





Abstract
Background Risk stratification plays an essential role in the management of patients with pulmonary arterial hypertension (PAH). The current European guidelines propose a three-stratum model to categorise risk as low, intermediate or high, based on the expected 1-year mortality. However, with this model, most patients are categorised as intermediate risk. We investigated a modified approach based on four risk categories, with intermediate risk subdivided into intermediate-low and intermediate-high risk.
Methods We analysed data from the Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension (COMPERA), a European pulmonary hypertension registry, and calculated risk at diagnosis and first follow-up based on World Health Organization functional class, 6-min walk distance (6MWD) and serum levels of brain natriuretic peptide (BNP) or N-terminal pro-BNP (NT-proBNP), using refined cut-off values. Survival was assessed using Kaplan–Meier analyses, log-rank testing and Cox proportional hazards models.
Results Data from 1655 patients with PAH were analysed. Using the three-stratum model, most patients were classified as intermediate risk (76.0% at baseline and 63.9% at first follow-up). The refined four-stratum risk model yielded a more nuanced separation and predicted long-term survival, especially at follow-up assessment. Changes in risk from baseline to follow-up were observed in 31.1% of the patients with the three-stratum model and in 49.2% with the four-stratum model. These changes, including those between the intermediate-low and intermediate-high strata, were associated with changes in long-term mortality risk.
Conclusions Modified risk stratification using a four-stratum model based on refined cut-off levels for functional class, 6MWD and BNP/NT-proBNP was more sensitive to prognostically relevant changes in risk than the original three-stratum model.
Abstract
COMPERA 2.0, a four-stratum risk assessment model based on refined cut-off levels for functional class, 6MWD and BNP/NT-proBNP was more sensitive to prognostically significant changes in risk than the original three-stratum model https://bit.ly/3mzPKjA
Introduction
Risk stratification has become an integral part of the management of patients with pulmonary arterial hypertension (PAH). The 2015 joint pulmonary hypertension (PH) guidelines of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS) proposed a multidimensional risk stratification model based on 14 variables derived from nine assessments [1, 2]. Based on this model, risk is divided into three strata as low, intermediate or high with estimated 1-year mortality rates <5%, 5–10% and >10%, respectively. Achieving and maintaining a low risk profile is recommended as treatment goal in patients with PAH [1–3].
Since publication of these guidelines, several registry-based studies showed that simplified versions of the ESC/ERS tool provided reliable prognostication. In particular, a combination of functional class, 6-min walk distance (6MWD) and brain natriuretic peptide (BNP) or N-terminal pro-BNP (NT-proBNP) was found to have strong prognostic value, both at the time of diagnosis and even more so at follow-up, i.e. after initiation of targeted therapies [4–6]. These variables were also the most reliable predictive parameters in the Lite-2 version of the Registry to Evaluate Early and Long-term PAH Disease Management (REVEAL) risk calculator, a risk stratification tool developed in the United States [7–9].
Several modalities have been developed to calculate individual risk. French investigators used a panel of noninvasive (functional class, 6MWD, BNP/NT-proBNP) and invasive (right atrial pressure, cardiac index) variables and summed up the number of variables meeting low risk criteria. They found that combined assessment of functional class, 6MWD and BNP/NT-proBNP had the highest prognostic value [4]. This strategy was confirmed by the Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension (COMPERA) investigators [10]. In both series, patients who met low risk criteria for all three variables (functional class I or II, 6MWD >440 m, BNP <50 ng·L−1 or NT-proBNP <300 ng·L−1) while on therapy had 5-year survival rates >90%. However, these criteria were met only by 9–19% of the patients [4, 10].
The Swedish Pulmonary Arterial Hypertension Registry (SPAHR) group and the COMPERA group used an alternative approach: based on the cut-off levels proposed in the ESC/ERS guidelines, each variable was graded from 1 to 3, where 1 defined low risk, 2 intermediate risk and 3 high risk. The mean value was calculated by dividing the sum of all grades by the number of variables [5, 6]. As the French group, the SPAHR and COMPERA groups included haemodynamics (right atrial pressure, cardiac index, mixed-venous oxygen saturation) in addition to World Health Organization functional class (WHO FC), 6MWD and BNP/NT-proBNP. In line with the French observations, the COMPERA investigators found that the noninvasive variables had a higher predictive value than the haemodynamic variables and showed that risk assessment based on the noninvasive variables alone provided good discrimination demonstrating significant survival differences between the risk groups [6].
Based on these studies, functional class, 6MWD and BNP/NT-proBNP have been established as key elements of current risk assessment tools in PAH. However, it was noted in the SPAHR and COMPERA analyses that most patients did not meet the low risk criteria while receiving PAH treatment. In fact, the majority of patients met intermediate risk criteria (∼70% at baseline and ∼60% at follow-up) [5, 6]. In these patients, a more granular risk prediction is required, in particular for far-reaching therapeutic decisions including the need for parenteral prostanoid therapy and evaluation for lung transplantation. Several investigators have shown that the use of additional variables derived from echocardiography, right heart catheterisation or blood gas analysis improved risk prediction [11–14]. As an alternative model, the SPAHR group recently proposed a modification of their original approach defining a calculated score of 1.5–1.99 as intermediate-low risk and a score of 2.0–2.4 as intermediate-high risk [15]. This approach showed promising results with further discrimination within the intermediate risk group, albeit based on a relatively small sample size.
