





Abstract
Background The major reasons to treat sarcoidosis are to lower the morbidity and mortality risk or to improve quality of life (QoL). The indication for treatment varies depending on which manifestation is the cause of symptoms: lungs, heart, brain, skin or other manifestations. While glucocorticoids remain the first choice for initial treatment of symptomatic disease, prolonged use is associated with significant toxicity. Glucocorticoid-sparing alternatives are available. The presented treatment guidelines aim to provide guidance to physicians treating the very heterogenous sarcoidosis manifestations.
Methods A European Respiratory Society Task Force committee composed of clinicians, methodologists and patients with experience in sarcoidosis developed recommendations based on the GRADE (Grading of Recommendations, Assessment, Development and Evaluations) methodology. The committee developed eight PICO (Patients, Intervention, Comparison, Outcomes) questions and these were used to make specific evidence-based recommendations.
Results The Task Force committee delivered 12 recommendations for seven PICOs. These included treatment of pulmonary, cutaneous, cardiac and neurologic disease as well as fatigue. One PICO question regarding small-fibre neuropathy had insufficient evidence to support a recommendation. In addition to the recommendations, the committee provided information on how they use alternative treatments, when there was insufficient evidence to support a recommendation.
Conclusions There are many treatments available to treat sarcoidosis. Given the diverse nature of the disease, treatment decisions require an assessment of organ involvement, risk for significant morbidity, and impact on QoL of the disease and treatment.
Abstract
Evidence-based guidelines for the treatment of sarcoidosis are presented. The ERS Task Force committee used the GRADE approach and specific recommendations are made. A major factor in treating patients is the risk of loss of organ function or impairment of quality of life. https://bit.ly/3iAERfY
Introduction
The previous international statement for the diagnosis and management of sarcoidosis was developed in 1999 by the European Respiratory Society (ERS), American Thoracic Society (ATS), and World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) [1, 2]. The diagnostic approach has recently been updated [3]. Over time, there has been a shift of emphasis on who, when and with what to treat sarcoidosis patients [4, 5]. The decision of who and when to treat an individual sarcoidosis patient depends on two major factors: risk for death or organ failure and impairment of quality of life (QoL). About 5% of patients with sarcoidosis die from the disease [4, 6–8]. Pulmonary and cardiac disease are the most common reasons for death from sarcoidosis [9]. Irreversible organ damage to the brain, eyes or kidneys can also cause significant morbidity [10]. Recent studies have identified features associated with increased risk for death from pulmonary disease, including pulmonary hypertension, reduced lung function and pulmonary fibrosis [6, 11–13]. Anti-inflammatory therapy for less severe but impaired patients may prevent progression to irreversible disease [10]. Both sarcoidosis-associated fatigue (SAF), a symptom not associated with a specific organ manifestation, and small-fibre neuropathy (SFN)-associated symptoms are encountered in a significant number of sarcoidosis patients [14–17], and treatment is a high priority for these patients [18]. While fatigue is common, we looked specifically at fatigue severe enough to consider treatment (troublesome fatigue).
A Task Force committee was developed by the ERS to develop new guidelines for treating sarcoidosis using a standardised methodology [19]. The committee systematically reviewed treatment for pulmonary, cutaneous, cardiac and neurologic manifestations as well as SAF and SFN. There have been several proposed terms to describe the clinical phenotype of sarcoidosis patients, including stage (which refers to the chest radiography pattern as described by Scadding [20]), activity (ongoing inflammation) and acute versus chronic [5]. Most of the papers reviewed did not offer specific criteria of the patients treated. We chose to make our recommendations based on the presence of symptomatic disease unless otherwise noted. Specific recommendations for each PICO (Patients, Intervention, Comparison, Outcomes) question using GRADE (Grading of Recommendations, Assessment, Development and Evaluations) criteria are shown in table 1. The committee found insufficient information to make recommendations for other organ involvement. While eye involvement occurs in a significant number of cases, there are few studies specifically regarding treatment of ocular sarcoidosis [21–24] and the committee did not feel this could be studied at this time. There have been some studies reporting on the use of adalimumab for non-infectious uveitis including sarcoidosis [25, 26]. However, these studies did not specifically analyse ocular sarcoidosis. To date, few studies have reported specifically on the effectiveness of adalimumab for ocular sarcoidosis [21, 23, 27].
Task Force recommendations
Table 2 summarises the anti-inflammatory drugs used in the treatment of sarcoidosis [4, 28–48]. More details regarding dosages, major toxicities and monitoring are given in supplement S1 in the supplementary material. General comments regarding individual therapies for sarcoidosis are reviewed in supplement S1 in the supplementary material. We did not search studies that specifically evaluated dosing, monitoring or compared one versus another treatment duration for any form of sarcoidosis. Several studies have noted that relapse of symptomatic disease occurs in a significant number of patients upon withdrawal of therapy after 1–2 years. The reported rate of relapse of disease upon glucocorticoid withdrawal after 2 years of initial therapy ranges from 20% to 80% [28–31]. Withdrawal of methotrexate therapy after 2 additional years for chronic sarcoidosis was associated with an 80% re-institution of systemic therapy [32]. For patients treated with infliximab for advanced sarcoidosis, discontinuation of treatment after 6–12 months was associated with relapse of disease more than half the time [33–35]. These observations have led to the comment that patients may have modifications of treatment to avoid toxicity and the need for continued successful treatment should be re-evaluated every 1–2 years [4].
Immunosuppressive therapies for sarcoidosis
For the most part, the analysis was restricted to anti-inflammatory treatments. Use of agents to treat complications of sarcoidosis such as pulmonary hypertension and hydrocephalus were not evaluated. Nor did we analyse the results of transplantation, especially lung or heart transplantation, which can be an important part of the management of advanced disease [36–38].
Methodology
This guideline was developed by an ERS Task Force chaired by R. Baughman (USA) and D. Valeyre (France). The Task Force included specialists with recognised expertise in the management of patients with sarcoidosis (13 pulmonologists and one haematologist/oncologist), three ERS methodologists (T. Tonia, B. Nagavci and D. Rigau) and three clinician-methodologists (two general pulmonologists (D. Ouellette and A. Mathioudakis) and one rheumatologist (P. Korsten) who also specialised in sarcoidosis), and three patient representatives from Germany, Italy and the USA.
The guideline panel held four meetings beginning in early 2017. A total of eight clinical questions were formulated using the PICO format. Panel members rated selected outcomes as being not important, important or critical for decision making (table 3). These outcomes were used as markers for indications for treatment for individual PICOs. Systematic literature reviews were conducted for each question. Teams consisting of two sarcoidosis experts, one methodologist and one patient representative were assigned to each clinical question. Teams met virtually and during physical meetings to address the topics. The patient representatives were full members of the guideline committee and represented three different countries’ support groups: Germany, Italy and the USA. In addition, we had performed (and published) a large multilanguage questionnaire in which over 1800 sarcoidosis patients rated the level of importance of key outcomes [18].
Outcomes for patient care and clinical research
Literature searches and systematic literature review
A team of three librarians at an independent centre (Henry Ford Hospital, Detroit, MI, USA) contributed to the development of the systematic review. Searches were conducted in MEDLINE, Embase and the Cochrane Database of Systematic Reviews between February 2017 and July 2017. An update of the search was performed in November 2018. Furthermore, supplementary searches were conducted (in PubMed) using relevant studies and systematic reviews to find additional potentially relevant studies not covered by the main searches (latest search: January 2021).
Librarians collaborated with a clinician-methodologist liaison (D. Ouellette) to design and run a search strategy using MeSH (Medical Subject Headings) terms and key words for each clinical question. The search was limited to studies in the English language. The search retrieved 6968 records. The search was reviewed by sarcoidosis experts for completeness. Teams excluded studies based on pre-defined selection criteria. Some studies required obtaining the full text for review. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [58] details for each PICO are shown in supplement S2 in the supplementary material. We selected randomised controlled trials, and in their absence comparative observational studies, addressing each of the PICO questions. We extracted details on the design, eligibility criteria and interventions of all included studies, on the baseline characteristics of the study participants, and on the outcomes of interest. Risk of bias of randomised controlled trials and observational studies was evaluated using the Cochrane risk of bias tool [59] and Newcastle–Ottawa scale [60], respectively. When it was meaningful, meta-analysis was conducted following methodology suggested by Cochrane [61] and the GRADE collaboration [62]. Heterogeneity was assessed using I2 and meta-analyses were conducted using a random effects model in anticipation of clinical and methodological heterogeneity [61]. Publication bias was not evaluated as none of the meta-analyses included an adequate number of studies [61]. Certainty in the body of evidence was assessed using GRADE methodology [62]. The PRISMA flow diagrams specify the primary articles for each PICO, and the evidence summaries, evidence to decision tables and summary of judgements are shown for each recommendation (supplement S2 in the supplementary material). In cases of uncertainty, decisions were reached by discussion with the ERS methodologists and consensus. Included references are listed in the evidence summaries.
