





Figures
- FIGURE 1
Approach for pulmonary sarcoidosis. Use of rituximab, JAK inhibitor and repository corticotropin injection (RCI) should be on a case-by-case basis. This figure is a combination of the recommendations made in this guideline and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. #: assess need for treatment based on low risk, intermediate risk but impaired quality of life or high risk as discussed in text. GC: glucocorticoid.
- FIGURE 2
Stepwise approach to the management of cosmetically important cutaneous sarcoidosis. Use of apremilast and tofacitinib should be on a case-by-case basis. This figure is a combination of the recommendations made in this guideline and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. #: assess need for treatment as discussed in text. GC: glucocorticoid.
- FIGURE 3
Approach to cardiac sarcoidosis. This figure is a combination of the recommendations made in this guideline and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. #: use of implanted cardioverter defibrillator recommendation adapted from the Heart Rhythm Society [160, 162]; ¶: clinically relevant cardiac sarcoidosis is defined as rhythm disturbances, heart failure or high risk for sudden cardiac death; +: infliximab and adalimumab are usually used in combination with second-line agents. GC: glucocorticoids.
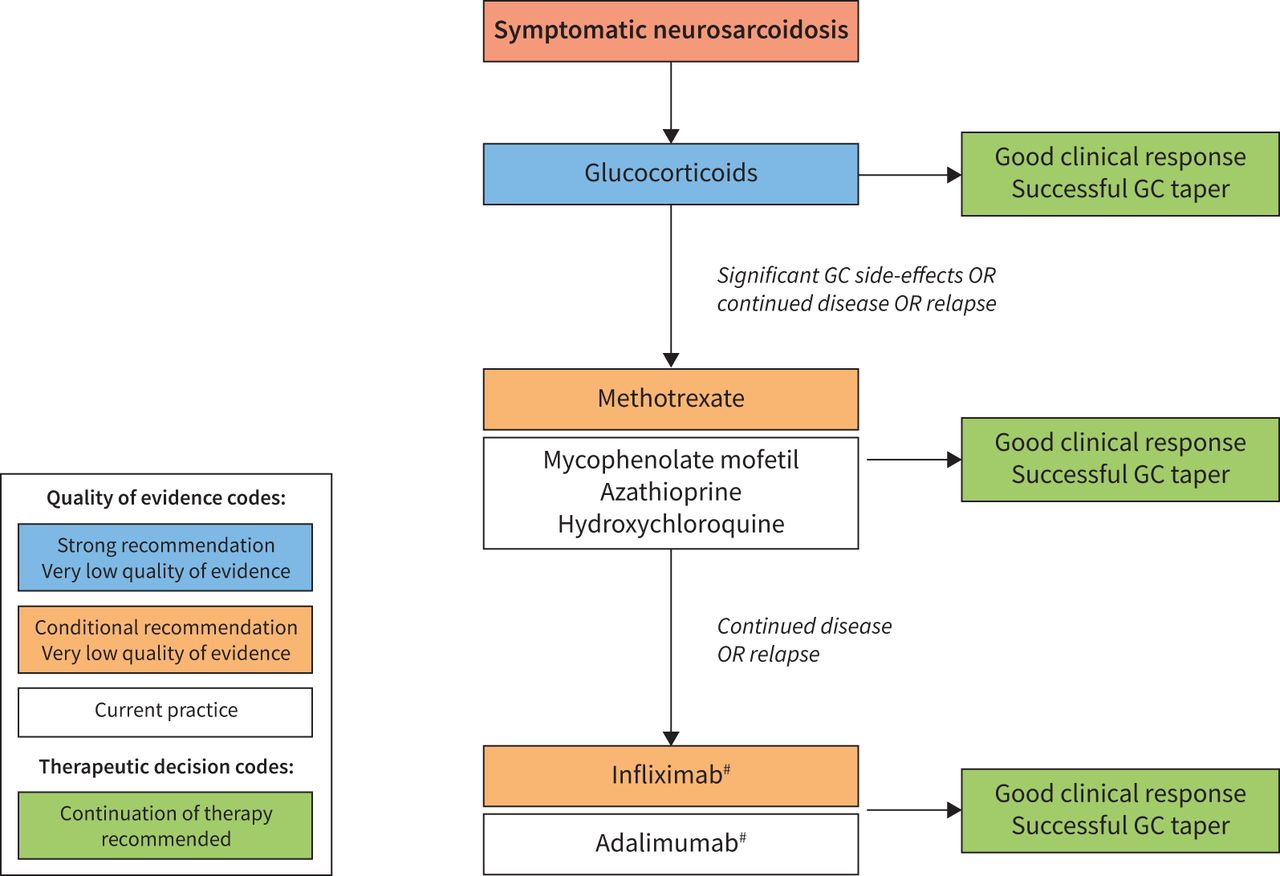
- FIGURE 4
Approach to neurologic sarcoidosis. This figure is a combination of the recommendations made in this guideline, and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. #: infliximab and adalimumab are usually used in combination with second-line agents. GC: glucocorticoids.
