





Abstract
Bronchiectasis is being diagnosed increasingly in children and adolescents. Recurrent respiratory exacerbations are common in children and adolescents with this chronic pulmonary disorder. Respiratory exacerbations are associated with an impaired quality of life, poorer long-term clinical outcomes, and substantial costs to the family and health systems. The 2021 European Respiratory Society (ERS) clinical practice guideline for the management of children and adolescents with bronchiectasis provided a definition of acute respiratory exacerbations for clinical use but to date there is no comparable universal definition for clinical research. Given the importance of exacerbations in the field, this ERS Task Force sought to obtain robust definitions of respiratory exacerbations for clinical research. The panel was a multidisciplinary team of specialists in paediatric and adult respiratory medicine, infectious disease, physiotherapy, primary care, nursing, radiology, methodology, patient advocacy, and parents of children and adolescents with bronchiectasis. We used a standardised process that included a systematic literature review, parent survey, and a Delphi approach involving 299 physicians (54 countries) caring for children and adolescents with bronchiectasis. Consensus was obtained for all four statements drafted by the panel as the disagreement rate was very low (range 3.6–7.2%). The panel unanimously endorsed the four consensus definitions for 1a) non-severe exacerbation and 1b) severe exacerbation as an outcome measure, 2) non-severe exacerbation for studies initiating treatment, and 3) resolution of a non-severe exacerbation for clinical trials involving children and adolescents with bronchiectasis. This ERS Task Force proposes using these internationally derived, consensus-based definitions of respiratory exacerbations for future clinical paediatric bronchiectasis research.
Abstract
This ERS Task Force statement developed internationally derived, consensus-based definitions of respiratory exacerbations for future clinical paediatric bronchiectasis research https://bit.ly/3sqT2YP
Introduction
Bronchiectasis is a chronic pulmonary disorder, which is used as an umbrella term to describe a clinical syndrome of recurrent or persistent wet/productive cough and lower airway infection and/or inflammation, accompanied by abnormal bronchial dilatation detected by chest computed tomography (CT) scans [1]. Previously considered inevitably progressive, it is now accepted that bronchiectasis in children and adolescents may be reversible over time if detected early in the course of the disease and treated effectively [1, 2].
Bronchiectasis is associated with a high symptom burden [3], and increased patient needs [4] and treatment costs [5, 6]. It remains one of the most neglected pulmonary disorders [7], especially in children [8], and has marked inequity compared with other chronic pulmonary diseases [9, 10]. The need for better health services and clinical research for improving the lives and outcomes of children and adolescents with bronchiectasis, as well as the wellbeing of families, was highlighted by an international parent/patient survey on clinical needs led by the European Lung Foundation (ELF) [4]. Several aspects of acute respiratory exacerbations featured prominently in the ELF survey [4].
Similar to other chronic pulmonary disorders, recurrent acute respiratory (pulmonary) exacerbations (“attacks” or “flare-ups”) are common in people with bronchiectasis. Exacerbations are particularly important in children and adolescents with bronchiectasis as they are associated with increased respiratory symptoms, impaired quality of life (QoL) [11], accelerated lung function decline (−1.9% forced expiratory volume in 1 s (FEV1) predicted per hospitalised exacerbation) [12], and high healthcare resource use [13] and costs (AUD 30 182 (EUR 20 800/GBP 17 040) per hospitalisation in 2016 in Australia [6]). Also, children and adolescents with bronchiectasis have high healthcare attendance and high rates of antibiotic consumption and school/childcare absences due to bronchiectasis exacerbations (30, 50 and 24.9 episodes per 100 person-months of observation, respectively) [13]. Importantly, patients and parents responding to the ELF survey rated exacerbations among the top three factors affecting their child's QoL [4].
