Sacro Cuore, Italy; Salvatore Valente, Università Cattolica del Sacro Cuore, Italy; Christos Rossios, Imperial College, UK; David Gibeon, Imperial College, UK; Uruj Hoda, Imperial College, UK; João Pedro Carvalho da Purificação Rocha, Royal Brompton and Harefield NHS Foundation Trust, UK; Adesimbo Sogbesan, Royal Brompton and Harefield NHS Foundation Trust, UK; Julaiha Gent, Royal Brompton and Harefield NHS Foundation Trust, UK; Andrew Menzies-Gow, Royal Brompton and Harefield NHS Foundation Trust, UK; Davide Campagna, University of Catania, Italy; Jeannette Bigler, Amgen Inc.; Michael J. Boedigheimer, Amgen Inc.; Wen Yu, Amgen Inc.; Xugang Hu, Amgen Inc.; Klaus Fichtner, Boehringer Ingelheim Pharma GmbH & Co. KG; Katja Nething, Boehringer Ingelheim Pharma GmbH & Co. KG; Damijan Erzen, Boehringer Ingelheim Pharma GmbH & Co. KG; Ralf Sigmund, Boehringer Ingelheim Pharma GmbH & Co. KG; Martina Gahlemann, Boehringer Ingelheim (Schweiz) GmbH; Kathrin Riemann, Boehringer Ingelheim Pharma GmbH & Co. KG; Alix Berton, Boehringer Ingelheim Pharma GmbH & Co. KG; Matthias Klüglich, Boehringer Ingelheim Pharma GmbH & Co. KG; Jens Hohlfeld, Fraunhofer ITEM; Philipp Badorrek, Fraunhofer ITEM; Cornelia Faulenbach, Fraunhofer ITEM; Anna James, Karolinska Institutet, Sweden; Ann-Sofie Lantz, Karolinska University Hospital & Karolinska Institutet, Sweden; Elisabeth Henriksson, Karolinska Institutet, Sweden; Roelinde Middelveld, Karolinska Institutet, Sweden; Karin Strandberg, Karolinska University Hospital & Karolinska Institutet, Sweden; Gabriella Galffy, Semmelweis University, Budapest, Hungary; M. Szentkereszty, Semmelweis University, Budapest, Hungary; Katherine M. Smith, University of Nottingham, UK; Lilla Tamasi, Semmelweis University, Budapest, Hungary; Bertrand De Meulder, University of Lyon, France; Diane Lefaudeux, University of Lyon, France.
The U-BIOPRED consortium wishes to acknowledge the help and expertise of the following individuals and groups without whom, the study would not have been possible.
Investigators and contributors: I.M. Adcock, Airways Disease Section, National Heart and Lung Institute, Imperial College London, London, UK; H. Ahmed, European Institute for Systems Biology and Medicine, University of Lyon, France; D. Allen, North West Severe Asthma Network, Pennine Acute Hospital NHS Trust; C. Auffray, European Institute for Systems Biology and Medicine, University of Lyon, France; P. Badorrek, Fraunhofer ITEM; S. Ballereau, European Institute for Systems Biology and Medicine, University of Lyon, France; A.T. Bansal, Acclarogen Ltd, St John's Innovation Centre, Cambridge, UK; A.F. Behndig, Umeå University; E.H. Bel, Dept of Respiratory Medicine, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; A. Berglind, Karolinska University Hospital & Karolinska Institutet; A. Berton, Boehringer Ingelheim Pharma GmbH & Co. KG; J. Bigler, Amgen Inc.; H. Bisgaard, Copenhagen Prospective Studies on Asthma in Childhood, Faculty of Health and Medical Sciences, University of Copenhagen and Gentofte Hospital, University of Copenhagen, Copenhagen, Denmark; M.J. Boedigheimer, Amgen Inc.; P. Brinkman, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; E. Bucchioni, Chiesi Pharmacueticals SPA, Parma, Italy; A. Bush, Dept of Paediatrics and National Heart and Lung Institute, Imperial College, London, Dept of Respiratory Paediatrics, Royal Brompton Hospital, London, UK; K. Bønnelykke, University of Copenhagen and Danish Pediatric Asthma Center, Gentofte Hospital, University of Copenhagen, Denmark; A. Chaiboonchoe, European Institute for Systems Biology and Medicine, University of Lyon, France; D. Campagna, University of Catania; M. Caruso, Dept of Clinical and Experimental Medicine Hospital University, University of Catania, Italy; C. Casaulta, University Children's Hospital Bern, Switzerland; P. Chanez, Département des