Assessment of the level of evidence and degree of recommendations
We followed the GRADE approach to assess the confidence in the evidence (quality) and the degree of recommendations [63]. Recommendations were graded as strong or conditional after considering the quality of the evidence, the balance of desirable and undesirable consequences of compared management options, the assumptions about the relative importance of outcomes, the implications for resource use, and the acceptability and feasibility of implementation [63]. Evidence summary of findings tables and evidence to decisions frameworks were generated for each clinical question (supplement S2 in the supplementary material) [64]. The panel formulated the clinical recommendations and decided on their strength first by consensus and then by voting for final recommendations. Following the GRADE approach, strong recommendations were worded as “we recommend”, while conditional recommendations were worded as “we suggest”.
A strong recommendation was made for an intervention when the panel was certain that the desirable consequences of the intervention outweighed the undesirable consequences and a strong recommendation against an intervention was made when the opposite was true. A strong recommendation indicates that most patients and healthcare providers would choose to have, or not to have, the intervention.
A conditional recommendation for an intervention was made when the panel was uncertain that the desirable consequences of an intervention outweighed the undesirable consequences in most patients and a conditional recommendation against an intervention was made when uncertainty existed that undesirable consequences of an intervention outweighed the desirable consequences in most patients. Reasons for uncertainty included low quality of evidence, a close balance between desirable and undesirable effects or patients’ values and preferences. A conditional recommendation indicates that different patients and healthcare providers may make different choices regarding an intervention.
In addition to the recommendations, specific considerations were made regarding individual PICOs. These considerations reflect the Task Force members current practice and describe their clinical experience. They are used in these guidelines to compliment the algorithms, but they are not intended as recommendations for clinical practice. Data supporting these comments was provided for each of the PICOs. For each PICO group, an algorithm was generated and a colour code used to differentiate strong (blue) and conditional (orange and purple) recommendations and no colour for current practice. In addition, we have added comments regarding continuation of therapy (green) or consider changing therapy (yellow). All recommendations, comments and algorithms were reviewed and approved by the full panel.
Disclosure of potential conflicts of interest
Committee members disclosed all potential conflicts of interest according to ERS policy. Conflicted members were asked to abstain from discussions and voting on recommendations in which they were considered to have potential conflicts. Compliance with the conflict of interest policy was monitored by the chairs. All members, including the methodologists and the patient representatives, were active voting members of the panel.
Pulmonary sarcoidosis
General considerations
Treatment indications in patients with pulmonary sarcoidosis are the balance of a) the minimisation of risk of disability, loss of life due to pulmonary involvement or loss of QoL, and b) the risk of comorbidities and loss of QoL due to glucocorticoid and other therapies [65]. Interstitial lung disease (ILD) or pulmonary hypertension are the main causes of sarcoidosis-related mortality [6, 13, 66] and represent risks of lifelong exercise intolerance. In Japan, where cardiac involvement is more common than the rest of the world, cardiac sarcoidosis remains a major cause of death [67]. Many patients suffer from unacceptable loss of QoL due to dyspnoea, chest pain, cough, and, variably, malaise, fatigue and arthralgia [4]. We draw a major distinction between treatment decisions based on medical expertise for patients with higher risk disease and those centred on the wishes of the informed patient, implying the choice, dose, duration and dose alterations of treatment, which are primarily driven by loss of QoL. As noted previously, high-risk pulmonary sarcoidosis patients include those with reduced forced vital capacity (FVC) and diffusing capacity of the lung for carbon monoxide (DLCO), moderate to severe pulmonary fibrosis or pre-capillary pulmonary hypertension [6, 12, 13]. In existing placebo-controlled trials, no distinction is made to separate the treatment goals of minimising danger and maximising QoL.
At presentation, patients usually undergo pulmonary function tests with measurements of FVC, forced expiratory volume in 1 s (FEV1) and DLCO, chest radiography, and, in those with clinically significant pulmonary sarcoidosis, high-resolution chest computed tomography (HRCT) [4]. In some cases, the 6-min walk distance (6MWD) may be reduced because of pulmonary or cardiac disease, muscle involvement, or fatigue [50]. Transthoracic echocardiography may be indicated in patients with chronic exercise intolerance or suspected pulmonary hypertension [68]. General treatment goals are to achieve either disease regression or short-term disease stabilisation (when irreversible) with higher dose glucocorticoid treatment and to identify the minimum longer term glucocorticoid dose required for stabilisation of sarcoidosis.
Institution of treatment usually relies on both structural and pulmonary function changes. Both chest radiography and HRCT provide static images of structural changes, whereas the hybrid positron emission tomography (PET) provides both a structural and functional lung assessment. Lung involvement per se is not an indication for treatment, but extensive ILD or pulmonary fibrosis confers an increased long-term risk of respiratory failure [6, 13, 66]. Evolving evidence suggests that PET can aid intervention response assessment [69, 70]. High standardised uptake value levels are associated with more rapid and better regression of disease after treatments [48, 71–73]. Since PET and HRCT are expensive and associated with radiation exposure, they should be considered on a case-by-case basis. FVC, DLCO, Borg score for dyspnoea and 6MWD may aid in assessing functional changes [74].
PICO 1: In patients with pulmonary sarcoidosis, should glucocorticoid treatment be used versus no immunosuppressive treatment?
Recommendation
For untreated patients with major involvement from pulmonary sarcoidosis believed to be at higher risk of future mortality or permanent disability from sarcoidosis, we recommend the introduction of glucocorticoid treatment to improve and/or preserve FVC and QoL. (Strong recommendation, low quality of evidence.)
Summary of evidence
The clinical outcomes identified by the panel included overall response, chest radiography and pulmonary function changes, and symptoms. Unfortunately, markers for increased morbidity or mortality were not specifically studied in the identified trials. Our systematic review identified 1747 potentially relevant articles; the full texts of 36 were reviewed and 19 were selected [28, 31, 75–91]. Many of our pre-specified outcomes were not evaluated in these trials.
The overall response to oral glucocorticoid treatment, based on clinical and radiological evaluation of two studies involving 134 patients [75, 76], found a larger proportion of patients experiencing clinical improvement (risk ratio 2.44, 95% CI 1.40–4.25) in short-term follow-up (3–6 months). There was also a trend towards fewer patients experiencing clinical deterioration (risk ratio 0.38, 95% CI 0.11–1.31), in the short term. In three placebo-controlled trials involving 340 patients [75, 77, 78], radiographic improvements favoured glucocorticoid treatment (risk ratio 1.35, 95% CI 1.11–1.64) with a lower prevalence of significant radiographic deterioration (risk ratio 0.39, 95% CI 0.18–0.87). Pulmonary function was not significantly impacted for the whole group [75, 77, 78], but there was a significant pulmonary function improvement for patients with initial lung involvement [77, 79]. Asymptomatic patients without radiographic improvement were randomly allocated to receive either glucocorticoids for at least 18 months or glucocorticoids only if clinically worsened. At 5 years the treated group had better functional outcome [80]. It should be stressed that these data may not apply to the subgroup of patients with higher risk disease. Interventions across the entire range of disease severity, including patients with limited or inactive disease, do not provide guidance in this important subgroup. This especially holds true for failure to demonstrate pulmonary function improvement in whole cohorts, including many patients with mild or intrinsically irreversible disease. Specifically, there is no existing controlled evaluation of glucocorticoid treatment efficacy in preventing pulmonary function decline in severe pulmonary disease.
Data from additional studies
Glucocorticoid treatment clearly has short-term efficacy by improving symptoms and chest radiography, and in achieving regression or prevention of progression in some cases. Currently, there is no suggestion that these effects are attenuated in higher risk disease. Based on two studies, these benefits appear to be short lived as they do not persist after discontinuation of glucocorticoids [76, 90]. The dose of glucocorticoids varied, but two studies found no additional benefit for treating pulmonary disease with more than 20 mg prednisone a day [81, 82]. It has been observed that at least half of patients started on glucocorticoids were still on treatment 2 years later [28, 31, 88]. None of the current studies or accumulated clinical experience specifically evaluated higher risk disease or whether stable disease with glucocorticoid treatment is likely to progress with the same glucocorticoid dosage. In summary, the data provide a basis for a likely long-term glucocorticoid treatment benefit in high-risk pulmonary sarcoidosis. To date, no data exist concerning mortality balance between benefits from long-term treatment and risks due to treatment-induced comorbidities. This underlines the importance of re-evaluating the need for glucocorticoid continuation in the longer term in chronic fibrotic pulmonary sarcoidosis unlikely to benefit from prolonged treatment.
Response to treatment for 3–6 months, if unsustained after treatment cessation [76, 83], provides a solid rationale to limit glucocorticoid use to patients with higher risk disease or unacceptable loss of QoL, or combined pulmonary and systemic symptoms.
In three double-blind, placebo-controlled randomised trials, the addition of inhaled glucocorticoid (versus placebo) to oral glucocorticoid did not provide significant benefits regarding symptoms or pulmonary function tests [84–86].
Justification of recommendations
Systemic glucocorticoid administration is associated with an overall response, as judged by a clinician, or based on clinical and radiological evaluation. It is also associated with radiological improvement. The strong recommendation for glucocorticoid use in symptomatic pulmonary patients at risk for mortality is based on data summarised in supplement S2 in the supplementary material and includes several randomised trials [75, 76, 78–80, 90–92]. This strong recommendation was based on the committee's consensus concerning a serious situation warranting treatment.