We hypothesised that a subdivision into four risk strata (low, intermediate-low, intermediate-high, and high) based on more granularity within the cut-off levels of 6MWD, WHO FC and BNP/NT-proBNP might improve risk stratification. Here, we used the COMPERA database to investigate a refined risk stratification model (COMPERA 2.0) using modified cut-off levels, some of which have been proposed recently by the REVEAL group [7].
Methods
Database
Details of COMPERA (www.COMPERA.org; registered at clinicaltrials.gov with identifier NCT01347216) have been reported in previous communications [16, 17]. In summary, COMPERA is an ongoing PH registry launched in 2007 that prospectively collects baseline, follow-up and outcome data of patients who receive targeted therapies for any form of PH. Patients are enrolled within 6 months after PH diagnosis to ensure inclusion of newly diagnosed patients only. PH centres from several European countries participate (Austria, Belgium, Germany, Greece, Hungary, Italy, Latvia, Lithuania, the Netherlands, Slovakia, Switzerland, United Kingdom), with ∼80% of the enrolled patients coming from Germany.
COMPERA has been approved by the ethics committees of all participating centres, and all patients provided written informed consent prior to inclusion.
Patients
For the present analysis, patients were selected from the COMPERA database by the following criteria. 1) Treatment-naïve patients aged ≥18 years newly diagnosed with any form of PAH between 1 January 2009 and 31 December 2020; 2) at least one follow-up available; 3) baseline haemodynamics showing mean pulmonary arterial pressure ≥25 mmHg, pulmonary arterial wedge pressure ≤15 mmHg and pulmonary vascular resistance >3 Wood units (240 dyn·s·cm−5); and 4) all three variables of interest (WHO FC, 6MWD, BNP or NT-proBNP) available at baseline. Patients with other forms of PH were excluded from this analysis as were patients with Eisenmenger syndrome and patients with confirmed or suspected pulmonary veno-occlusive disease or pulmonary capillary haemangiomatosis.
Refined risk stratification
The cut-off levels for WHO FC, 6MWD and NT-proBNP for the COMPERA 2.0 risk stratification model were modified from the ESC/ERS guidelines and from our previous analysis [2, 6] as follows. The refined cut-off values for 6MWD and BNP were adopted from REVEAL [8, 9]. As no NT-proBNP cut-off value to distinguish between intermediate-low risk and intermediate-high risk was available from REVEAL Lite 2, we determined the optimal cut-off from the present database by selecting the value with the highest predictive value, i.e. the lowest p-value of the log-rank test, for mortality in the group of patients with NT-proBNP levels between 300 ng·L−1 and 1100 ng·L−1 at baseline, using 50-ng·L−1 intervals.
For functional class, we considered distinguishing between WHO FC I and II. However, as very few patients in the present dataset were classified as WHO FC I (n=7 at baseline), and as WHO FC II has repeatedly been shown to be associated with good long-term survival, we continued grouping WHO FC I and II as a single (low-risk) group.
Based on the criteria shown in table 1, each variable was graded from 1 to 4, and the mean was calculated by dividing the sum of all grades by the number of variables and rounding to the next integer. For the three-stratum model, we defined a score of 1 as low risk, 2 as intermediate risk and 3 as high risk. For the four-stratum model, we used the following definitions: 1=low risk, 2=intermediate-low risk, 3=intermediate-high risk and 4=high risk. Risk stratification was performed at baseline, i.e. before initiation of PAH medications, and at first follow-up between 3 and 12 months after treatment initiation.
Criteria for refined risk stratification in the three-stratum model and the four-stratum model based on World Health Organization functional class (WHO FC), 6-min walk distance (6MWD) and brain natriuretic peptide (BNP)/N-terminal pro-BNP (NT-proBNP)
Statistical analyses
This was a post hoc analysis of prospectively collected data. Continuous data are presented as mean±sd or as median (interquartile range (IQR)), and categorical data as number and percentage. The dataset as of 30 June 2021, was analysed. Vital status was ascertained by on-site visits or phone calls to the patients or their caregivers. Patients who underwent lung transplantation and patients who were lost to follow-up were censored at the date of the last contact. No imputations were made for missing data. Survival was evaluated using Kaplan–Meier analysis and log-rank test. Survival analyses were done for the entire group and for subgroups of patients with idiopathic, heritable, drug-associated and connective tissue disease associated (CTD)-PAH according to risk at baseline and first follow-up (with survival time starting at first follow-up for the latter analysis). The effects of changes in risk from baseline to first follow-up on consecutive survival were evaluated using the Cox regression model. The associated hazard ratios (HR) and 95% confidence intervals were calculated.
All statistical analyses were performed using R version 4.0.0.