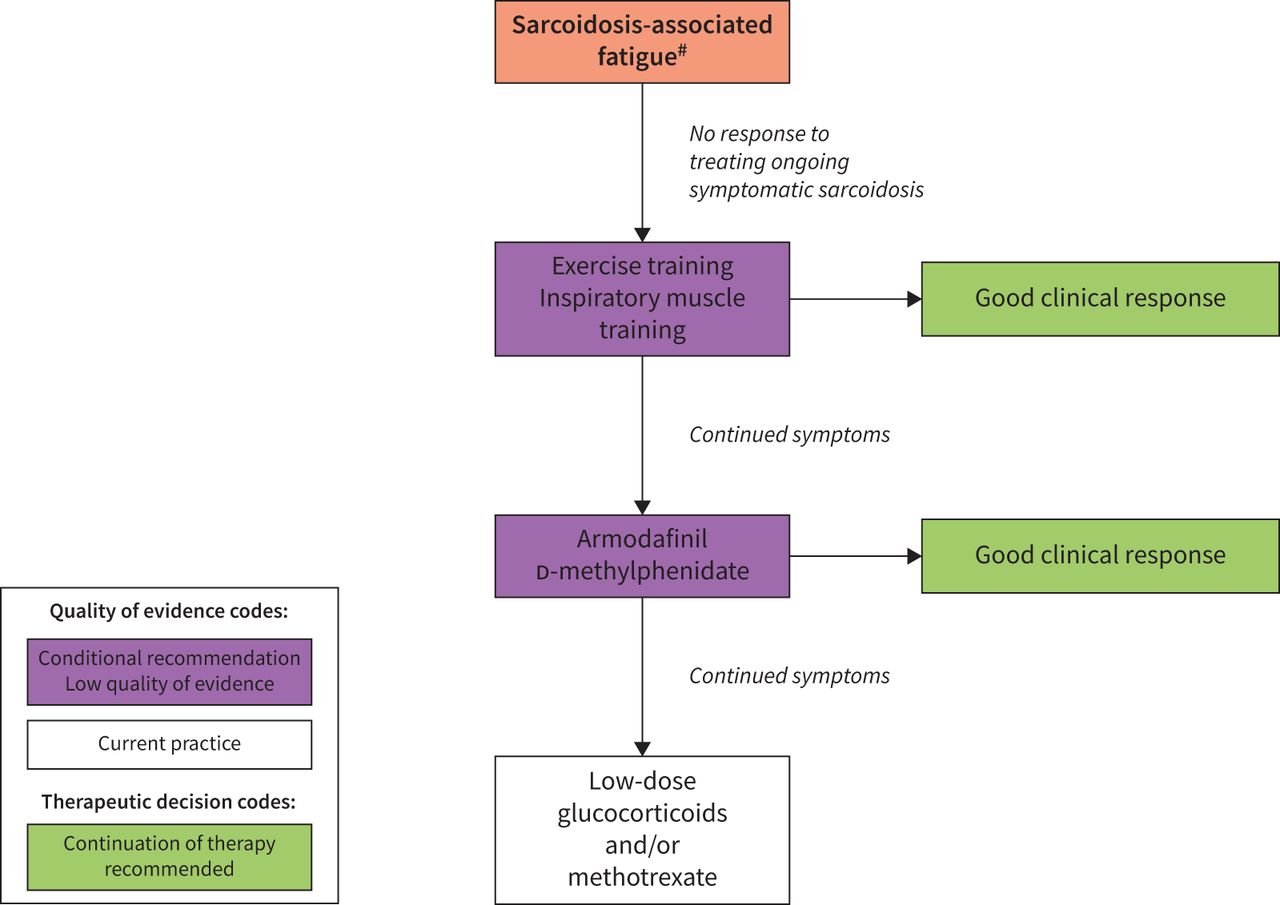
- FIGURE 5
Approach to the evaluation and management of sarcoidosis-associated fatigue. The use of low-dose corticosteroids with or without methotrexate should be considered on a case-by-case basis. This figure is a combination of the recommendations made in this guideline, and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. #: other causes of fatigue include diabetes mellitus, thyroid dysfunction, neuroendocrine disorders, sleep apnoea, small-fibre neuropathy, vitamin D deficiency with low 1,25-dihydroxycholecalciferol, congestive heart failure and neurologic disease.
- FIGURE 6
An approach to small-fibre neuropathy symptoms used by Task Force members. The use of intravenous immunoglobulin (IVIg) or anti-tumour necrosis factor (TNF) antagonists should be considered on a case-by-case basis. This figure is a combination of the recommendations made in this guideline and a description of Task Force members’ current practice in situations where there was not enough evidence to warrant a recommendation or for questions for which a systematic review of the literature was not undertaken. Note that the information depicted as current practice (in white boxes) is not intended as a recommendation for clinical practice. GABA: γ-aminobutyric acid.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Task Force recommendations
PICO question Recommendations 1) In patients with pulmonary sarcoidosis, should glucocorticoid treatment be used versus no immunosuppressive treatment? For untreated patients with major involvement from pulmonary sarcoidosis believed to be at higher risk of future mortality or permanent disability from sarcoidosis, we recommend the introduction of glucocorticoid treatment to improve and/or preserve FVC and QoL. (Strong recommendation, low quality of evidence.)