Thus, it is unsurprising that parents and the panel designated exacerbations as a critical outcome measure for all the key questions in the 2021 European Respiratory Society (ERS) clinical practice guidelines (CPG) for the management of children and adolescents with bronchiectasis [2]. While the CPG recommendations include a definition of exacerbations for clinical use [2], there is currently no consensus on a definition of exacerbations for paediatric bronchiectasis research, although a definition for adult bronchiectasis is available [14]. Therefore, there is a need to obtain robust and patient/parent-informed definitions of respiratory exacerbations for clinical research relevant for paediatric bronchiectasis. For this document, the definition of bronchiectasis is the same as the one used in the ERS CPG for the management of children and adolescents with bronchiectasis [2], i.e. a clinical syndrome of recurrent or persistent wet/productive cough, airway infection and inflammation, and abnormal bronchial dilatation on chest CT scans.
This ERS Task Force statement reviewed the current literature on defining respiratory exacerbations in children and adolescents with bronchiectasis. This Task Force statement on the definition of exacerbations for clinical trials in children and adolescents with bronchiectasis presents an international consensus view, using a Delphi approach on statements formulated after the panel evaluated the systematic review and parents’ survey.
Methods
The current statement, developed by an ERS Bronchiectasis Task Force, included specialists in paediatric respiratory medicine with expertise in managing children and adolescents with bronchiectasis as well as paediatric experts in infectious disease, radiology, physiotherapy and nursing, two global leaders in adult bronchiectasis, the Cochrane Airways Group coordinating editor (also a primary care physician), ELF representatives, and representatives of the bronchiectasis/protracted bacterial bronchitis-specific parent/patient advisory group (PAG) members. Conflicts of interest were declared at commencement of this project and prior to the final submission, and managed in accordance with ERS policies. At the first meeting, the panel agreed on the overall approach (figure 1), and both inclusion and exclusion criteria (supplementary material).
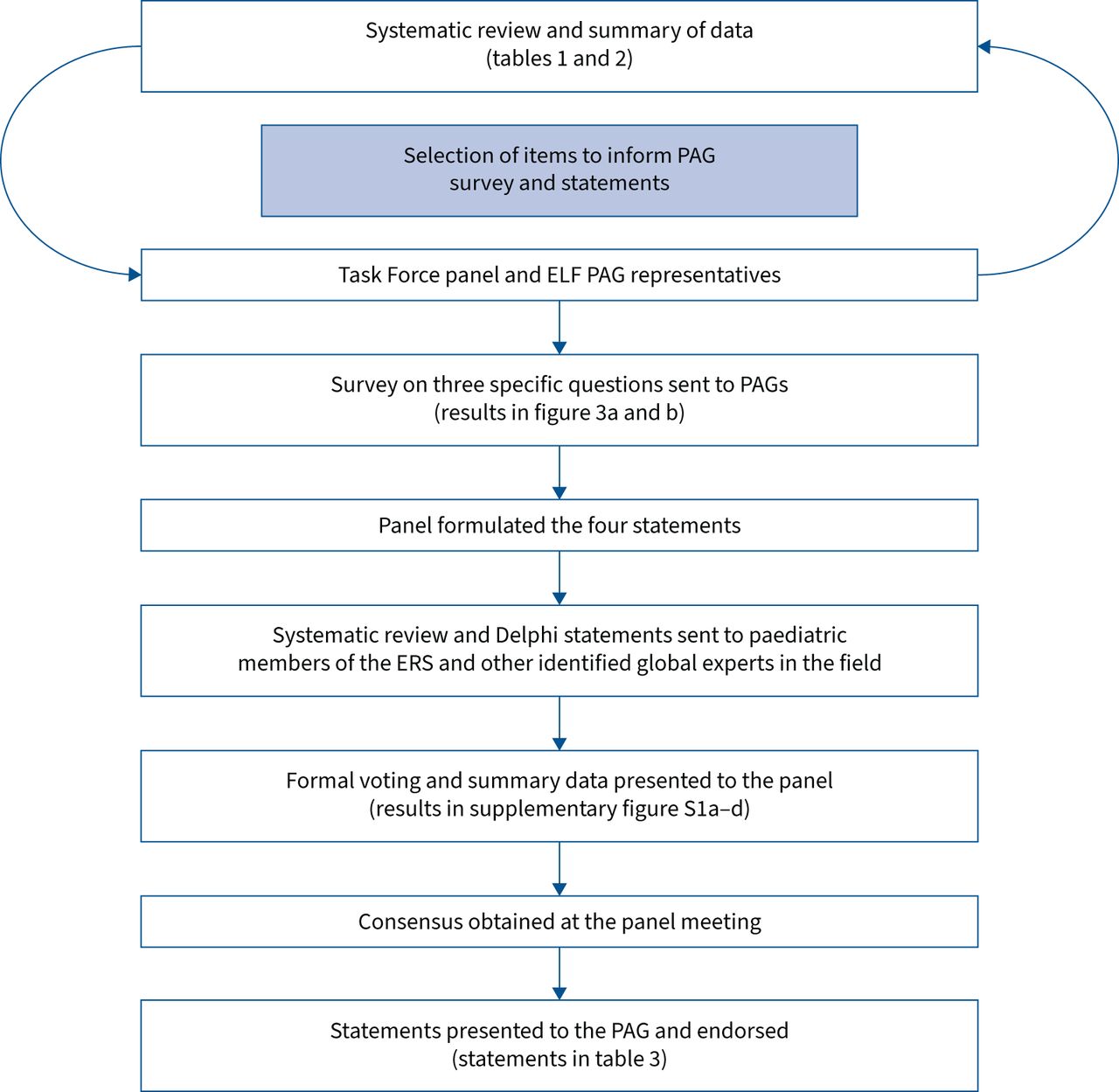
Schematic overview of the methodology used to develop the consensus for the definitions of exacerbations. PAG: patient advisory group; ELF: European Lung Foundation; ERS: European Respiratory Society.
Systematic review and PAGs survey