Results
Baseline characteristics and survival of the entire cohort
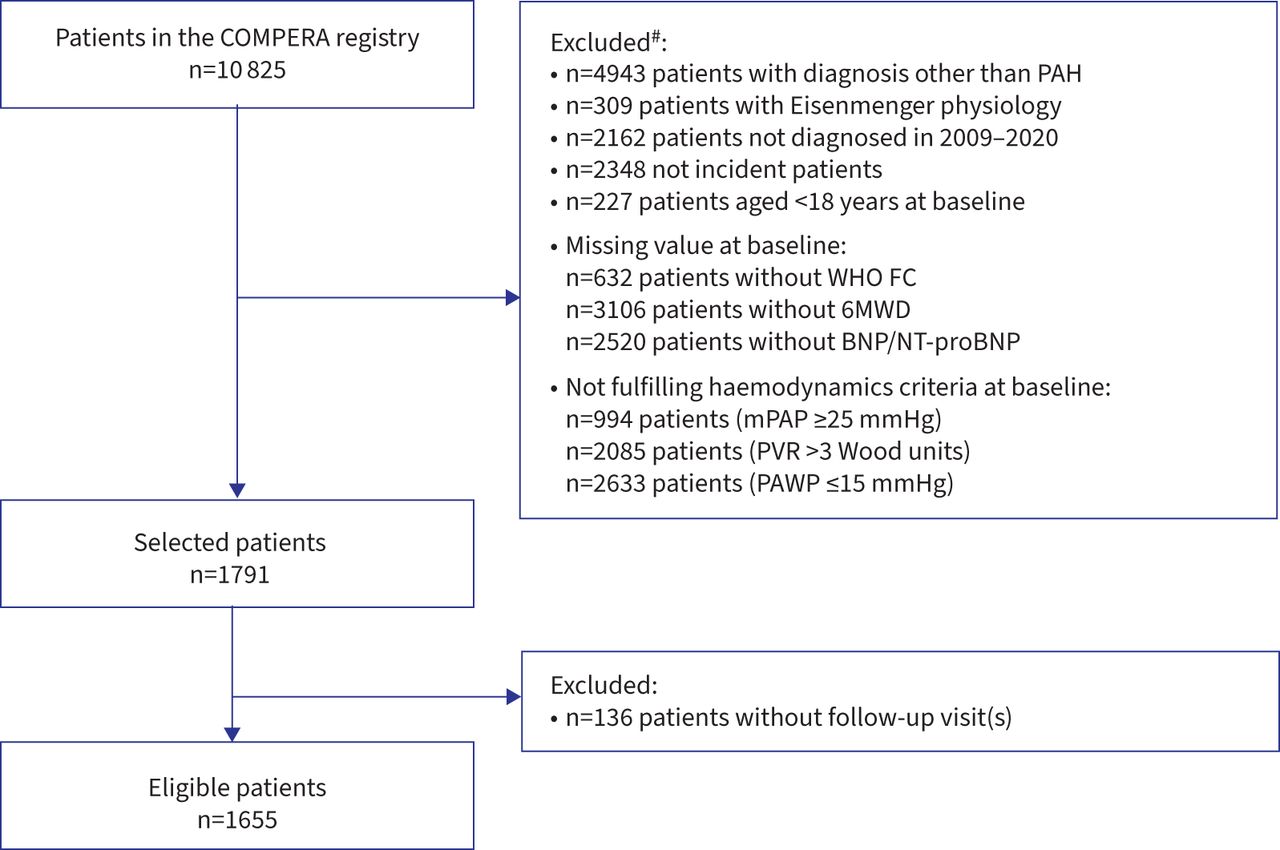
Out of 10 825 patients enrolled into COMPERA, 9710 were excluded for the reasons shown in figure 1, including 136 patients who fulfilled all inclusion criteria, but who had no follow-up information or were lost to follow-up without any information. A total of 1655 patients were finally included in this analysis. The characteristics of these patients at baseline are shown in table 2.