2) In patients with pulmonary sarcoidosis, should one add immunosuppressive treatment or remain on glucocorticoid treatment alone? For patients with symptomatic pulmonary sarcoidosis believed to be at higher risk of future mortality or permanent disability from sarcoidosis who have been treated with glucocorticoids and have continued disease or unacceptable side-effects from glucocorticoids, we suggest the addition of methotrexate to improve and/or preserve FVC and QoL. (Conditional recommendation, very low quality of evidence.)
For patients with symptomatic pulmonary sarcoidosis believed to be at higher risk of future mortality or permanent disability from sarcoidosis who have been treated with glucocorticoids or other immunosuppressive agents and have continued disease, we suggest the addition of infliximab to improve and/or preserve FVC and QoL. (Conditional recommendation, low quality of evidence.)
3) In patients with cutaneous sarcoidosis, should glucocorticoid treatment be used versus no immunosuppressive treatment? For patients with cutaneous sarcoidosis and cosmetically important active skin lesions which cannot be controlled by local treatment, we suggest oral glucocorticoids be considered to reduce skin lesions. (Conditional recommendation, very low quality of evidence.)
4) In patients with cutaneous sarcoidosis, should one add other immunosuppressive treatment when treatment with glucocorticoids has not been effective? For patients with cutaneous sarcoidosis who have been treated with glucocorticoids and/or other immunosuppressive agents and have continued cosmetically important active skin disease, we suggest the addition of infliximab compared to no additional treatment to reduce skin lesions. (Conditional recommendation, low quality of evidence.)