The Cochrane Airways Group information specialist designed and ran the search on 22 February 2021 using the search strategy outlined in the supplementary material. Search results were uploaded onto Rayyan (https://rayyan.qcri.org). Two panel members (V.G. and A.Z.) independently screened the abstracts. The papers were retrieved and reviewed by same two panel members and a third reviewer (A.C.) who also summarised the studies. Additional papers and protocol registries were identified from authors’ databases. Disagreements were resolved by consensus. A PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram showing the total number of articles found in the search, including those that were subsequently included/excluded, is shown in figure 2.

PRISMA diagram outlining the selection of studies. RCT: randomised controlled trial; PCD: primary ciliary dyskinesia.
The ELF lead (J.B.) sent a survey (using SurveyMonkey (www.surveymonkey.co.uk); from 11 March 2021 to 16 April 2021) to two PAGs (CPG [2] and Brisbane parent advisory groups (www.crelungs.org.au/cre-parent-and-community-advisory-group)) on three specific questions (two on symptoms/signs and one on duration) relating to defining an acute respiratory exacerbation of bronchiectasis in their child (figures 3a and b). The first question had 16 items and the second 25 items. The third question was “Overall, how long do you think the items listed need to be present before you would consider there is a non-severe (non-hospitalised) exacerbation episode present?”. Data were then summarised by the ELF panel member (J.B.) and presented to the Task Force panel.

{kind=link}
{kind=link}
{kind=link}
The parent advisory groups’ responses to the questions posed in the survey undertaken by the European Lung Foundation (ELF). a) Question 1: Which items do you think should be part of defining an acute respiratory exacerbation in a child or a young person with bronchiectasis? Options: 1=not important; 2=slightly important; 3=moderately important; 4=very important and 5=essential. All but one item rated between 4 (very important) and 5 (essential). Most important: “Change in chest X-ray”, “Advised to start antibiotics”, “Breathless at rest” and “Decline in lung function”. b) Question 2: How long do you think these items need to be present before you would consider this is an acute exacerbation episode? Options: 1, 2, 3, 4, 5, 6 and <7 days. 1 day: “Coughing up blood”; 1–1.5 days: “Blue tongue or lips”, “Finding harder to breathe than normal”, “More rapid breaths than normal”, “Breathless at rest”, “Chest pain” and “Fever >38 degrees centigrade”; all items: between 1 and 4 days. #: additional comments made by some respondents; we have not included these comments in the document. Mean values are indicated in red.