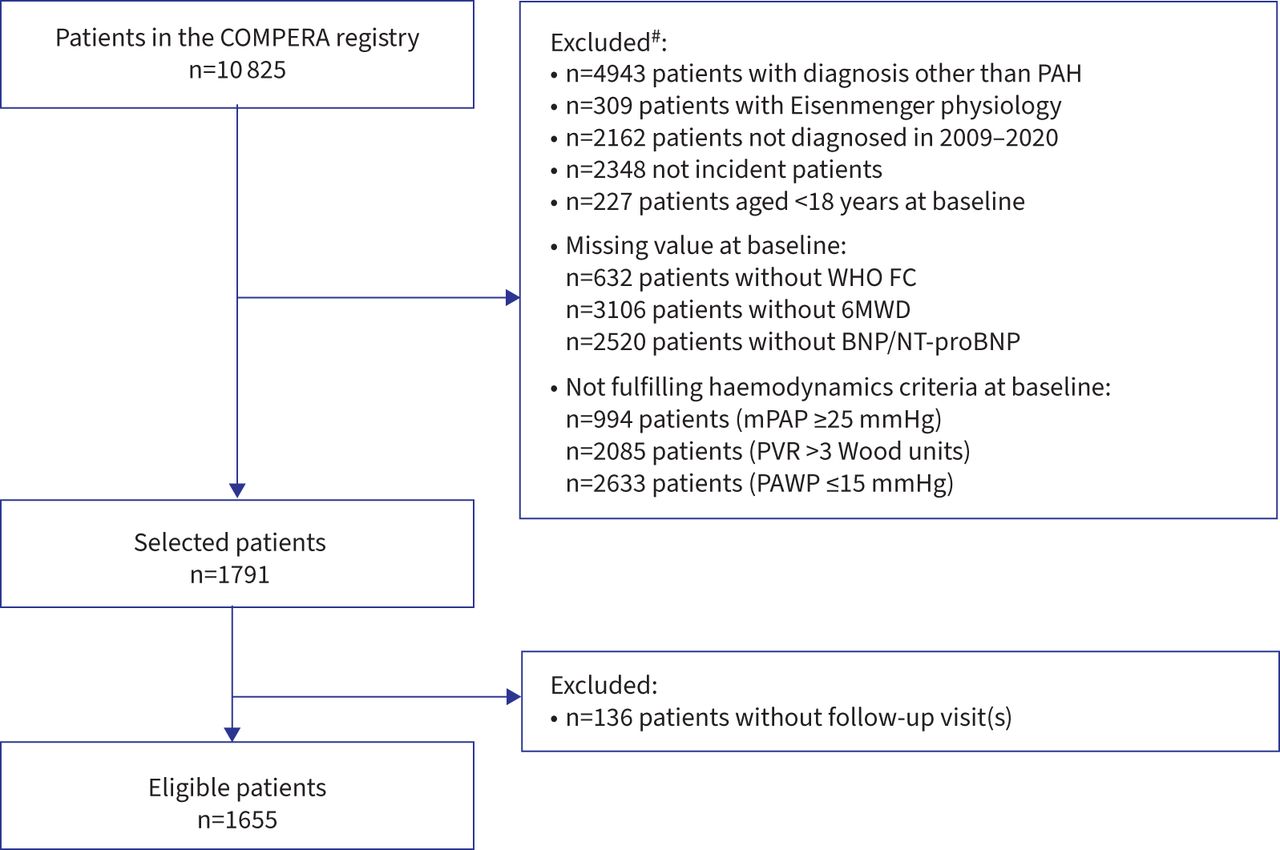
Strengthening the Reporting of Observational Studies in Epidemiology diagram showing patient eligibility for analysis. #: more than one reason for exclusion could apply. COMPERA: Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension; PAH: pulmonary arterial hypertension; WHO FC: World Health Organization functional class; 6MWD: 6-min walk distance; BNP: brain natriuretic peptide; NT-proBNP: N-terminal pro-BNP; mPAP: mean pulmonary arterial pressure; PVR: pulmonary vascular resistance; PAWP: pulmonary arterial wedge pressure.
Baseline characteristics
The median (IQR) observation time was 2.6 (1.2–4.9) years. During follow-up, 640 (38.7%) patients died, 21 (1.3%) underwent lung transplantation and 90 (5.4%) were lost to follow-up. For the entire cohort, the Kaplan–Meier estimated survival rates 1, 3 and 5 years after diagnosis were 91.1%, 70.7% and 55.2%, respectively.
Determination of NT-proBNP cut-off level to distinguish between intermediate-low and intermediate-high risk
To determine the NT-proBNP cut-off level for the discrimination between intermediate-low and intermediate-high risk, we calculated the log-rank test for patients whose baseline NT-proBNP levels were between 300 ng·L−1 and 1100 ng·L−1 (n=374), using 50-ng·L−1 steps to split these patients into two groups. As shown in supplementary figure S1, the lowest p-value (p=0.091) was found for an NT-proBNP value of 650 ng·L−1. As this number was also close to this group's median, we used it as cut-off to distinguish between the two intermediate risk groups in all further analyses.
Risk at baseline and survival
At baseline, using the three-stratum model, 142 (8.6%) patients were classified as low risk, 1257 (76.0%) patients as intermediate risk and 256 (15.5%) patients as high risk.
With the four-stratum model, 92 (5.6%) patients were classified as low risk, 401 (24.2%) patients as intermediate-low risk, 910 (55.0%) patients as intermediate-high risk and 252 (15.2%) as high risk (table 2).
The Kaplan–Meier estimated survival rates 1, 3 and 5 years after diagnosis for the low risk group were 100%, 89.0% and 82.9%, respectively; for the intermediate-low risk group, 97.9%, 85.6% and 78.6%, respectively; for the intermediate-high risk group, 90.9%, 62.2% and 50.3%, respectively; and for the high risk group, 78.1%, 46.5% and 28.2%, respectively (p<0.001 for between-group comparisons; figure 2a). The survival estimates of the idiopathic, heritable, drug-associated and CTD-PAH subgroups in the four-risk-strata model were consistent with the overall group, as shown in supplementary figures S2 and S3.

Kaplan–Meier survival curves based on the four risk strata obtained a) at baseline, b) at first follow-up.
Risk at follow-up and survival
Information on risk variables at first follow-up after treatment initiation (median 4.1 months) was available for 1414 patients (supplementary table S1). At that time, 64.1% of the patients were receiving monotherapy, 33.2% oral combination therapy and 1.3% combination therapy including intravenous or subcutaneous prostacyclin analogues (supplementary table S2).