For patients with worsening QoL from pulmonary disease, we recommend shared decision making between physicians and patients with a consideration of initial low- to medium-dose glucocorticoid treatment (5–10 mg a day) [4], and with the dose and duration of maintenance treatment based on the efficacy/side-effects balance.
For patients not felt to be at risk for morbidity or mortality, or having no significant impairment of QoL, the Task Force usually offers no glucocorticoid treatment because of the high prevalence of adverse events. Figure 1 summarises this approach.

Approach for pulmonary sarcoidosis. Use of rituximab, JAK inhibitor and repository corticotropin injection (RCI) should be on a case-by-case basis. This figure is a combination of the recommendations made in this guideline and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. #: assess need for treatment based on low risk, intermediate risk but impaired quality of life or high risk as discussed in text. GC: glucocorticoid.
Future research
There is an urgent need for accurate risk stratification in pulmonary sarcoidosis. Unmet needs include optimal pulmonary function thresholds, integrated with disease duration and risk assessment for progression in higher risk disease. It is uncertain when higher risk disease is best managed with glucocorticoid monotherapy as opposed to combination therapy with second- or third-line agents. The role of PET in rationalising long-term treatment following initial stabilisation of irreversible disease requires exploration in large cohorts.
A database is needed to quantify the therapeutic efficacy of glucocorticoids in patients with unacceptable loss of QoL, to explore the efficacy and adverse effects with the use of low-dose glucocorticoid treatment, and to evaluate the optimal dose and duration driven by patient choice.
Another area which needs to be better studied includes how high the initial glucocorticoid dosage should be, how long to stay on that dose and how to taper.
PICO 2: In patients with pulmonary sarcoidosis, should one add immunosuppressive treatment or remain on glucocorticoid treatment alone?
Recommendations
Recommendation 1: For patients with symptomatic pulmonary sarcoidosis believed to be at higher risk of future mortality or permanent disability from sarcoidosis who have been treated with glucocorticoids and have continued disease or unacceptable side-effects from glucocorticoids, we suggest the addition of methotrexate to improve and/or preserve FVC and QoL. (Conditional recommendation, very low quality of evidence.)
Recommendation 2: For patients with symptomatic pulmonary sarcoidosis believed to be at higher risk of future mortality or permanent disability from sarcoidosis who have been treated with glucocorticoids or other immunosuppressive agents and have continued disease, we suggest the addition of infliximab to improve and/or preserve FVC and QoL. (Conditional recommendation, low quality of evidence.)
Summary of evidence
Studied populations include patients with chronic symptomatic pulmonary sarcoidosis treated with glucocorticoids and/or other immunosuppressive agents. The systematic literature review identified 1319 potentially relevant articles; the full texts of 41 were reviewed and six were selected [93–98]. We identified six drugs with adequate reports: infliximab, golimumab, ustekinumab, pentoxifylline, cyclosporine A and methotrexate. As displayed in the evidence to decision table (supplement S2 in the supplementary material), most of our pre-selected outcomes were not evaluated in clinical studies or trials. Some randomised controlled interventions were studied in patients receiving glucocorticoid. Infliximab, compared to prednisone, significantly improved FVC, the primary end-point in two phase III randomised trials for the treatment of chronic respiratory symptoms. However, absolute FVC changes were small. Secondary end-points included chest imaging and QoL assessments [94, 96].
In one randomised, double-blind, placebo-controlled trial, methotrexate did not demonstrate significant FVC improvement, although allowing a significant prednisone reduction with lower weight gain in the second 6 months [93]. Other open-label prospective and retrospective trials have found methotrexate to be steroid sparing and associated with improved lung function [45, 99, 100].
No recommendation could be made for cyclosporine A, golimumab or ustekinumab as randomised trials showed no benefit over placebo [95, 98]. These drugs should be considered on a case-by-case basis.
Data from additional studies
Azathioprine is as effective as methotrexate in pulmonary sarcoidosis [45, 101]. Leflunomide and mycophenolate mofetil are also effective [44, 46, 102]. In a randomised trial, chloroquine was mildly beneficial in pulmonary sarcoidosis [103]. In a retrospective study from one centre, chloroquine was less effective than in skin sarcoidosis [104]. Adalimumab was found effective for pulmonary disease in a prospective, open-label trial [47] and a small retrospective series [105].
Some studies support the use of rituximab [106]. The CLEAR (Concomitant Levofloxacin, Ethambutol, Azithromycin and Rifampin) regimen was found effective in a small uncontrolled observational study [107], but a recently reported double-blind, placebo-controlled trial found no difference in response rate compared to placebo [108]. The committee did not feel that current data supported a treatment recommendation for CLEAR. Repository corticotropin injection has been found to be steroid sparing in two retrospective studies [109, 110] and one prospective study [48]. However, the drug is currently quite expensive and the mechanism of action remains unclear [111]. There is a reported response to a JAK inhibitor and benefits with anti-interleukin-6 therapy in small retrospective series [112, 113]. These agents are considered by the Task Force members on a case-by-case basis when other therapies are ineffective or not tolerated.
Justification of recommendation
The evidence base of the conditional recommendation for methotrexate in symptomatic pulmonary patients at risk for mortality is summarised in supplement S2 in the supplementary material and includes a randomised trial [93]. The conditional recommendation for infliximab in symptomatic chronic pulmonary sarcoidosis not responding to other immunosuppressives, including glucocorticoids, is based on two trials summarised in supplement S2 in the supplementary material [94, 96]. The committee could not make recommendations on other drugs. Data supporting the use of some drugs is provided in the evidence to decision table in supplement S2 in the supplementary material. Figure 1 summarises the approach used by most members of committee.
Future research
Additional studies are needed to evaluate the efficacy, safety and cost efficiency of rituximab, repository corticotropin injection, anti-tumour necrosis factor (TNF) biosimilars and other immunosuppressive agents. Also, the role of antifibrotic agents such as nintedanib and pirfenidone needs to be further studied [114]. Newer end-points, including change in PET and QoL, need to be validated.
Cutaneous sarcoidosis
General considerations
Cutaneous sarcoidosis is a rare skin disease, but occurs in up to 30% of patients with sarcoidosis, and skin findings are often the initial presenting symptom [115, 116]. Skin sarcoidosis can present as a variety of non-specific clinical lesions including papules, plaques and nodules, but also less commonly as vitiligo, ulcers, alopecia or subcutaneous nodules [117, 118]. Chronic cutaneous sarcoidosis-specific lesions such as lupus pernio can be cosmetically burdensome, occasionally symptomatic and are difficult to treat [56, 119, 120]. Treatment of cutaneous sarcoidosis is usually limited to cosmetically important lesions [121]. Therapeutic decisions for cutaneous sarcoidosis are often guided by the impact of disfigurement and the extent of other organ involvement, and are limited by comorbidities that increase the risk of drug toxicity.
Recently, two specific instruments have been used in more than one trial to measure response to treatment [56, 57]. The Sarcoidosis Activity and Severity Index (SASI) provides a scale of different aspects of skin disease including erythema, induration and desquamation [56]. Both instruments have been used to assess response to treatments of cutaneous sarcoidosis [120, 122–124]. Comparison of paired photographs has also been used [120, 122]. The sarcoidosis-specific QoL instruments, the King's Sarcoidosis Questionnaire [55] and the Sarcoidosis Assessment Tool [54], both contain skin modules and should prove useful in future trials in assess QoL changes with treatment.
PICO 3: In patients with cutaneous sarcoidosis, should glucocorticoid treatment be used versus no immunosuppressive treatment?
Recommendation
For patients with cutaneous sarcoidosis and cosmetically important active skin lesions which cannot be controlled by local treatment, we suggest oral glucocorticoids be considered to reduce skin lesions. (Conditional recommendation, very low quality of evidence.)
Summary of evidence
This question was originally framed to study patients with extrapulmonary sarcoidosis treated with glucocorticoids versus no treatment. It was narrowed to study patients with cutaneous sarcoidosis when the systematic literature review revealed that this population was the focus of the preponderance of studies in this area. Clinical outcomes identified by the panel as being important included clinical remission and remission of lupus pernio.
Our systematic literature review identified 1032 potentially relevant articles; the full texts of 33 were reviewed and seven were selected [120, 125–130]. As seen in the evidence to decision table in supplement S2 in the supplementary material, most of our pre-selected outcomes were not evaluated in the trials that we studied. The two outcomes assessed were clinical remission and remission of lupus pernio, as reported by the authors.
There were no randomised trials in this area. We selected six retrospective observational cohort studies on skin sarcoidosis with different types of lesions and localisations, all of which studied at least 20 patients [125–130]. Treatment with systemic glucocorticoids was associated with improvement or remission in up to two-thirds of patients. Often, the desired effects were limited to the duration of treatment and recurrences were not uncommon upon glucocorticoid tapering, requiring additional immunosuppressive therapy. For patients with lupus pernio, a retrospective study on 54 patients showed that only 20% of patients receiving systemic glucocorticoid alone achieved complete or near-complete resolution and 50% having some improvement but requiring an average daily prednisone dose of 16 mg [120]. This study employed evaluating photographs of the lesions before and after treatment, but the assessment was retrospective and photographs were obtained at various times during therapy.