Development of consensus
Between January and December 2021, the panel held three virtual meetings in addition to corresponding by e-mail between meetings. The overall methods were re-presented at these further meetings and the panel agreed on the final overall approach (figure 1), including predetermining that consensus would be considered achieved if ≥80% agreed with the statements.
The panel reviewed the data from the systematic review and the PAG survey. Discussions were held based on these data and draft consensus statements modified until all the panel members agreed on all four statements. These four statements defined: 1) exacerbation as an outcome for clinical trials (allowing categorisation into 1a) non-severe and 1b) severe exacerbations), 2) a non-severe exacerbation that warrants treatment in clinical trial settings, and 3) the resolution of a non-severe exacerbation. These statements (using SurveyMonkey) were then circulated to the ERS paediatric assembly members and other global bronchiectasis experts known to the authors and their networks (e.g. the Australian National Health and Medical Research Council Centre for Research Excellence for Paediatric Bronchiectasis). Only data from physicians who cared for children with bronchiectasis were included in the survey that was open for 2 months (1 September 2021 to 31 October 2021). The survey results were reviewed by the Task Force, and the consensus statements were adapted and finalised by the panel. Lastly, these statements were presented to the ELF PAG for final review and endorsement.
Results
The search identified 1079 potential publications; 38 full-text articles were retrieved (from the search data) with an additional five papers identified from references in these articles and from other sources. 21 studies fulfilled the inclusion criteria (table 1 and figure 2). The key aspects of the 21 studies of various types (grouped by studies treating an exacerbation, studies with exacerbation as an outcome and consensus documents) are tabulated in table 1. Two studies involved treatment of exacerbations, while two were consensus documents, one was a guideline and in the rest (n=16), exacerbations were an outcome. The combined data from these studies and the indicators used to define an exacerbation are summarised in table 2.
Studies on pulmonary exacerbation in children and adolescents with bronchiectasis (BE), grouped by studies on treatment of exacerbations, studies where exacerbations were an outcome and consensus statements
Summary of indicators of bronchiectasis exacerbations in the included studies (n=21)
Two studies aimed to define exacerbations: one [15] was retrospective and the second [16] was a prospective study where blood markers were also included. Using symptom duration to define a non-severe exacerbation was mentioned in 11 (52.5%) studies. In all but one study, the duration was ≥3 days.
From the 21 included studies, there was no universal definition. The most common indicator used to define an exacerbation was “change in cough frequency or character (dry to wet)”, used in 17 (81%) studies. The other four most common indicators were: “change in sputum colour or volume”, “breathlessness/dyspnoea”, “change in auscultatory findings” and “new chest radiography findings” (table 2).
In the PAG survey, for Question 1, “Change in chest X-ray” and “Advised to start antibiotics” were the two highest (of 16 items) ranked items. All but one item was ranked as very important or essential (i.e. a mean score of ≥4) (figure 3a). In Question 2, the PAGs considered 22 of the 25 listed items needed to be present for ≤3 days (figure 3b). When considering overall symptom duration that needs to be present when defining the occurrence of a non-severe (non-hospitalised) exacerbation, none indicated that symptoms should be any longer than “At least 3 days”.
The physicians’ survey had 348 respondents, of whom 49 were disqualified as they either did not care for children and adolescents or did not complete the survey questions. The remaining 299 physicians were from 54 countries; 89% (n=266) were paediatric respiratory specialists, of whom 77% practiced in a university-based setting, and most (67%) cared for ≥10 children and adolescents with bronchiectasis.
The physicians’ Delphi achieved our predefined consensus rate at the first iteration with a high agreement rate (“strongly agree” or “agree”) ranging from 82.3% to 92.9% for the four statements. The disagreement rate (“strongly disagree” or “disagree”) ranged from 3.6% to 7.2% and the “neither agree or disagree” rate was between 3.3% and 11.5%. The full data are presented in supplementary figure S1a–d. The panel unanimously endorsed these statements at the final virtual meeting (table 3). Likewise, the ELF PAG also endorsed the four statements.