At first follow-up, with the three-stratum model, 282 (19.9%) patients were classified as low risk, 903 (63.9%) patients as intermediate risk and 229 (16.2%) as high risk.
With the four-stratum model, 240 (17%) patients were classified as low risk, 395 patients (27.9%) as intermediate-low risk, 534 (37.8%) as intermediate-high risk and 245 (17.3%) as high risk.
The Kaplan–Meier estimated survival rates 1, 3 and 5 years after diagnosis for the low risk at first follow-up group were 98.5%, 91.2% and 82.8%, respectively; for the intermediate-low risk group, 97.2%, 81.8% and 66.8%, respectively; for the intermediate-high risk group, 91.3%, 63.0% and 46.5%, respectively; and for the high risk group, 78.0%, 48.0% and 33.3%, respectively (p<0.001 for between-group comparisons; figure 2b).
Changes in risk from baseline to first follow-up and survival
Overall, risk improved from baseline to first follow-up (figure 3). When the three-stratum approach was applied to the current dataset, 440 (31.1%) patients changed their risk category (figure 3a and supplementary table S3). Changes in risk from baseline to follow-up were associated with changes in long-term mortality risk, as shown in figure 4a and b.

Change in risk from baseline to first follow-up. Risk at baseline and at first follow-up and changes in risk are shown for a) the three-stratum model and b) the four-stratum model.
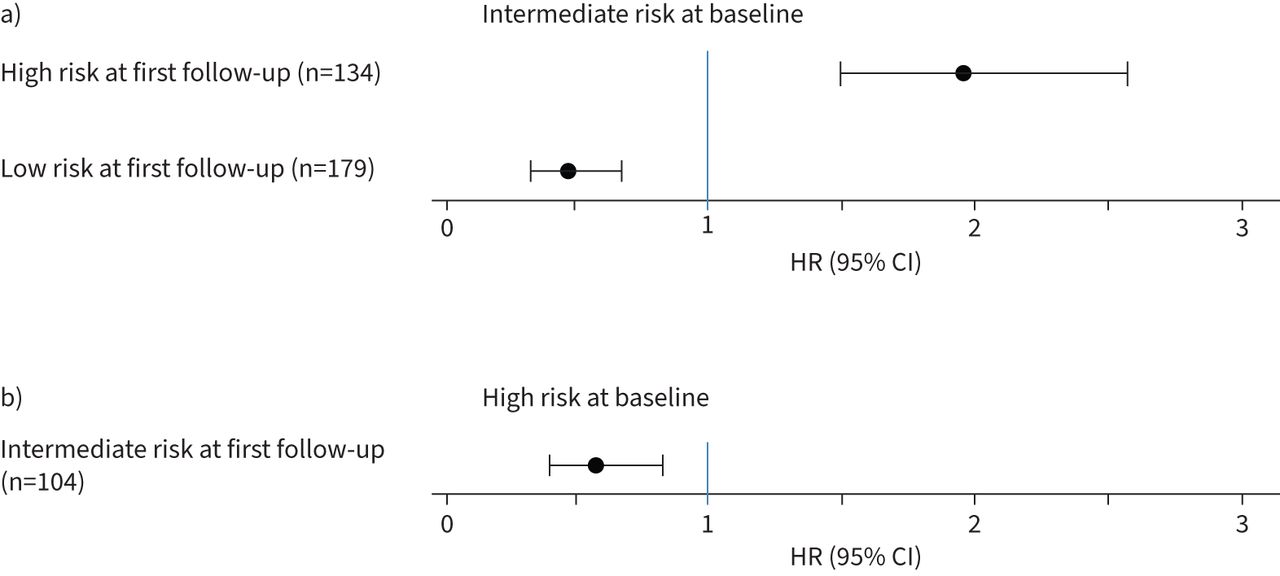
Mortality risk of patients who changed their risk category from baseline to follow-up with the three-stratum model. Mortality risk of patients who changed from baseline to follow-up with the three-stratum model a) from intermediate risk to other risk categories and b) from high risk to intermediate risk. Data for patients coming from low risk at baseline and those from patients coming from high risk and improving to low risk are not shown due to small numbers. All comparisons were made against patients who remained in their original risk category. Analyses were done with Cox proportional hazard models and depicted as hazard ratio (HR) and 95% confidence intervals.
Using the refined four-stratum approach, 695 (49.2%%) patients changed their risk category from baseline to first follow-up including 263 (18.6%) patients who changed between the intermediate-low and intermediate-high strata (figure 3b and supplementary table S4).
Changes in risk observed with the four-stratum model including those between intermediate-low and intermediate-high risk were associated with changes in long-term mortality risk (figure 5a–d). In patients who started at intermediate-low risk at baseline, the likelihood of death increased by 60.3% in those who deteriorated to intermediate-high risk at follow-up (n=65), compared to patients who remained at intermediate-low risk (HR 1.603, 95% CI 0.921–2.792); if these patients improved to low risk (n=102), the likelihood of death decreased by 35.5% (HR 0.645, 95% CI 0.343–1.214; figure 5a).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mortality risk of patients who changed their risk category from baseline to follow-up with the four-stratum model. Survival of patients who changed from baseline to follow-up with the four-stratum model a) from intermediate-low risk to other risk categories, b) from intermediate-high risk to other risk categories, c) from high risk to other risk categories and d) from intermediate-high or high risk combined to intermediate-low or low risk. Data for patients coming from low risk at baseline and those from patients coming from high risk and improving to low risk are not shown due to small numbers. All comparisons were made against patients who remained in their original risk category. Analyses were done with Cox proportional hazard models and depicted as hazard ratio (HR) and 95% confidence intervals.