Data from additional studies
Topical glucocorticoids are generally considered to be beneficial for limited skin lesions of mild or moderate extension. However, evidence of their efficacy is scarce. In a study of 20 patients who received topical treatment including intralesional administration, only five had complete resolution and the rest had partial resolution [125]. Clobetasol or halobetasol propionate have been used especially for limited and discrete papules and plaque [131, 132]. Intralesional injections of triamcinolone acetonide may be more effective than topical preparations [133]. Topical or intralesional glucocorticoids are impractical for cases with widespread lesions [134].
Justification of recommendation
The conditional recommendation for glucocorticoids for cosmetically important skin lesions is based on the few retrospective studies which reported resolution of lesions. The short-term response was commonly seen. There was insufficient evidence to make a recommendation regarding topical glucocorticoids. While physicians are comfortable with using glucocorticoids, the risk of long-term adverse effects must always be considered.
Implementation consideration
While oral glucocorticoids were effective, prolonged use is associated with substantial side-effects. Use of steroid-sparing alternatives should be considered whenever possible, especially for chronic lesions such as lupus pernio.
Future research
With the advent of new technologies to assess skin response, the value of topical and systemic glucocorticoids should be re-evaluated. Among the new tests are standardised skin scoring techniques [56, 57]. The role of high-frequency ultrasound to assess skin lesions needs further evaluation [135].
PICO 4: In patients with cutaneous sarcoidosis, should one add other immunosuppressive treatment when treatment with glucocorticoids has not been effective?
Recommendation
For patients with cutaneous sarcoidosis who have been treated with glucocorticoids and/or other immunosuppressive agents and have continued cosmetically important active skin disease, we suggest the addition of infliximab compared to no additional treatment to reduce skin lesions. (Conditional recommendation, low quality of evidence.)
Summary of evidence
This question was originally framed to study patients with extrapulmonary sarcoidosis treated with immunosuppressive treatments compared to those receiving glucocorticoids. It was narrowed to study patients with cutaneous sarcoidosis when the systematic literature review revealed that this population was the focus of the preponderance of studies in this area. Clinical outcomes identified by the panel as being important included a validated metric for assessing cutaneous lesions (SASI score [56, 57]) and QoL metrics (Short Form-36 (SF-36) Physical Component Summary and SF-36 [136]).
Our systematic literature review identified 980 potentially relevant articles. The full texts of 91 articles were reviewed. We identified five prospective controlled studies of patients with cutaneous sarcoidosis randomised to either an immunosuppressive agent or continuing glucocorticoid that had quantitative data amenable to extraction [95, 124, 137–139]. We identified two prospective, randomised controlled studies that compared the use of infliximab to glucocorticoid to treat cutaneous sarcoidosis and provided data concerning our selected outcomes [124, 138]. Baughman et al. [124] demonstrated a statistically significant improvement in the SASI desquamation index in patients treated with infliximab compared to glucocorticoid alone. In an additional study, an extrapulmonary organ severity tool (ePOST) was used to assess individual organ involvement [138]. The ePOST tool was useful as a broad assessment of each organ, but it was not specific for skin involvement.
Data from additional studies
Two randomised trials using drugs targeted against TNF other than infliximab failed to show benefit for treating cutaneous sarcoidosis. One was for golimumab [95] and the other was for thalidomide [137]. The latter study used different end-points than a previous positive open-label trial of thalidomide for cutaneous sarcoidosis [140]. Adalimumab (also a monoclonal antibody against TNF) has also been studied in one double-blind, placebo-controlled trial and was found to be more effective than placebo for chronic cutaneous sarcoidosis [139]. This study was not abstracted for analysis because only qualitative data were available. Future studies are needed to explore the clinical benefit of adalimumab.
Other treatments have been used for cutaneous sarcoidosis that have not been studied in prospective, randomised controlled studies. There has been an open-label prospective trial of treatment for sarcoidosis using chloroquine [141]. The positive response to chloroquine has been confirmed by other case series, many of which included hydroxychloroquine instead of chloroquine [104, 125, 142]. Methotrexate has been reported as effective in treating cutaneous disease in several series for both adults and children [99, 143–145]. There has been an open-label prospective trial of treatment for sarcoidosis with apremilast [122]. The positive response to apremilast has not been confirmed by either case series or another clinical trial. There have been no clinical series reporting on the use of azathioprine, leflunomide or mycophenolate mofetil specifically for cutaneous sarcoidosis. These drugs have been reported as useful for chronic sarcoidosis [44–46, 102]. However, none of these drugs has been specifically studied in cutaneous sarcoidosis, so we are unable to make recommendations regarding their use.
We identified one additional study that examined the CLEAR regimen instead of an immunosuppressive agent and compared this to placebo to treat patients with cutaneous sarcoidosis [123]. Both an intention-to-treat and a per-protocol analysis demonstrated a statistically significant improvement in the SASI score with CLEAR treatment. The CLEAR trial was a single-masked study performed at one centre and has not been confirmed. However, a subsequent larger double-blind, placebo-controlled trial of CLEAR for pulmonary disease found no evidence of effectiveness of this regimen [108]. The committee did not feel that current data supported a treatment recommendation.
Justification of the recommendation
Two small, prospective, randomised controlled studies demonstrate improvement in sarcoidosis cutaneous lesions as assessed by the SASI score with treatment by infliximab compared to continued glucocorticoid and other immunosuppressants alone in patients with cutaneous sarcoidosis [94, 124]. Infliximab is an immunomodulatory agent with a risk of adverse effects including increased susceptibility to infection, although adverse events were low in the analysed studies. The balance of effects would lead most patients to favour the use of infliximab. The stepwise approach to the management of cosmetically important cutaneous sarcoidosis is shown in figure 2.

Stepwise approach to the management of cosmetically important cutaneous sarcoidosis. Use of apremilast and tofacitinib should be on a case-by-case basis. This figure is a combination of the recommendations made in this guideline and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. #: assess need for treatment as discussed in text. GC: glucocorticoid.
Implementation considerations
Barriers to use of infliximab include the expense of treatment, the availability of facilities for parenteral administration of the agent and the potential of adverse effects. Some patients might wish to avoid agents that require parenteral administration.
Future research
The skin is an easy organ to assess, resample and biopsy. This makes it a useful target for evaluating new therapies in sarcoidosis. It is important to show whether changes in the skin reflect other organ involvement.
Cardiac sarcoidosis
General considerations
Cardiac involvement is apparent at presentation in 2–5% of unselected patients [146]. However, autopsy studies and the systematic evaluation of patients with chronic sarcoidosis with magnetic resonance imaging (MRI) suggest possible involvement in 25–30% [147, 148]. Manifestations of cardiac sarcoidosis include atrioventricular conduction delay, His-Purkinje system conduction block, ventricular and supraventricular tachydysrhythmias, and cardiomyopathy [149]. Table 4 lists variables that indicate a higher risk for cardiac events in various cohorts and should be considered as factors in the decision about whether or not to treat cardiac sarcoidosis [150–159]. Specific recommendations have been made regarding the management of cardiac sarcoidosis, mostly in terms of the management of arrhythmias [160–162].
Prognostic variables that may influence treatment decisions for cardiac sarcoidosis
PICO 5: In patients with clinically relevant cardiac sarcoidosis, should glucocorticoids with or without other immunosuppressives versus no immunosuppression be used?
Recommendation
For patients with evidence of functional cardiac abnormalities, including heart block, dysrhythmias or cardiomyopathy, we recommend the use of glucocorticoids (with or without other immunosuppressives). (Strong recommendation, very low quality of evidence.)
Summary of evidence
For this PICO, the clinical outcomes included: improvement, worsening/progression (defined by several findings AND clinical judgement), changes in cardiac PET, changes in cardiac MRI, arrythmias, QoL and toxicity [155, 163–165]. Our systematic literature review identified 996 potentially relevant articles; the full texts of 33 were reviewed and 17 were selected [67, 150, 153, 155, 157, 158, 166–176]. The data included retrospective studies specifically examining the effect of glucocorticoid treatment versus no treatment and association studies that included glucocorticoid therapy as a covariate predictor of various cardiac outcomes. No study that specifically assessed the effects of glucocorticoid therapy enrolled patients prospectively or systematically with sufficient rigour to directly compare the outcomes; all studies were subject to substantial risk-of-channelling bias or other unmeasured confounders. However, the available data suggest that the risks of important composite cardiac end-points were reduced, with hazard ratios ranging from 0.33 to 0.78. Many of the end-point events were driven by appropriate defibrillator or antiarrhythmic therapies, which were inferred (but not proven) to be equivalent to the prevention of sudden cardiac death. Nonetheless, the bulk of the studies evaluated outcomes deemed likely to be of critical importance to affected patients.