Defining respiratory exacerbations in children and adolescents with bronchiectasis for clinical research
Discussion
This ERS Task Force document on defining respiratory exacerbations for paediatric bronchiectasis clinical research is the first such consensus document. The multidisciplinary international Task Force panel formulated four statements based upon the 21 included studies identified in the systematic review, our collective clinical research experience and the opinion of the PAGs on defining respiratory exacerbations of paediatric bronchiectasis. We had a high agreement rate (>82%) on the Delphi survey, undertaken by 299 physicians (from 54 countries) who care for children and adolescents with bronchiectasis, on all four statements.
Exacerbations are used widely as either an outcome variable or an analysed end-point measure for intervention studies in chronic airway diseases. These include clinical trials involving children and adolescents with asthma [17], cystic fibrosis [18] or bronchiectasis [19]. Having standardised definitions for exacerbations will help with reducing heterogeneity in patient and physician behaviour, therefore allowing a better comparison between trials aiming to reduce exacerbation frequency. However, our systematic review undertaken for this Task Force document showed that despite some common features, such as increased cough and/or sputum production, there was wide variation in the definitions of exacerbations used in previous studies (table 1). As different aspects of exacerbations are examined in clinical studies, this Task Force statement includes different definitions for the various scenarios that will be encountered. This means the definition of an exacerbation employed as an outcome measure for intervention trials (e.g. a multicentre randomised controlled trial seeking to reduce exacerbations [19]) differs from that when the intervention is used to assess treatment of exacerbations themselves (e.g. as in two recent multicentre randomised controlled trials of antibiotics [20, 21]). Defining resolution of exacerbation is also required, not only for studies assessing treatment of exacerbations, but also to determine when another exacerbation commences if two exacerbations occur closely together. Thus, the panel included Statement 3 as part of this Task Force document.
Although the statements in this Task Force document share common features with the recommendation in the paediatric bronchiectasis CPG [2], there are also important differences between the two ERS documents. The CPG focused on a definition for clinical care rather than research, and was a single statement advocating for prompt and optimal treatment of exacerbations. In contrast, the present Task Force statements include four different definitions to align with the particular study objectives (exacerbations as an outcome, to initiate treatment or its resolution). The differences between the definitions for clinical and research purposes are expected as the clinical definition focuses upon prompt recognition, while the research definition promotes robustness of outcome variables for research. While both Task Forces utilised a rigorously conducted systematic review, the present Task Force methods included a Delphi approach that encompassed worldwide expert physicians in the field.
Our statement differs from the adult statement for clinical research [14], which was led by one of our panel members (A.T.H.). The adult group defined an exacerbation as “a person with bronchiectasis with a deterioration in three or more of the following key symptoms for at least 48 h: cough; sputum volume and/or consistency; sputum purulence; breathlessness and/or exercise tolerance; fatigue and/or malaise; haemoptysis AND a clinician determines that a change in bronchiectasis treatment is required” [14]. Despite the similarities between the clinical research definition for adults [14] and Statement 1a (table 3) of our Task Force, there are also differences in the duration of symptoms, types of symptoms required and our categorisation of severe versus non-severe exacerbations. Our Task Force paid particular attention to the duration of symptoms, with robust discussions during our meetings and by e-mail. Based upon the systematic review we undertook (tables 1 and 2), and PAG advice, we chose at least 3 days (rather than the 2 days used for adults [14]). The surveyed international physician community with specific expertise in paediatric bronchiectasis supported this decision with an agreement rate of 88.7% (disagreement rate of 6.4% with 5% indicating “neither agree or disagree“) on the Delphi statement. Overall, we considered 2 days was too short in children, as the cough may spontaneously improve without the need for any intervention. This element is included to avoid over-prescribing of antibiotics when they may not be necessary.
The above is also not surprising as while bronchiectasis in children and adolescents shares some similarities with adults (e.g. wet/productive cough being the dominant symptom with exacerbation periods), there are also substantial differences. Acute respiratory infections are more common in younger children than in adults [22], and haemoptysis in children and adolescents with bronchiectasis is rare [1] compared with its incidence in adults. Also, children require parental care, support and input, and are clearly cognitively different from adults, whereby paediatricians mostly rely upon parent report while adults self-report. In children and dependent adolescents, the burden of illness from bronchiectasis is not just on the patient (i.e. the child) but also the entire family. Biologically, differences between paediatric- and adult-based studies include significantly dissimilar pathogen profiles (bacterial [23] and complex microbial community compositions [24]), age-related immunological responses [25] and likely outcomes of treatment [1].