5) In patients with clinically relevant cardiac sarcoidosis, should glucocorticoids with or without other immunosuppressives versus no immunosuppression be used? For patients with evidence of functional cardiac abnormalities, including heart block, dysrhythmias or cardiomyopathy, we recommend the use of glucocorticoids (with or without other immunosuppressives). (Strong recommendation, very low quality of evidence.)
6) In patients with neurosarcoidosis, should immunosuppressive treatment be used versus no immunosuppressive treatment? For patients with clinically significant neurosarcoidosis, we recommend treatment with glucocorticoids. (Strong recommendation, very low quality of evidence.)
For patients with neurosarcoidosis that have been treated with glucocorticoids and have continued disease, we suggest the addition of methotrexate. (Conditional recommendation, very low quality of evidence.)
For patients with neurosarcoidosis that have been treated with glucocorticoids and a second-line agent (methotrexate, azathioprine, mycophenolate mofetil) and have continued disease, we suggest the addition of infliximab. (Conditional recommendation, very low quality of evidence.)
7) In patients with sarcoidosis-associated fatigue, should immunosuppressants, neurostimulants, exercise or other treatments be used versus no treatment for fatigue? In patients with sarcoidosis who have troublesome fatigue, we suggest a pulmonary rehabilitation programme and/or inspiratory muscle strength training for 6–12 weeks to improve fatigue. (Conditional recommendation, low quality of evidence.)
In patients with sarcoidosis who have troublesome fatigue that is not related to disease activity, and after consideration of a pulmonary exercise or rehabilitation programme, we suggest the use of d-methylphenidate or armodafinil for 8 weeks to test its effect on fatigue and tolerability. (Conditional recommendation, low quality of evidence.)
8) In sarcoidosis patients with small-fibre neuropathy, should immunosuppressants or intravenous immunoglobulin be prescribed versus no treatment? No recommendations were made for this PICO question due to a lack of sufficient evidence.
PICO: Patients, Intervention, Comparison, Outcomes; FVC: forced vital capacity; QoL: quality of life.
- TABLE 2
Immunosuppressive therapies for sarcoidosis
Drug Usual dosage Major toxicities Recommended monitoring Comments Prednisone/prednisolone Initial 20 mg once a day; follow-up 5–10 mg once a day to once every other day Diabetes; hypertension; weight gain; osteoporosis; cataracts; glaucoma; moodiness Bone density; blood pressure and serum glucose Cumulative toxicity Methotrexate 10–15 mg once a week Nausea; leukopenia; hepatotoxicity; pulmonary CBC, hepatic, renal serum testing Cleared by kidney, avoid in significant renal failure Leflunomide 10–20 mg once a day Nausea; leukopenia; hepatotoxicity; pulmonary CBC, hepatic, renal serum testing Cleared by kidney, avoid in significant renal failure Azathioprine 50–250 mg once a day Nausea; leukopenia; infections; malignancy CBC Mycophenolate mofetil 500–1500 mg twice a day Diarrhoea; leukopenia; infections; malignancy CBC Less experience in sarcoidosis than other agents Infliximab or biosimilars# 3–5 mg·kg−1 initially, 2 weeks later, then once every 4–6 weeks Infections; allergic reaction Screen for prior TB; monitor for allergic reactions; contraindicated in severe CHF, prior malignancy, demyelinating neurologic disease, active TB, deep fungal infections Allergic reactions can be life threatening Adalimumab# 40 mg every 1–2 weeks Infections Screen for prior TB; monitor for allergic reactions; contraindicated in severe CHF, prior malignancy, demyelinating neurologic disease, active TB, deep fungal infections Less toxic than infliximab Rituximab# 500–1000 mg every 1–6 months Infections Screen for viral hepatitis; check IgG level with chronic therapy High risk for viral reactivation; can lead to IgG deficiency RCI# 40–80 units twice a week Diabetes; hypertension; oedema; anxiety Monitor glucose and blood pressure Most of toxicity is on day of injection Hydroxychloroquine 200–400 mg once a day Loss of vision Ocular exams periodically depending on age and renal function Minimal impact on cardiac and neurologic disease More details regarding dosages, major toxicities and monitoring are given in supplement S1 in the supplementary material and adapted from prior reports [4, 39–48]. CBC: complete blood count; TB: tuberculosis; CHF: congestive heart failure; RCI: repository corticotropin injection. #: use reserved for patients who have failed prior treatments with steroids and/or antimetabolites.