Data from additional studies
Heart block is often an early sign of cardiac involvement and it may be the manifestation with the best chance of responding to glucocorticoids [167, 177]. The optimal dose and duration of immunosuppressive therapy are unknown. A retrospective analysis suggested that prednisolone doses higher than 0.5 mg·kg−1 were no more effective than a starting dose of 0.5 mg·kg−1 [178]. It is likewise unclear whether pulse intravenous methylprednisolone is useful and for whom should it be considered [179]. Some data suggest that earlier initiation of glucocorticoids confers better cardiac outcomes [165]. Similarly, one retrospective case–control study found that withdrawal of glucocorticoids after initiation of treatment, regardless of clinical improvement, was associated with worse outcomes [180].
Glucocorticoids may lead to significant morbidity [181]; therefore, early initiation of steroid-sparing medications should be considered [4]. However, for cardiac sarcoidosis, the evidence to support steroid-sparing medications is poor and subject to all the aforementioned biases. The most commonly described steroid-sparing agents were methotrexate, azathioprine, mycophenolate mofetil, leflunomide and cyclophosphamide [154, 155, 182]. In most of the studies, the patients treated with steroid-sparing agents had no better outcomes that those treated with glucocorticoid monotherapy, but a single-centre retrospective study comparing the addition of methotrexate to prednisone versus prednisone alone suggested improved ejection fraction and brain natriuretic peptide after 5 years of treatment [164]. Anti-TNF antibodies may be useful for refractory disease [183, 184].
Justification of the recommendation
The level of evidence to support treatment approaches for cardiac sarcoidosis was very low, with multiple potential confounders and biases inherent in the available studies [149, 185]. Much of the data supporting the use of glucocorticoids is indirect, originating in association studies where glucocorticoid treatment is a covariate among other outcome predictors [185]. There is likewise minimal description in the available studies of the indications for glucocorticoid treatment or the characteristics of the treated versus untreated patients. The risk of death from cardiac sarcoidosis is high, especially for those with reduced left ventricular function [153]. Since glucocorticoid treatment has been associated with improvement in left ventricular ejection [155, 165], the Task Force members concluded that the danger associated with cardiac sarcoidosis favoured glucocorticoid treatment for clinically relevant cardiac sarcoidosis [5, 186]. There was insufficient evidence to make a recommendation regarding other immunosuppressants, but the Task Force members still consider such treatment to minimise the toxicity of glucocorticoids. Figure 3 summarises the approach used by most Task Force members.

Approach to cardiac sarcoidosis. This figure is a combination of the recommendations made in this guideline and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. #: use of implanted cardioverter defibrillator recommendation adapted from the Heart Rhythm Society [160, 162]; ¶: clinically relevant cardiac sarcoidosis is defined as rhythm disturbances, heart failure or high risk for sudden cardiac death; +: infliximab and adalimumab are usually used in combination with second-line agents. GC: glucocorticoids.
Future research
An area of current uncertainty is the management of asymptomatic patients with concerning imaging features, such as late gadolinium enhancement, fluorodeoxyglucose uptake, T2 prolongation or impaired global longitudinal strain, even when cardiac function is preserved and electrical abnormalities are absent [163, 187].
Other issues include the optimal dose of glucocorticoid, duration of treatment and role of steroid-sparing medications. There is an urgent need to develop and validate reliable biomarkers and imaging features for the assessment of treatment response.
Neurologic disease
General considerations
Sarcoidosis can affect any portion of the nervous system. Symptomatic neurosarcoidosis occurs in 5–20% of sarcoidosis patients [146, 188, 189]. Although most sarcoidosis deaths are from pulmonary disease, neurosarcoidosis is an important cause of death and deaths from neurosarcoidosis occur at a younger age [190–192]. Neurosarcoidosis may affect the cranial nerves, brain, leptomeninges and peripheral nerves. The clinical manifestations of symptomatic neurosarcoidosis often have a significant deleterious impact of the sarcoidosis patient's QoL, and include facial nerve palsy, optic neuritis, aseptic meningitis, serious sequelae from central nervous system granulomatous mass lesions, hydrocephalus and encephalopathy/psychosis [191, 193].
PICO 6: In patients with neurosarcoidosis, should immunosuppressive treatment be used versus no immunosuppressive treatment?
Recommendations
Recommendation 1: For patients with clinically significant neurosarcoidosis, we recommend treatment with glucocorticoids. (Strong recommendation, very low quality of evidence.)
Recommendation 2: For patients with neurosarcoidosis that have been treated with glucocorticoids and have continued disease, we suggest the addition of methotrexate. (Conditional recommendation, very low quality of evidence.)
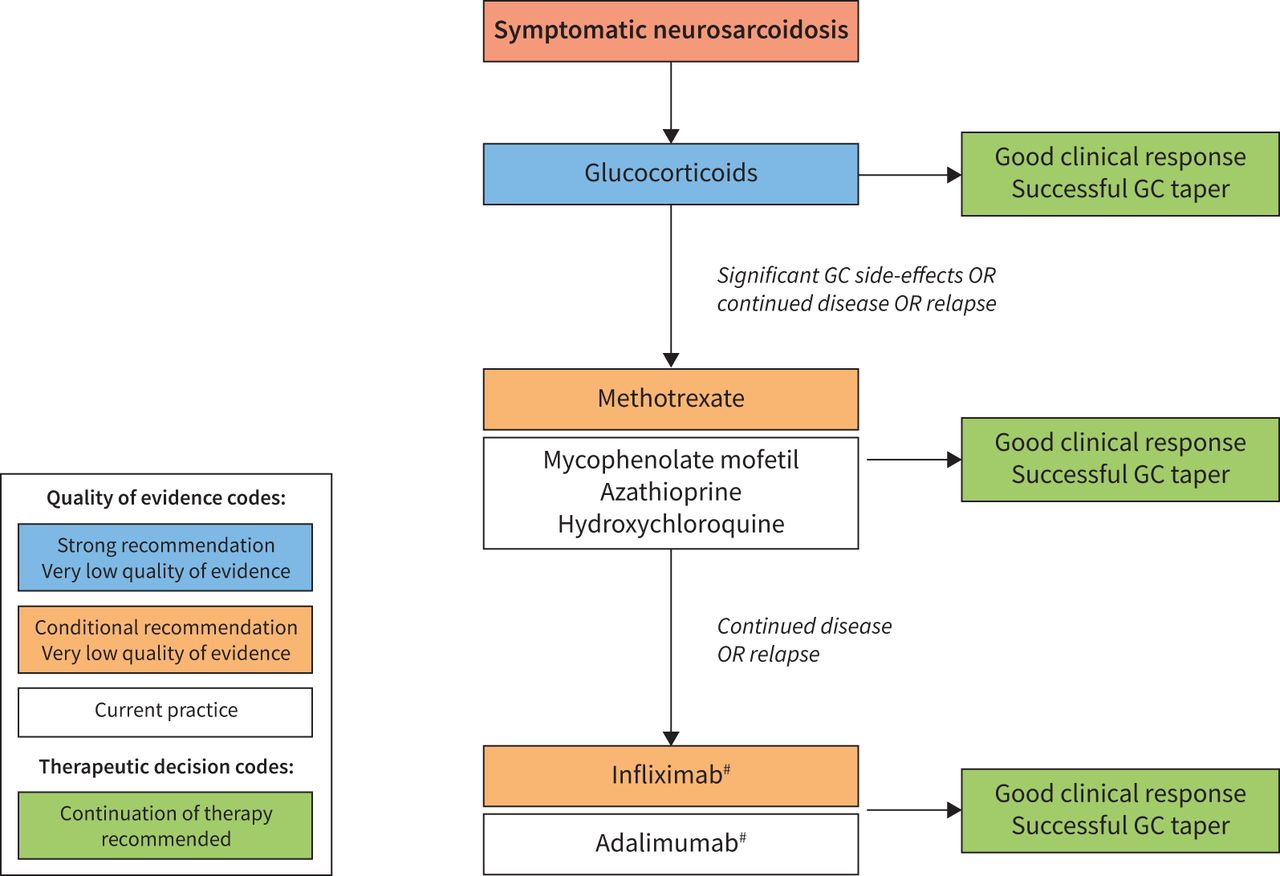
Recommendation 3: For patients with neurosarcoidosis that have been treated with glucocorticoids and a second-line agent (methotrexate, azathioprine, mycophenolate mofetil) and have continued disease, we suggest the addition of infliximab. (Conditional recommendation, very low quality of evidence.)
Summary of evidence
The clinical outcomes that were evaluated were: improvement, worsening/progression (defined by several findings AND clinical judgement), QoL and toxicity. Our systematic literature review identified 1305 potentially relevant articles; the full texts of 56 were reviewed and four were selected [35, 191, 194, 195].