In this Task Force document, our paediatric definition of pulmonary exacerbation includes “Onset of new or worsening radiographic changes (e.g. chest radiography)”. While this document refers to recommended definitions for clinical research, we acknowledge that in clinical practice it can on occasions be difficult differentiating community-acquired pneumonia from atelectasis and other chest radiography changes related to pulmonary exacerbations of bronchiectasis. In our ERS CPG for the management of children and adolescents with bronchiectasis [2], we did not differentiate between pneumonia and a pulmonary exacerbation.
Bronchiectasis unrelated to cystic fibrosis has gained prominence in the last decade with the increasing recognition that is not as rare as once believed [1, 26]. There is now increasing traction in the field of paediatric bronchiectasis with the establishment of an ERS Clinical Research Collaboration (Child-BEAR-Net [27]) and an Australian National Health and Medical Research Council Centre for Research Excellence in Paediatric Bronchiectasis (AusBREATHE [28]). However, we have a considerable journey ahead to achieve equity for children and adolescents with bronchiectasis and to improve their outcomes.
Conclusions
This ERS Task Force document proposes the internationally derived, systematically evaluated, consensus-based definitions of respiratory exacerbations outlined in table 3. We hope it will contribute to the planning and help improve the quality of future clinical paediatric bronchiectasis research. We believe that our expert panel, combined with the opinion from parents of children and adolescents with bronchiectasis, have derived internationally applicable definitions of respiratory exacerbations for children and adolescents with bronchiectasis.
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-00300-2022.Shareable
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-00300-2022.Supplement
Supplementary figure S1 ERJ-00300-2022.Figure_S1
Acknowledgements
We thank Elizabeth Stovold, the information specialist from the Cochrane Airways Group (London, UK), for having undertaken all the searches. We are also grateful to the extended ELF PAG and the Australian National Health and Medical Research Council Centre for Research Excellence PAG who helped shape the document through sharing their experiences and views on exacerbations. Finally, we are grateful to the physicians who responded to the survey as without their input, we would not have been able to develop a Delphi approach.
Footnotes
This document was endorsed by the ERS Executive Committee on 2 May 2022.
Other Child-BEAR-Net committee members: James Chalmers, Andrew Collaro, Kostas Douros, Matthias Griese, Jonathan Grigg, Andreas Hector, Oleksandr Mazulov, Fabio Midulla, Alexander Möller, Marijke Proesmans and Stephanie Yerkovich.
Conflict of Interest: E. Alexopoulou, L. Bell, A. Bush, C. Constant, R. Fortescue, B. Karadag, A.T. Hill, A. Kantar, V. Goyal, A. Zacharasiewicz, J. Boyd, A. Claydon, Z. Powell and C. Wilson have nothing to disclose. A.B. Chang reports grants from National Health and Medical Research Council, Australia, during the conduct of the study; is IDMC member for an unlicensed vaccine (GSK), is advisory member of study design for an unlicensed molecule for chronic cough (Merck), and is IDMC member for an unlicensed monoclonal antibody (AstraZeneca); and has received personal fees from being an author of two UpToDate chapters, outside the submitted work. K. Grimwood reports grants from Australian National Health and Medical Research Council, and Medical Research Futures Fund, during the conduct of the study. S. Aliberti reports grants and personal fees from AstraZeneca, Insmed, Fisher & Paykel and Chiesi, and personal fees from GlaxoSmithKline, Gilead Sciences, Novartis, MENARINI, Fondazione Charta, Grifols, Boehringer Ingelheim and Zambon, outside the submitted work.
Support statement: This work was supported by the European Respiratory Society (grant: TF-2020-17) and the National Health and Medical Research Council (grant: 1170958). Funding information for this article has been deposited with the Crossref Funder Registry.
- Received February 9, 2022.
- Accepted April 4, 2022.
- Copyright ©The authors 2022. For reproduction rights and permissions contact permissions{at}ersnet.org
References