Maladies Respiratoires, Laboratoire d'immunologie, Aix Marseille Université Marseille, France; K.F. Chung, Imperial College, London, UK; C.H. Compton, GSK, Stockley Park, UK; J. Corfield, AstraZeneca R&D Mölndal, Sweden and Areteva R&D, Nottingham, UK; S.E. Dahlen, The Centre for Allergy Research, The Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden; B. Dahlén, Lung/Allergy Clinic, Karolinska University Hospital Huddinge, Stockholm, Sweden; B. De Meulder, European Institute for Systems Biology and Medicine, University of Lyon, France; I. Delin, Institute of Environmental Medicine, Karolinska Instituet, Stockholm, Sweden; P. Dennison, NIHR Southampton Respiratory Biomedical Research Unit, Clinical and Experimental Sciences, NIHR-Wellcome Trust Clinical Research Facility, Faculty of Medicine, University of Southampton, UK; R. Djukanovic, Southampton NIHR Respiratory Biomedical Research Unit, Southampton University Hospital, Southampton, UK; K. Dyson, CROMSOURCE, Shrewsbury, UK; L. El Hadjam, European Institute for Systems Biology and Medicine, University of Lyon, France; V.J. Erpenbeck, Translational Medicine, Respiratory Profiling, Novartis Institutes for BioMedical Research, Basel, Switzerland; D. Erzen, Boehringer Ingelheim Pharma GmbH & Co. KG; C. Faulenbach, Fraunhofer ITEM; K. Fichtner, Boehringer Ingelheim Pharma GmbH & Co. KG; N. Fitch, BioSci Consulting, Belgium; L.J. Fleming, National Heart and Lung Institute, Imperial College, London, UK; E. Formaggio, CROMSOURCE, Verona, Italy; S.J. Fowler, Centre for Respiratory Medicine and Allergy, The University of Manchester, Manchester Academic Health Science Centre, University Hospital of South Manchester NHS Foundation Trust, Manchester, UK, and Airways Clinic, Lancashire Teaching Hospitals NHS Foundation Trust, Preston, UK; U. Frey, University Children's Hospital Basel, Basel, Switzerland; M. Gahlemann, Boehringer Ingelheim (Schweiz) GmbH; G. Galffy, Semmelweis University, Budapest, Hungary; D. Garissi, Global Head Clinical Research Division, CROMSOURCE, Italy; T. Garret, BioSci Consulting, Belgium; T. Geiser, University Hospital Bern, Switzerland; J. Gent, Royal Brompton and Harefield NHS Foundation Trust; M. Gerhardsson de Verdier, AstraZeneca R&D Mölndal, Medical Evidence and Observational Research Centre, Mölndal, Sweden; C. von Garnier, University Hospital Bern, Tiefenau Hospital Bern, Switzerland; D. Gibeon, National Heart and Lung Institute, Imperial College, London, UK; E. Guillmnt-Farry, Royal Brompton and Harefield NHS Foundation Trust, UK; Y. Guo, Data Science Institute/Discovery Sciences Group, Hammersmith Hospital Campus, Imperial College London, UK; S. Hashimoto, Dept of Respiratory Medicine, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; G. Hedlin, Dept of Women's and Children's Health and Center for Allergy research, Karolinska Institutet, Karolinska University Hospital, Stockholm, Sweden; P.W. Hekking, Dept of Respiratory Medicine, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; E. Henriksson, Karolinska Institutet; T. Higenbottam, Allergy Therapeutics, West Sussex, UK; U. Hoda, Imperial College; J.M. Hohlfeld, Fraunhofer ITEM; I. Horváth, Dept of Pulmonology, Semmelweis University, Budapest, Hungary; P. Howarth, Southampton NIHR Respiratory Biomedical Research Unit, Southampton University Hospital, Southampton, UK; X. Hu, Amgen Inc.; A. James, Karolinska Institutet; E. Jeyasingham, UK Clinical Operations, GSK, Stockley Park, UK; K. Johnston, University of Manchester, UK; N. Jullian, European Institute for Systems Biology and Medicine, University of Lyon, France; G. Kerry, University of Manchester, UK; M. Klüglich, Boehringer Ingelheim Pharma GmbH & Co. KG; A.J. Knox, Respiratory Research Unit, University of Nottingham, Nottingham, UK; J.R. Konradsen, Karolinska University Hospital & Karolinska Institutet; L. Krueger, University