In patients coming from intermediate-high risk at baseline, the likelihood of death decreased by 20.1% in those who improved to intermediate-low risk at follow-up (n=198) compared to patients who remained at intermediate-high risk (HR 0.799, 95% CI 0.611–1.046; figure 5b). If these patients deteriorated to high risk at follow-up (n=139), they had a 49.2% increased likelihood of death compared to patients who remained at intermediate-high risk (HR 1.492, 95% CI 1.122–1.983; figure 5b). Conversely, in patients coming from high risk at baseline, only a slightly decreased likelihood of death was seen when improving to intermediate-high risk at follow-up (n=80) compared to patients who remained at high risk (HR 0.895, 95% CI 0.608–1.317; figure 5c).
Of note, of 995 patients who were classified as high or intermediate-high risk at baseline, only 75 (7.5%) improved to low risk at follow-up, but 216 (21.7%) improved to intermediate-low risk (supplementary table S4). In this group of patients, reaching an intermediate-low risk profile at follow up was associated with a 41.3% reduction in the likelihood of death compared to patients who did not improve their risk category (HR 0.587, 95% CI 0.459–0.749; figure 5d).
Discussion
In the present study, we evaluated a modified risk assessment strategy termed COMPERA 2.0 using four instead of three risk strata, and refined cut-off levels for 6MWD and BNP/NT-proBNP. The main findings were 1) very few patients (5.6%) were at low risk at the time of diagnosis; 2) with the three-stratum model, most patients presented with an intermediate risk profile at the time of diagnosis and at follow-up, and this group was further divided into intermediate-low and intermediate-high risk groups with the four-stratum model; 3) the long-term survival of patients presenting with low or intermediate-low risk at the time of diagnosis was almost identical; 4) at follow-up, all four risk strata were of reasonable size (17–38% of the patients), showing significant differences in long-term survival; 5) with the four-stratum model, changes in risk from baseline to first follow-up were documented in 49.2% of the patients, compared to 31.1% with the three-stratum model; 6) changes in risk from baseline to first follow-up observed with the four-stratum model, including changes between intermediate-low and intermediate-high risk, were associated with changes in long-term mortality risk; and 7) patients classified as high or intermediate-high risk at baseline had a very low likelihood of reaching a low risk profile, but a higher likelihood of reaching an intermediate-low risk profile, which was associated with a decreased mortality risk over time.
It was not surprising to find a very low number of patients presenting with a low risk profile at the time of diagnosis. This is in line with previous data from SPAHR and COMPERA [5, 6] as well as findings from the French registry [4]. At baseline, the four-stratum model did not show a survival difference in patients classified as low or intermediate-low risk. However, risk assessment at the time of diagnosis is particularly important for identifying high-risk patients, for whom initial combination therapy including intravenous or subcutaneous prostacyclin analogues is recommended, whereas for all other patients, initial oral combination therapy is currently the preferred treatment [2, 3]. Hence the absence of a survival difference between patients presenting with low or intermediate-low risk at baseline is not considered a shortcoming of the proposed model. At the same time, an intermediate-high risk status at baseline may prompt physicians to initiate a more aggressive therapeutic approach, especially when keeping in mind a recent publication from France on the effects of initial treatment strategies on long-term survival [18].
Compared to risk assessment at the time of diagnosis, risk stratification after treatment initiation provides more reliable prognostic information as it incorporates the individual response to therapy [19]. It has already been shown by several groups that changes in risk translate into changes in long-term survival [4, 6, 9]. However, a substantial limitation of the three-stratum model is that most patients present at intermediate risk at baseline and during follow-up while the number of patients who change their risk category is relatively low. Applying the original three-stratum model to the present series, 76.0% of the patients were at intermediate risk at baseline and 63.9% at follow-up, and only 31.1% changed their risk category between baseline and first follow-up. Thus, the three-stratum model may not be sufficiently sensitive to prognostically relevant changes. With the refined four-stratum model, changes from baseline to first follow-up were observed in 49.2% of the patients. Changes between the intermediate-low and intermediate-high strata occurred in 18.6% of the patients, and these changes had an impact on consecutive survival. Hence, there was more between-group penetrability with the four-stratum model, which may be of relevance not only in clinical settings but also when risk stratification tools are considered as end-points in clinical trials, where it will have a substantial impact on sample size calculations if changes can be expected to occur in ~30% or in almost 50% of the participants.