- TABLE 3
Outcomes for patient care and clinical research
Measure Category Level Pulmonary sarcoidosis Patient wellbeing Physician judgement Important Clinical judgement of improvement, worsening/progression Physician judgement Critical Clinical judgement alone Treatment chest imaging: Scadding score [20], changes in Treatment imaging Important Treatment chest imaging: Muers score [49], changes in PET/CT chest imaging, changes in Scan Important Pulmonary function tests: FVC, FEV1, FEV1/FVC, DLCO, SaO2 Lung function tests Critical 6-min walk distance [50] Exercise capacity Important Quality of life Quality of life Important SGRQ [51] Short Form-36 [52] Fatigue Assessment Scale [53] SAT Lung [54] KSQ General health [55] KSQ Lung health [55] Serious AEs; life-threatening AEs AEs Critical AEs leading to discontinuation Other AEs Extrapulmonary sarcoidosis Physician global assessment Cutaneous sarcoidosis disease activity Important SASI [56] CSAMI [57] Photographs Clinical judgement of improvement, worsening/progression Physician judgement Critical Skin measure of disease Important Eye measure of disease Critical Kidney measure of disease Important Löfgren syndrome measure of disease Hypercalcaemia Critical Quality of life Quality of life Critical Fatigue Assessment Scale SAT Skin [54] SAT Fatigue [54] KSQ Dermatology questionnaire Serious AEs; life-threatening AEs AEs Critical AEs leading to discontinuation Other AEs Cardiac sarcoidosis Clinical judgement of improvement, worsening/progression Physician judgement Critical PET/CT chest imaging, changes in Treatment imaging Critical MRI chest imaging, changes in Arrythmias Arrythmias Critical Quality of life Quality of life Important Serious AEs; life-threatening AEs AEs Critical AEs leading to discontinuation Other AEs Neurosarcoidosis Measures of neurologic disease Physician judgement Critical Clinical judgement of improvement, worsening/progression Quality of life Quality of life Critical Serious AE; life-threatening AEs AEs Critical AEs leading to discontinuation Other AEs All categories Steroid sparing Steroid sparing Critical PET: positron emission tomography; CT: computed tomography; FVC: forced vital capacity; FEV1: forced expiratory volume in 1 s; DLCO: diffusing capacity of the lung for carbon monoxide; SaO2: arterial oxygen saturation; SGRQ: St George's Respiratory Questionnaire; SAT: Sarcoidosis Assessment Tool; KSQ: King's Sarcoidosis Questionnaire; AE: adverse event; SASI: Sarcoidosis Activity and Severity Instrument; CSAMI: Cutaneous Sarcoidosis Activity and Morphology Instrument; MRI: magnetic resonance imaging.
- TABLE 4
Prognostic variables that may influence treatment decisions for cardiac sarcoidosis
• Age >50 years • Left ventricular ejection fraction <40% • New York Heart Association Functional Class III or IV • Increased left ventricular end-diastolic diameter • Late gadolinium enhancement on cardiac magnetic resonance imaging • Ventricular tachycardia • Cardiac inflammation identified by fluorodeoxyglucose positron emission tomography scan • Echocardiographic evidence of abnormal global longitudinal strain • Interventricular septal thinning • Elevated troponin or brain natriuretic peptide Features found to be associated with increased risk for morbidity or mortality from cardiac sarcoidosis [150–159].
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplement 1: Individual therapies ERJ-04079-2020.Supplement_1
Supplement 2: Evidence summaries and evidence to decision tables for all PICOs ERJ-04079-2020.Supplement_2
Supplementary Material
This one-page PDF can be shared freely online.
Shareable PDF ERJ-04079-2020.Shareable