Children's Hospital Bern, Switzerland; N. Krug, Fraunhofer Institute for Toxicology and Experimental Medicine Hannover, Germany; A-S. Lantz, Karolinska University Hospital & Karolinska Institutet; L.X. Larsson, AstraZeneca R&D, Mölndal, Sweden; P. Latzin, University Children's Hospital Bern, Bern, Switzerland; N. Lazarinis, Lung/Allergy Clinic, Karolinska University Hospital Huddinge, Stockholm, Sweden; D. Lefaudeux, European Institute for Systems Biology and Medicine, University of Lyon, France; N. Lemonnier, European Institute for Systems Biology and Medicine, University of Lyon, France; L.A. Lowe, University of Manchester, UK; R. Lutter, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; A. Mazein, European Institute for Systems Biology and Medicine, University of Lyon, France; L. McEvoy, University Hospital, Dept of Pulmonary Medicine, Bern, Switzerland; A. Menzies-Gow, Royal Brompton and Harefield NHS Foundation Trust; R.J.M. Middelveld, Karolinska Institutet; P. Montuschi, Faculty of Medicine, Catholic University of the Sacred Heart, Rome, Italy; N. Mores, Università Cattolica del Sacro Cuore; C.S. Murray, Centre for Respiratory Medicine and Allergy, The University of Manchester, Manchester Academic Health Science Centre, University Hospital of South Manchester NHS Foundation Trust, Manchester, UK; J. Musial, Dept of Medicine, Jagiellonian University Medical College, Krakow, Poland; D. Myles, Respiratory Therapy Area Unit, GlaxoSmithKline, Stevenage, Hertfordshire, UK; K. Nething, Boehringer Ingelheim Pharma GmbH & Co. KG; U. Nihlén, Dept of Respiratory Medicine and Allergology, Skåne University Hospital, Lund, Sweden, and AstraZeneca R&D, Mölndal, Sweden; R. Niven, North West Severe Asthma Network, University Hospital South Manchester NHS Trust; B. Nordlund, Astrid Lindgren Children's Hospital, Karolinska University Hospital, Stockholm, Sweden, and Dept of Women's and Children's Health, Karolinska Institutet, Stockholm, Sweden; S. Nsubuga, Royal Brompton and Harefield NHS Foundation Trust; L. Pahus, Assistance publique des Hôpitaux de Marseille, Hôpital NORD, Clinique des bronches, allergies et sommeil, Marseille, France; I. Pandis, Imperial College, London, UK; J. Pellet, European Institute for Systems Biology and Medicine, University of Lyon, France; C. Pison, European Institute for Systems Biology and Medicine, University of Lyon, France; G. Praticò, CROMSOURCE, Verona, Italy; M. Puig Valls, CROMSOURCE, Barcelona, Spain; K. Riemann, Boehringer Ingelheim Pharma GmbH & Co. KG; G. Roberts, NIHR Southampton Respiratory Biomedical Research Unit, University Hospital Southampton NHS Foundation Trust, Southampton, UK, Clinical and Experimental Sciences and Human Development in Health Academic Unit, University of Southampton Faculty of Medicine, Southampton, UK, and The David Hide Asthma and Allergy Research Centre, St Mary's Hospital, Isle of Wight, UK; J.P. Rocha, Royal Brompton and Harefield NHS Foundation Trust; C. Rossios, Imperial College; A. Rowe, Janssen R&D Ltd, High Wycombe, UK; T. Sandström, Dept of Medicine, Respiratory and Allergy unit, University Hospital, Umeå, Sweden; G. Santini, Università Cattolica del Sacro Cuore; M. Saqi, European Institute for Systems Biology and Medicine, University of Lyon, France; S. Scott, North West Severe Asthma Network, Countess of Chester NHS Trust; N. Sehgal, North West Severe Asthma Network, Pennine Acute Hospital NHS Trust; W. Seibold, Boehringer Ingelheim Pharma GmbH & Co.; D.E. Shaw, Respiratory Research Unit, University of Nottingham, Nottingham, UK; R. Sigmund, Boehringer Ingelheim Pharma GmbH & Co. KG; F. Singer, University Children's Hospital Zurich, Zurich, Switzerland; A. Sogbesan, Royal Brompton and Harefield NHS Foundation Trust; A.R. Sousa, Respiratory Therapeutic Unit, GlaxoSmithKline, Stockley Park, UK; P. Söderman, Karolinska University Hospital & Karolinska Institutet; F. Spycher, University Hospital, Dept of Pulmonary Medicine, Bern, Switzerland; S. Stephan, University of Manchester, UK; P.J. Sterk, Dept Respiratory Medicine, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; J. Stokholm, University of Copenhagen and Danish Pediatric Asthma Center, Gentofte Hospital, University of Copenhagen, Denmark; K. Strandberg, Lung/Allergy Clinic, Karolinska University Hospital Huddinge, Stockholm, Sweden; S. Sunthar, University of Manchester, UK; M. Szentkereszty, Semmelweis University, Budapest, Hungary; L. Tamasi, Semmelweis University, Budapest, Hungary; K. Tariq, NIHR Southampton Respiratory Biomedical Research Unit, Clinical and Experimental Sciences, NIHR-Wellcome Trust Clinical Research Facility, Faculty of Medicine, University of Southampton, UK; S. Valente, Università Cattolica del Sacro Cuore; W.M. van Aalderen, Dept of Paediatric Respiratory Medicine and Allergy, Emma Children's Hospital, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; C.M. van Drunen, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; J. Vestbo, Respiratory Research Group, Manchester Academic Health Science Centre, University Hospital South Manchester NHS Foundation Trust, Manchester, UK; N.H. Vissing, Copenhagen Prospective Studies on Asthma in Childhood, Faculty of Health and Medical Sciences, University of Copenhagen and Gentofte Hospital, University of Copenhagen, Copenhagen, Denmark; A. Vyas, North West Severe Asthma Network, Lancashire Teaching Hospitals NHS Trust; A.H. Wagener, Dept of Respiratory Medicine, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; S.S. Wagers, BioSci Consulting, Belgium; S.J. Wilson, Clinical and Experimental Sciences Academic Unit, University of Southampton Faculty of Medicine, Southampton, UK; W. Yu, Amgen Inc.; W. Zetterquist, Dept of Woman and Child Health, Karolinska Institutet, Stockholm, Sweden; Z. Zolkipli, NIHR Southampton Respiratory Biomedical Research Unit, University Hospital Southampton NHS Foundation Trust, Southampton, UK, Clinical and Experimental Sciences and Human Development in Health Academic Unit, University of Southampton Faculty of Medicine, Southampton, UK, and The David Hide Asthma and Allergy Research Centre, St Mary's Hospital, Isle of Wight, UK; A.H. Zwinderman, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands.
Partner organisations: Novartis Pharma AG; University of Southampton, Southampton, UK; Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands; Imperial College London, London, UK; University of Catania, Catania, Italy; University of Rome ‘Tor Vergata’, Rome, Italy; Hvidore Hospital, Hvidore, Denmark; Jagiellonian Univ. Medi.College, Krakow, Poland; University Hospital, Inselspital, Bern, Switzerland; Semmelweis University, Budapest, Hungary; University of Manchester, Manchester, UK; Université d'Aix-Marseille, Marseille, France; Fraunhofer Institute, Hannover, Germany; University Hospital, Umea, Sweden; Ghent University, Ghent, Belgium; Ctr. Nat. Recherche Scientifique, Villejuif, France; Università Cattolica del Sacro Cuore, Rome, Italy; University Hospital, Copenhagen, Denmark; Karolinska Institutet, Stockholm, Sweden; Nottingham University Hospital, Nottingham, UK; University of Bergen, Bergen, Norway; Netherlands Asthma Foundation, Leusden, NL; European Lung Foundation, Sheffield, UK; Asthma UK, London, UK; European Fed. of Allergy and Airways Diseases Patients’ Associations, Brussels, Belgium; Lega Italiano Anti Fumo, Catania, Italy; International Primary Care Respiratory Group, Aberdeen, Scotland; Philips Research Laboratories, Eindhoven, NL; Synairgen Research Ltd, Southampton, UK; Aerocrine AB, Stockholm, Sweden; BioSci Consulting, Maasmechelen, Belgium; Almirall; AstraZeneca; Boehringer Ingelheim; Chiesi; GlaxoSmithKline; Roche; UCB; Janssen Biologics BV; Amgen NV; Merck Sharp & Dohme Corp.