According to current guidelines, achieving and maintaining a low risk profile is a major treatment objective in PAH [1–3], but it has been shown that this goal is not reached in most patients [4, 6, 20]. In the present series, only 7.5% of the patients who were classified as high or intermediate-high risk at baseline reached the low risk category at follow-up, while 21.7% reached the intermediate-low risk category, which was associated with a decreased mortality risk, albeit less so than with reaching the low risk category. Thus, while improving from high or intermediate-high to intermediate low risk can be considered a partial treatment success, our data confirm that a low risk profile is an essential treatment goal in patients with PAH. At the same time, an intermediate-high risk category at follow-up was associated with a high mortality risk and should trigger treatment escalation whenever reasonably possible. Hence, the distinction between intermediate-low and intermediate-high risk can support clinical decision-making.
In the present analysis, we used several cut-off values that have originally been proposed by the REVEAL group [7–9], and one may ask why not use REVEAL Lite 2 instead of COMPERA 2.0? REVEAL Lite 2 is a well validated and established tool, but we believe that our model has potential advantages. Firstly, REVEAL Lite 2 has no NT-proBNP cut-off to distinguish between intermediate-low and intermediate-high risk, which is a major drawback, as NT-proBNP is used more frequently than BNP as cardiac biomarker. Secondly, REVEAL Lite 2 includes heart rate and systolic blood pressure, i.e. two highly variable parameters, which were not obtained in a standardised manner in the original REVEAL registry [8]. The prognostic value of these parameters awaits independent confirmation, especially when added to functional class, 6MWD and BNP/NT-proBNP. Thirdly, REVEAL Lite 2 incorporates renal dysfunction, defined as estimated glomerular filtration rate <60 mL·min−1·1.73 m−2 or renal insufficiency deemed present by the investigator. While there is little doubt that kidney function is prognostically important in patients with PAH [21], we believe that this variable needs to be better defined and validated before being included in risk stratification models. The COMPERA 2.0 model is based only on parameters that have been thoroughly validated, and future studies are needed to determine whether the use of additional parameters increases the predictive value of this tool.
The limitations of the present study are those inherent to registry analyses, including lack of standardised visit schedules and missing values. The number of patients lost to follow-up was small, but not negligible. Although the sample size was relatively large, the numbers became small for the subgroup analyses. This was particularly relevant for the number of patients who changed their risk category between baseline and follow-up, which became relatively small in some subsets, so that statistical significance could not be claimed for all possible changes in risk and their impact on consecutive survival. Furthermore, the NT-proBNP cut-off value was derived and validated in the same cohort, so that independent confirmation is necessary. In addition, we did not attempt to further calibrate and weigh the variables in our model.
As a general limitation, all available simplified models provide a basic risk assessment, while individual risk is determined by numerous other factors including age [22, 23], sex [24], type of PAH [25], symptoms, signs, disease trajectories [26] and comorbidities [16]. In addition, risk stratification can be modified by variables derived from cardiac imaging [27–30], cardiopulmonary exercise testing [31] and right heart catheterisation [13, 32]. Hence, while combining functional class, 6MWD and NT-proBNP has proven useful for a primary risk assessment, all available information should be considered for individual treatment decisions.
In summary, our data show that a four-stratum risk model based on refined cut-off levels for WHO FC, 6MWD and BNP/NT-proBNP was more sensitive than the three-stratum model to prognostically relevant changes in risk. Thus, it is possible that the four-stratum model may be more useful both in clinical practice and as a research tool in clinical trials. If these findings can be confirmed by other groups, the four-stratum model may replace the current three-stratum model as risk stratification tool in PAH.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-02311-2021.Supplement
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-02311-2021.Shareable
Footnotes
This article has supplementary material available from erj.ersjournals.com
Conflict of interest: M.M. Hoeper has received fees for lectures and/or consultations from Acceleron, Actelion, Bayer, GSK, Janssen, MSD and Pfizer.
Conflict of interest: C. Pausch has nothing to disclose.
Conflict of interest: K.M. Olsson has received fees for lectures and/or consultations from Acceleron, Actelion, Bayer, GSK, Janssen, MSD, Pfizer and United Therapeutics.
Conflict of interest: D. Huscher has received travel compensation from Shire.
Conflict of interest: D. Pittrow has received fees for consultations from Actelion, Amgen, Aspen, Bayer, Biogen, Boehringer Ingelheim, Daiichi Sankyo, MSD, Novartis, Sanofi-Genzyme, Takeda and Viatris.
Conflict of interest: E. Grünig has received fees for lectures and/or consultations from Actelion, Bayer, GSK, Janssen, MSD, Pfizer and United Therapeutics.
Conflict of interest: G. Staehler has received honoraria for lectures and/or consultancy for Actelion, Bayer, GSK, Novartis and Pfizer.
Conflict of interest: C.D. Vizza has received fees for lectures and/or consultations from Acceleron, Actelion, Bayer, GSK, Janssen, MSD, Pfizer and United Therapeutics.
Conflict of interest: H. Gall reports personal fees from Actelion, AstraZeneca, Bayer, BMS, GSK, Janssen-Cilag, Lilly, MSD, Novartis, OMT, Pfizer and United Therapeutics.