One retrospective analysis of 234 neurosarcoidosis patients [191] found that although treatment with glucocorticoid alone significantly lowered the overall relapse rate of sarcoidosis compared to no treatment (hazard ratio 0.59, 95% CI 0.39–0.90; p=0.01), the specific rate of neurosarcoidosis relapse was not significantly affected (hazard ratio 0.68, 95% CI 0.38–1.23; p=0.2). Additional drugs besides glucocorticoids were found to significantly lower the relapse rate of neurosarcoidosis in this cohort (see the following data section) and most of these drugs were used in combination with glucocorticoids; this suggests glucocorticoids may have contributed to protecting against neurosarcoidosis relapse in these cases. In a meta-analysis of 1088 neurosarcoidosis patients [194], glucocorticoids were initiated as first-line therapy in 434 out of 539 (81%) treated patients and a favourable outcome was reported in 161 out of 227 (71%, 95% CI 65–77%) patients who only received glucocorticoid. We believe that these data, although limited, support the use of glucocorticoids as first-line therapy for neurosarcoidosis.
Joubert et al. [191] demonstrated that infliximab statistically significantly lowered the rate of overall sarcoidosis relapse (hazard ratio 0.31, 95% CI 0.11–0.82; p=0.02), but failed to demonstrate a statistically significant lower relapse rate of neurosarcoidosis (hazard ratio 0.16, 95% CI 0.02–1.24; p>0.05). A retrospective report demonstrated good neuroimaging and functional outcomes in 66 neurosarcoidosis patients treated with infliximab-containing regimens [35].
Data from additional studies
Reports of treatment of neurosarcoidosis consist of the second-line agents methotrexate, azathioprine and mycophenolate mofetil as well as antimalarial drugs and cyclosporine A. These drugs are usually added to glucocorticoid treatment when glucocorticoids are ineffective or a relapse occurs after tapering. These drugs may be used concomitantly with glucocorticoids as part of the initial treatment of neurosarcoidosis. The evidence for these agents is also sparse, with the possible exception of methotrexate [196]. An analysis from one institution found a statistically significant reduction in the relapse rate of neurosarcoidosis with methotrexate (hazard ratio 0.47, 95% CI 0.25–0.87; p=0.02) and hydroxychloroquine (hazard ratio 0.37, 95% CI 0.15–0.92; p=0.03), but not with azathioprine (hazard ratio 1.88, 95% CI 0.69–5.14; p=0.22) or mycophenolate mofetil (hazard ratio 0.58, 95% CI 0.25–1.34; p=0.20) [191]. In the previously described meta-analysis [194], treatment with methotrexate, azathioprine and hydroxychloroquine was initiated in 144 of the 539 (27%) patients who were treated for neurosarcoidosis. A favourable outcome was observed in 47 of the 85 (55%, 95% CI 45–66%) patients who received these agents and were not switched to third-line therapy. A retrospective analysis was performed concerning 40 neurosarcoidosis patients who received either methotrexate (n=32) and/or mycophenolate mofetil (n=14) as part of their treatment regimen [195]. Those who received methotrexate had a significantly lower yearly relapse rate than those who received mycophenolate mofetil (0.2 versus 0.6 relapses per year; p=0.058) and the median time to relapse was also longer in the methotrexate group (28 versus 11 months; p=0.049). To summarise the available data concerning the use of non-biologic agents for the treatment of neurosarcoidosis, the limited data support the use of methotrexate. Although the evidence for the other agents is minimal, there is inadequate evidence to state that these agents are ineffective for neurosarcoidosis. After methotrexate, we would consider azathioprine, mycophenolate mofetil or hydroxychloroquine. Although chloroquine and cyclosporine A could also be considered as potential second-line agents for neurosarcoidosis, their side-effect profile suggests that other non-biologic agents should be preferred. We are only aware of two case reports suggesting that adalimumab is beneficial for the treatment of neurosarcoidosis [197, 198]. There is low quality of evidence supporting cyclophosphamide for the treatment of neurosarcoidosis. In one study [191], intravenous cyclophosphamide statistically significantly lowered the rate of relapse of neurosarcoidosis compared to untreated patients (hazard ratio 0.26, 95% CI 0.11–0.59; p=0.001). In addition, in a retrospective series [196, 199], cyclophosphamide was found to be beneficial for neurosarcoidosis that was refractory to glucocorticoids and methotrexate. Despite the potential efficacy of cyclophosphamide for the treatment of neurosarcoidosis, we believe that infliximab and even adalimumab are more preferred based on the side-effect profiles of these agents.
Justification of recommendation
The strong recommendation for glucocorticoids for clinically significant neurosarcoidosis is based on very low quality of evidence; the committee felt the high risk for significant irreversible neurologic loss warranted the strong recommendation. The conditional recommendation for infliximab was based on two retrospective studies [35, 200] and other studies, as summarised in supplement S2 in the supplementary material.
Clinical evidence concerning the treatment of neurosarcoidosis is meagre due to the absence of any randomised controlled trial and to the wide variety of outcomes evaluated in retrospective studies (neuroimaging, remission/relapse, functional status, mortality) which evaluated different drugs. In addition, because drug trials for neurosarcoidosis have not rigorously compared specific agents against other ones, our recommendations concerning the stepwise approach to the treatment of neurosarcoidosis are based not only on efficacy data but also drug cost, side-effect profile and ease of use. Figure 4 shows the committees usual approach to treating neurosarcoidosis.

Approach to neurologic sarcoidosis. This figure is a combination of the recommendations made in this guideline, and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. #: infliximab and adalimumab are usually used in combination with second-line agents. GC: glucocorticoids.
Future research
Studies confirming the effectiveness of infliximab for neurosarcoidosis need to be performed. Studies examining whether high-dose glucocorticoids are required with infliximab as initial treatment for advanced neurosarcoidosis may help reduce the burden of glucocorticoid toxicity. These studies would require standardised outcome measures. Given the relative rarity of neurosarcoidosis, multicentre studies will most likely be required. In addition, neurosarcoidosis may not be amenable to uniform treatment decisions but may require different treatments depending both on the localisation and the severity of affection (central, peripheral or spine).
Fatigue
General considerations
Fatigue is a very common symptom in sarcoidosis (reported in up to 90% of patients) and is strongly associated with a lower QoL [201, 202]. It is not always related to organ involvement induced by sarcoidosis and may persist for many years, even after apparent remission of active granulomatous inflammation [203]. Other causes of fatigue have to be ruled out before SAF can be diagnosed [15]. These include diabetes mellitus, thyroid dysfunction, neuroendocrine disorders, mental disorders (especially depression), obstructive sleep apnoea, SFN, vitamin D deficiency (especially low 1,25-dihydroxycholecalciferol), heart failure and neurologic disease. Also, studies have shown poor agreement between physicians’ and patients’ assessment of SAF, highlighting the importance of using patient-reported outcome measures for the evaluation of effects of interventions in clinical trials and clinical practice [204].
PICO 7: In patients with sarcoidosis-associated fatigue, should immunosuppressants, neurostimulants, exercise or other treatments be used versus no treatment for fatigue?
Recommendations
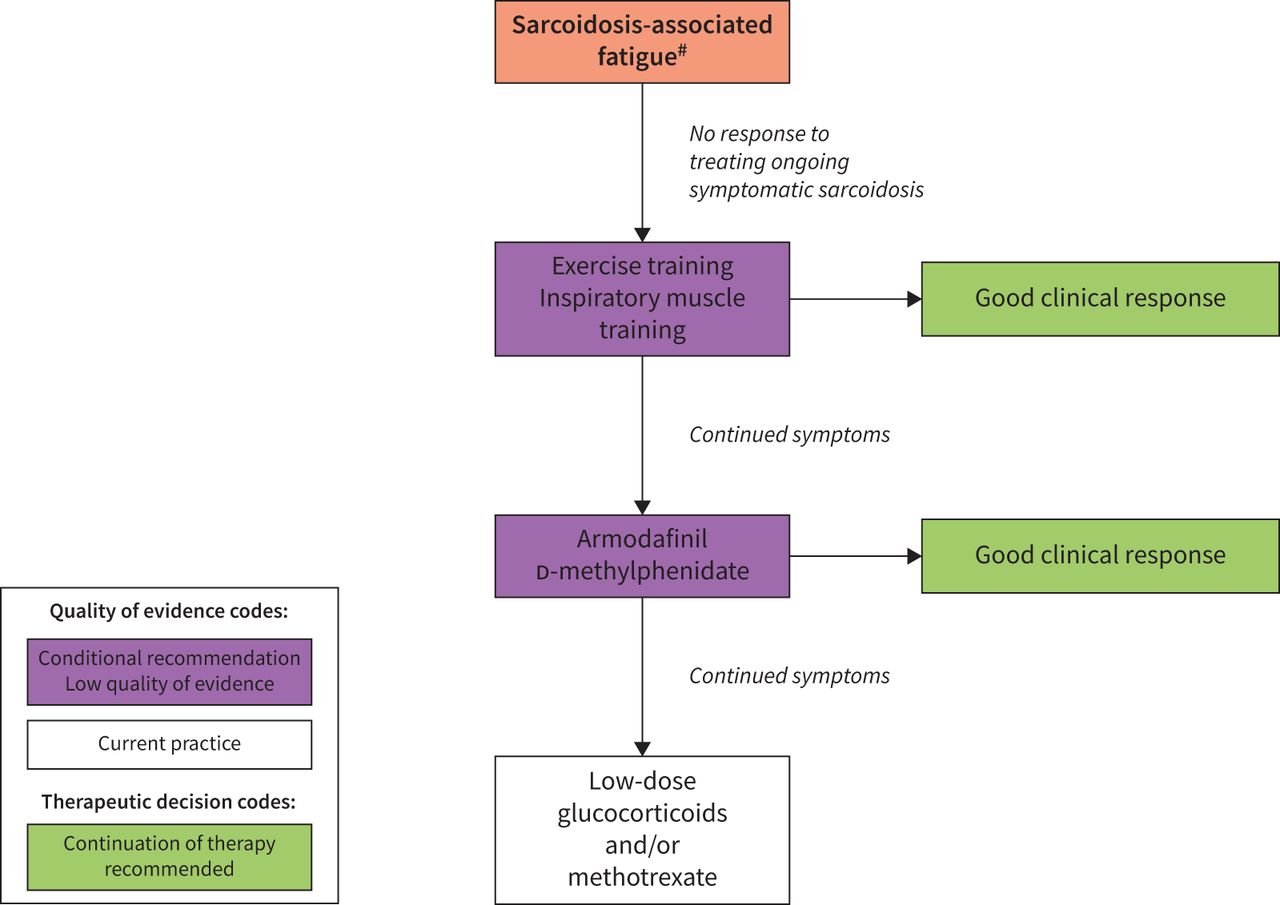
Recommendation 1: In patients with sarcoidosis who have troublesome fatigue, we suggest a pulmonary rehabilitation programme and/or inspiratory muscle strength training for 6–12 weeks to improve fatigue. (Conditional recommendation, low quality of evidence.)