Third Parties to the project, contributing to the clinical trial: Academic Medical Centre (AMC), Amsterdam (In the U-BIOPRED consortium the legal entity is AMC Medical Research BV (AMR); AMR is a subsidiary of both AMC and the University of Amsterdam; AMC contribute across the U-BIOPRED project); University Hospital Southampton NHS Trust (third party of the University of Southampton and contributor to the U-BIOPRED clinical trial); South Manchester Healthcare Trust (third party to the University of Manchester, South Manchester Healthcare Trust, contributor to the U-BIOPRED clinical trial and to the U-BIOPRED Biobank); Protisvalor Méditerranée SAS (third party to University of the Mediterranean; contributor to the U-BIOPRED clinical trial); Karolinska University Hospital (third party Karolinska Institutet (KI), contributor to the U-BIOPRED clinical trial); Nottingham University Hospital (third party to University of Nottingham, contributor to the U-BIOPRED clinical trial); NIHR-Wellcome Trust Clinical Research Facility.
Members of the ethics board: Jan-Bas Prins, biomedical research, LUMC, the Netherlands; Martina Gahlemann, clinical care, BI, Germany; Luigi Visintin, legal affairs, LIAF, Italy; Hazel Evans, paediatric care, Southampton, UK; Martine Puhl, patient representation (co-chair), NAF, the Netherlands; Lina Buzermaniene, patient representation, EFA, Lithuania; Val Hudson, patient representation, Asthma UK; Laura Bond, patient representation, Asthma UK; Pim de Boer, patient representation and pathobiology, IND; Guy Widdershoven, research ethics, VUMC, the Netherlands; Ralf Sigmund, research methodology and biostatistics, BI, Germany.
The patient input platform: Amanda Roberts, UK; David Supple (chair), UK; Dominique Hamerlijnck, The Netherlands; Jenny Negus, UK; Juliёtte Kamphuis, The Netherlands; Lehanne Sergison, UK; Luigi Visintin, Italy; Pim de Boer (co-chair), The Netherlands; Susanne Onstein, The Netherlands.
Members of the safety monitoring board: William MacNee, clinical care; Renato Bernardini, clinical pharmacology; Louis Bont, paediatric care and infectious diseases; Per-Ake Wecksell, patient representation; Pim de Boer, patient representation and pathobiology (chair); Martina Gahlemann, patient safety advice and clinical care (co-chair); Ralf Sigmund, bio-informatician.
Footnotes
This article has supplementary material available from erj.ersjournals.com
This study is registered on ClinicalTrials.gov (identifier: NCT01982162).
Support statement: This paper is presented on behalf of the U-BIOPRED Study Group with input from the U-BIOPRED Patient Input Platform, Ethics Board and Safety Management Board. U-BIOPRED is supported through an Innovative Medicines Initiative Joint Undertaking under grant agreement no. 115010, resources of which are composed of financial contribution from the European Union's Seventh Framework Programme (FP7/2007–2013) and EFPIA companies’ in kind contribution (www.imi.europa.eu). We would also like to acknowledge help from the IMI funded eTRIKS project (EU Grant Code No.115446). Funding information for this article has been deposited with FundRef.
Conflict of interest: Disclosures can be found alongside the online version of this article at erj.ersjournals.com
- Received May 18, 2015.
- Accepted July 3, 2015.
- Copyright ©ERS 2015
References