Conflict of interest: O. Distler has/had consultancy relationship and/or has received research funding from 4 D Science, Actelion, Active Biotec, Bayer, Biogen Idec, Boehringer Ingelheim Pharma, BMS, ChemoAb, EpiPharm, Ergonex, espeRare foundation, GSK, Genentech/Roche, Inventiva, Janssen, Lilly, medac, MedImmune, Mitsubishi Tanabe, Pharmacyclics, Pfizer, Sanofi, Serodapharm and Sinoxa in the area of potential treatments of scleroderma and its complications including PAH; and has a patent mir-29 for the treatment of systemic sclerosis licensed.
Conflict of interest: C. Opitz has nothing to disclose.
Conflict of interest: J.S.R. Gibbs has received fees for lectures and/or consultations from Acceleron, Actelion, Aerovate, Bayer, Complexia, Janssen, MSD, Pfizer and United Therapeutics.
Conflict of interest: M. Delcroix reports research grants from Actelion/J&J, speaker and consultant fees from Bayer, MSD, Acceleron, AOP and Daiichi Sankyo, outside the submitted work; and is holder of the Janssen Chair for Pulmonary Hypertension at the KU Leuven.
Conflict of interest: H.A. Ghofrani has received honoraria for consultations and/or speaking at conferences from Bayer HealthCare AG, Actelion, Encysive, Pfizer, Ergonex, Lilly and Novartis; is member of advisory boards for Acceleron, Bayer HealthCare AG, Pfizer, GSK, Actelion, Lilly, Merck, Encysive and Ergonex; has received governmental grants from the German Research Foundation (DFG), Excellence Cluster Cardiopulmonary Research (ECCPS), State Government of Hessen (LOEWE) and the German Ministry for Education and Research (BMBF).
Conflict of interest: D-H. Park has nothing to disclose.
Conflict of interest: R. Ewert has received speaker fees and honoraria for consultations from Actelion, Bayer, GSK, Janssen, Lilly, MSD, Novartis, Pfizer and United Therapeutics.
Conflict of interest: H. Kaemmerer has received honoraria for lectures and/or consultancy from Actelion, Bristol Myers Squibb and Janssen.
Conflict of interest: H-J. Kabitz has received fees from Löwenstein Medical, Weinmann, Philips Respironics, ResMed, Vivisol, Sapio Life and Sanofi-Genzyme.
Conflict of interest: D. Skowasch received fees for lectures and/or consulting and/or research support (paid to institution) from Actelion, Bayer, GSK, Janssen, MSD and Pfizer.
Conflict of interest: J. Behr received grants from Actelion, Bayer, Biogen, Boehringer Ingelheim, Galapagos, Novartis, Roche and Sanofi/Genzyme.
Conflict of interest: K. Milger has received fees from Actelion, AstraZeneca, GSK, Janssen, MSD, Novartis and Sanofi-Aventis.
Conflict of interest: M. Halank has received speaker fees and honoraria for consultations from Acceleron, Actelion, AstraZeneca, Bayer, BerlinChemie, GSK, Janssen and Novartis.
Conflict of interest: H. Wilkens received fees for lectures and/or consultations from Actelion, Bayer, Biotest, Boehringer, GSK, Janssen, Pfizer and Roche.
Conflict of interest: H-J. Seyfarth has received speaker fees and honoraria for consultations from Actelion, Bayer, GSK, Janssen and MSD.
Conflict of interest: M. Held has received speaker fees and honoraria for consultations from Actelion, Bayer, Boehringer Ingelheim Pharma, GlaxoSmithKline, Janssen, MSD, Novartis, Pfizer, Nycomed, Roche and Servier.
Conflict of interest: D. Dumitrescu declares honoraria for lectures and/or consultancy from Actelion, AstraZeneca, Bayer, GSK, Janssen, MSD, Novartis, Pfizer, Servier and Vifor.
Conflict of interest: I. Tsangaris has received fees from Actelion, Bayer, ELPEN, GSK, Janssen, MSD, Pfizer and United Therapeutics.
Conflict of interest: A. Vonk-Noordegraaf reports receiving fees for lectures and/or consultations from Actelion, Bayer, GlaxoSmithKline, Janssen, MSD and Pfizer.
Conflict of interest: S. Ulrich reports personal fees from Actelion, Janssen and MSD outside the submitted work.
Conflict of interest: H. Klose has received speaker fees and honoraria for consultations from Actelion, Bayer, GSK, Janssen, MSD, Novartis, Pfizer and United Therapeutics.
Conflict of interest: M. Claussen reports honoraria for lectures from Boehringer Ingelheim Pharma GmbH and Roche Pharma, and for serving on advisory boards from Boehringer Ingelheim.
Conflict of interest: T.J. Lange has received speaker fees and honoraria for consultation from Acceleron, Actelion, Bayer, GSK, Janssen-Cilag, MSD, Pfizer and United Therapeutics.
Conflict of interest: S. Rosenkranz has received fees for lectures and/or consultations from Abbott, Acceleron, Actelion, Bayer, BMS, Gilead, GSK, Janssen, MSD, Novartis, Pfizer, United Therapeutics and Vifor; research grants to institution from AstraZeneca, Actelion, Bayer Janssen and Novartis.
- Received August 23, 2021.
- Accepted October 29, 2021.
- Copyright ©The authors 2022.
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