Recommendation 2: In patients with sarcoidosis who have troublesome fatigue that is not related to disease activity, and after consideration of a pulmonary exercise or rehabilitation programme, we suggest the use of d-methylphenidate or armodafinil for 8 weeks to test its effect on fatigue and tolerability. (Conditional recommendation, low quality of evidence.)
Summary of evidence
Our systematic literature review of articles regarding fatigue and sarcoidosis identified 165 potentially relevant articles; the full texts of 27 were reviewed and five were selected [205–209]. One of these was of an experimental intervention not available at this time (cibinetide) [209]. The remaining four articles were reviewed.
Two of the interventions involved randomised controlled trials with physical therapist interventions. Inspiratory muscle training for 6 weeks has been studied, which led to significant improvement of the 6-min walk test (6MWT), Borg dyspnoea scale, maximal inspiratory and expiratory pressure, and Fatigue Severity Scale in the treatment group [208]. A second randomised controlled trial has tested the effect of a structured exercise programme for 12 weeks [207]. Significant effects were found on the following outcomes: 6MWT, Borg dyspnoea scale, modified Medical Research Council dyspnoea scale, maximal inspiratory force, leg strength, partial arterial oxygen pressure, and Fatigue Severity Scale and St George's Respiratory Questionnaire.
Pharmacologic interventions with neurostimulants have also been evaluated by two randomised controlled trials. Dexmethylphenidate hydrochloride (d-methylphenidate (d-MPH)) was given to 10 patients with median (range) Functional Assessment of Chronic Illness Treatment-Fatigue (FACIT-F) score of 16 (4–37) and Fatigue Assessment Scale (FAS) of 38 (22–44) in a randomised crossover trial [205]. The improvement in fatigue at 8 weeks for the d-MPH group was 36%, similar to the improvement seen in patients with cancer chemotherapy-related fatigue [210]. In that study, no difference in toxicity was noted between drug and placebo. The other randomised controlled trial investigated armodafinil 150 mg daily for 4 weeks, then 250 mg daily for 4 weeks [206]. This resulted in an improvement in fatigue as measured by the FAS and FACIT-F scores. Only 15 patients were studied. One patient withdrew because of anxiety. The adverse effects of methylphenidate and armodafinil are known from other patient populations, and include addiction, insomnia, anxiety and tachycardia [211].
Data from additional studies
Other observational studies have shown positive effects of exercise training or rehabilitation programmes on SAF and other parameters associated with reduced QoL [212–214]. One study demonstrated improvement in fatigue as well as 6MWD for those participating in pulmonary rehabilitation [215]. A recent randomised trial, published since our systematic literature review, found that rehabilitation improved fatigue [216]. This regimen was comparable to other pharmacologic interventions [217]. A recent randomised controlled trial also showed that the use of low-dose glucocorticoids has been shown to alleviate SAF, especially in the context of ongoing inflammation [218], but the committee felt there was insufficient evidence to make a recommendation regarding low-dose glucocorticoids.
Justification of recommendation
The conditional recommendations for the treatment for SAF were each supported by one prospective trial. In the cases of physical treatment intervention, one study used a sham procedure for control and the other compared patients who chose not to participate in structured training. The pharmacologic interventions were both studied in a double-blind, placebo-controlled, crossover design. However, only a limited number of subjects were studied. The approach to the evaluation and management of SAF is shown in figure 5.

Approach to the evaluation and management of sarcoidosis-associated fatigue. The use of low-dose corticosteroids with or without methotrexate should be considered on a case-by-case basis. This figure is a combination of the recommendations made in this guideline, and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. #: other causes of fatigue include diabetes mellitus, thyroid dysfunction, neuroendocrine disorders, sleep apnoea, small-fibre neuropathy, vitamin D deficiency with low 1,25-dihydroxycholecalciferol, congestive heart failure and neurologic disease.
Future research
Further research is needed to confirm the effects of inspiratory muscle training, which have been noted in a single study, and to review the impact of the recommendation regarding physical training upon costs, resources and healthcare equity. The long-term effects should also be explored, especially how improvement can best be maintained after the end of training or a systematic rehabilitation programme.
Further research is needed to confirm the effects and toxicity of d-MPH and armodafinil, which have been noted in two single-centre studies, and to review the impact of the recommendation upon costs, resources and healthcare equity. The effects of long-term use of d-MPH and armodafinil should be explored.
Small-fibre neuropathy
General considerations
Apart from idiopathic cases, SFN has been associated with various underlying conditions. SFN is a non-granulomatous disorder characterised by neuropathic symptoms and dysautonomia due to loss of thinly myelinated and unmyelinated nerve fibres. It occurs in approximately 40–60% of sarcoidosis patients, and is more prevalent in Caucasians and females [17, 219–223]. Symptoms may include paraesthesias, allodynia, numbness, pain syndromes, gastrointestinal dysmotility, diaphoresis, orthostasis, palpitations and any other symptoms associated with dysautonomia. The SFN Screening List is a validated 21-item self-administered instrument that is useful to screen for the presence of SFN-associated symptoms in sarcoidosis patients [16, 224]. There is no diagnostic gold standard for diagnosing SFN. The combination of typical symptoms and the absence of large fibre involvement is required. Once suspected, the diagnosis can be confirmed by specialised tests such as skin biopsy for intraepidermal nerve fibre density, nerve fibre density assessed by corneal confocal microscopy, quantitative sudomotor axon reflex test (QSART) and thermal threshold testing [220–223]. Due to lack of awareness among clinical physicians, the diagnosis of SFN is probably highly underreported [16, 201]. The treatment for SFN includes agents specific for the condition such as intravenous immunoglobulin (IVIg) and anti-TNF therapy as well as supportive care for neuropathic symptoms [17, 225].
PICO 8: In sarcoidosis patients with small-fibre neuropathy, should immunosuppressants or intravenous immunoglobulin be prescribed versus no treatment?
No recommendations were made for this PICO question due to a lack of sufficient evidence.
Summary of evidence
Our systematic literature review identified 427 potentially relevant articles; the full texts of nine were reviewed and four were selected. Three of these involved cibinetide [209, 226, 227], an erythropoietin analogue, which is currently not available for clinical use. The other was a large retrospective review from one centre evaluating IVIg and/or anti-TNF monoclonal antibody treatment [17]. There are no validated, widely available end-points for evaluating the effect of SFN treatment in patients with sarcoidosis [16, 219, 221]. The clinical outcomes that were evaluated in this analysis were: measures of pain, measures of SFN (QSART), skin biopsies, SFN scale, cognitive scale and confocal microscopy. We were not able to identify sufficient treatment evidence to warrant a recommendation for any commercially available agent.
Data from additional studies
Treatment of SFN depends on the underlying disease, if identified. Symptoms are often disabling and difficult to alleviate, even when the cause is identified and adequately treated, leading to high morbidity and decreased QoL [219]. Usually, only symptomatic relief of complaints can be achieved. Guidelines for neuropathic pain have been adapted from the treatment regimens developed for other causes of SFN-related pain [219, 222]. There is no consensus regarding evaluating outcome for response to specific therapy for SFN. To date, studies have evaluated improvement in the autonomic symptoms, fibre neuropathy symptoms and the related pain, and the number of small fibres in the cornea [209, 226, 227]. However, these have not been routinely applied and were not employed in retrospective reports [17, 228, 229].
A large observational study found that that 75% of patients derived symptomatic benefit from a dosing regimen of IVIg either alone or in conjunction with anti-TNF monoclonal antibody therapy. The dosing regimen was like that described for chronic inflammatory demyelinating polyneuropathy [17]. A total of 79 patients were treated with IVIg alone or with anti-TNF monoclonal antibodies and were evaluated [17, 228]. The data are limited by the absence of a defined standard for assessing treatment response, patient selection bias, differences in concomitant treatment regimens and lack of a placebo group. Thus, conclusions regarding the usefulness of IVIg are currently preliminary. Nonetheless, a significant subset of patients are observed to experience moderate to dramatic improvements in symptoms and functionality within several months of initiating treatment [228]. The putative mechanism for effectiveness of IVIg is unclear, but may relate to immunomodulatory effects [230].
TNF may be a proximate trigger for central and peripheral inflammatory cascades that are postulated to cause neuropathy, as well as sarcoidosis itself [231]. The monoclonal anti-TNF antagonists infliximab and adalimumab have been assessed in two retrospective cohorts totalling 115 patients [17, 232]. These reports suggested that SFN-associated symptoms may respond to TNF inhibition, although the magnitude of the effect is difficult to ascertain from the available data. The GG promoter variant, associated with less exuberant TNF transcription, was also associated with better outcomes in treated patients [232].
Cibinetide, previously known as ARA-290, is an innate repair receptor agonist that has anti-inflammatory and neuroprotective properties [233–235]. Cibinetide is not yet approved for any indication, so it is not the subject of a formal recommendation in these guidelines. More importantly, it is not currently commercially available. However, cibinetide is the most extensively studied and best-validated treatment to date for sarcoidosis-associated SFN. In three randomised, placebo-controlled, double-blind studies, it has been shown to reduce symptom scores and improve markers of corneal nerve fibre health over short time-frames [209, 226, 227]. Interestingly, these neuropathic benefits correlated with increases in the 6MWD, underscoring the important functional consequences of SFN [209, 227, 234].
Justification
There were no studies with sufficient results to support any specific recommendations for SFN due to sarcoidosis. However, we have presented the current practice of managing SFN, summarised in figure 6.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
An approach to small-fibre neuropathy symptoms used by Task Force members. The use of intravenous immunoglobulin (IVIg) or anti-tumour necrosis factor (TNF) antagonists should be considered on a case-by-case basis. This figure is a combination of the recommendations made in this guideline and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. GABA: γ-aminobutyric acid.
Future research
Safety and clinical effectiveness of cibinetide, IVIg, anti-TNF antibodies and other interventions for patients with sarcoidosis and SFN needs to be investigated. Development and clinical validation of accurate biomarkers and/or clinical scores to assess treatment response should be developed.
Discussion
The management of sarcoidosis can be challenging. The clinician must remember not to focus on a single manifestation, but to look at the various manifestations both initially and over time [146, 236, 237]. The outcome of the disease is variable. Some patients have a very good outcome and never require treatment [238]. Less than 10% of patients die, mostly from advanced lung disease [6, 13, 66]. For many patients, the response to anti-inflammatory treatment can readily be seen. However, recurrence of disease is common if treatment is withdrawn too soon and at least a quarter of patients require treatment for more than 2 years [28, 30, 31]. These treatment guidelines concern mainly “sarcoidosis-modifying treatment” and do not make specific recommendations regarding useful treatments such as oxygen supplementation, implantable cardiac devices or organ transplantation.
This divergence of outcomes has led to confusion about who should or should not be treated. In these guidelines, we propose that patients be treated either for risk of death and/or permanent disability (danger), or to improve QoL [65, 239]. This concept has become readily accepted in clinical practice [4]. However, the evidence for effectiveness of treatment, especially to improve QoL, is relatively weak. Recently, two sarcoidosis-specific QoL instruments have been developed [54, 55]. The impact of treatment on these instruments has been reported [48, 95, 240]. However, we still need more information before we can be confident about the impact of treatment on QoL.
The majority of studies regarding treatment of symptomatic sarcoidosis have focused on pulmonary disease [40]. However, several studies have evaluated other manifestations such as skin, heart and neurologic disease. These non-pulmonary studies were useful in answering several of the PICOs in this report. However, there was insufficient information to evaluate treatment for other extrapulmonary disease such as liver, bone or eye disease. Symptoms of SAF and SFN are well established [15, 222, 241]; however, most studies in this area have been small and usually from a single centre [17, 205, 206, 215, 227].
The report has several limitations. All authors felt there was much to do: 1) the indications for treatment remain unclear and mostly based on a case-by-case basis; 2) measurements of response to treatments are still too heterogeneous; 3) clinical trials may provide more information [136]; and 4) single end-points such as FVC or chest imaging may not be reliable, and a composite score evaluating physiology, radiology, QoL and steroid sparing may be more effective [242].
In conclusion, we do not feel these guidelines are the final word on the management of sarcoidosis. Through a systematic review of the literature, the Task Force committee identified areas where there is sufficient information to make informed recommendations based on current evidence and our clinical experience. At the same time, areas where research on this topic is lacking or is not sufficient to make recommendations were also identified. We anticipate that an update of this guideline will be needed within the next 5 years as more information becomes available.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplement 1: Individual therapies ERJ-04079-2020.Supplement_1
Supplement 2: Evidence summaries and evidence to decision tables for all PICOs ERJ-04079-2020.Supplement_2
Shareable PDF
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-04079-2020.Shareable
Footnotes
This article has supplementary material available from erj.ersjournals.com
The guidelines published by the European Respiratory Society (ERS) incorporate data obtained from a comprehensive and systematic literature review of the most recent studies available at the time. Health professionals are encouraged to take the guidelines into account in their clinical practice. However, the recommendations issued by this guideline may not be appropriate for use in all situations. It is the individual responsibility of health professionals to consult other sources of relevant information, to make appropriate and accurate decisions in consideration of each patient's health condition and in consultation with that patient and the patient's caregiver where appropriate and/or necessary, and to verify rules and regulations applicable to drugs and devices at the time of prescription.
This document was endorsed by the ERS Executive Committee on 27 May 2021, ERN-LUNG on 7 June 2021 and WASOG on 27 May 2021.
Conflict of interest: R.P. Baughman reports grants from Gilead, Genentech, Bayer, aTyr and Bellephron, grants and personal fees for consultancy from Novartis, personal fees for consultancy from Methial, grants and personal fees for consultancy and lectures from Mallinckrodt, grants and personal fees for lectures from Boehringer Ingelheim, outside the submitted work.
Conflict of interest: D. Valeyre reports personal fees for advisory board work from Boehringer Ingelheim and Roche, outside the submitted work.
Conflict of interest: P. Korsten reports grants and personal fees from GlaxoSmithKline, personal fees from AbbVie, Pfizer, Chugai, Novartis Pharma, Sanofi-Aventis, Lilly and Gilead, outside the submitted work.
Conflict of interest: A.G. Mathioudakis reports grants from Boehringer Ingelheim, outside the submitted work.
Conflict of interest: W.A. Wuyts has nothing to disclose.
Conflict of interest: A. Wells reports personal fees for lectures and advisory board work from Boehringer Ingelheim and Roche, during the conduct of the study.
Conflict of interest: P. Rottoli has nothing to disclose.
Conflict of interest: H. Nunes has nothing to disclose.
Conflict of interest: E.E. Lower reports grants from Gilead, Genentech, Bayer and aTYR, grants and personal fees for consultancy from Novartis, outside the submitted work.
Conflict of interest: M.A. Judson received grant support for his institution from Mallickrodt.
Conflict of interest: D. Israël-Biet has nothing to disclose.
Conflict of interest: J.C. Grutters has nothing to disclose.
Conflict of interest: M. Drent has nothing to disclose.
Conflict of interest: D.A. Culver reports grants and personal fees from aTyr, Mallinckrodt, Boehringer Ingelheim and Foundation for Sarcoidosis Research, personal fees from Roche, outside the submitted work.
Conflict of interest: F. Bonella reports personal fees and non-financial support from Boehringer Ingelheim, Roche, Galapagos, BMS and Savara Pharma, outside the submitted work.
Conflict of interest: K. Antoniou has nothing to disclose.
Conflict of interest: F. Martone has nothing to disclose.
Conflict of interest: B. Quadder has nothing to disclose.
Conflict of interest: G. Spitzer has nothing to disclose.
Conflict of interest: B. Nagavci acts as an ERS methodologist.
Conflict of interest: T. Tonia acts as an ERS methodologist.
Conflict of interest: D. Rigau acts as an ERS methodologist.
Conflict of interest: D.R. Oullette reports grants from PCORI (Patient-Centred Outcomes Research Institute, US Federal) and Sanofi, outside the submitted work; and has provided expert witness work for venous thromboembolic disease.
Alexander G. Mathioudakis is supported by an ERS Fellowship in Guidelines Methodology (MTF 2015-1) and by the National Institute of Health Research Manchester Biomedical Research Centre (NIHR Manchester BRC).
- Received November 4, 2020.
- Accepted May 4, 2021.
- Copyright ©The authors 2021. For reproduction rights and permissions contact permissions{at}ersnet.org
References










